

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Neurological disorders have become serious long-term problems that affect more than 450 million individuals worldwide. The most common forms of neurological diseases include cognitive and cerebrovascular diseases, which lead to significant impairment in the activities of daily living (ADL) and consequently decrease the quality of life, especially in the elderly.1 Alzheimer's disease (AD) constitutes 69% of dementia cases in those older than 75 years, and is characterized by gradual loss of cognitive, affective, and ADL capabilities.2 Vascular dementia (VaD) is the second most common dementia,3 and is characterized by decline in memory and executive functions. Mild cognitive impairment (MCI) precedes clinically evident dementia,4 which has minimal-to-mild cognitive impairment that does not significantly impact the ADL. Although the age-standardized mortality rate of ischemic stroke (IS) has clearly decreased in recent years, stroke is still one of the leading causes of death and disability in Japan.5 The complexity of blood as a source of biomarkers is reflected in the limitations of various proteomic techniques, but these may still allow the detection of the above four diseases earlier than when using classically recognized markers.
Omega-3 polyunsaturated fatty acids (ω-3 PUFAs) can inhibit hepatic triglyceride synthesis, reduce platelet aggregation, cause vascular relaxation, and reduce inflammation.6 Eicosapentaenoic acid (EPA, 20:5n-3) and docosahexaenoic acid (DHA, 22:6n-3) are ω-3 PUFAs that have shown beneficial effects on brain functions through improving episodic memory and learning functions in healthy adults.7 EPA and DHA are useful clinical biomarkers for identifying whether the fatty-acid balance in the body is optimal or suboptimal. Reptin is essential for systemic viability and plays antagonistic roles in tissue growth and regulation of the tumor metastasis suppressor gene; several studies have found that it is overexpressed in certain types of cancer, including hepatocellular carcinoma and colorectal cancer.8 Adiponectin, a hormone that is secreted solely by adipocytes, exerts significant effects on atherogenesis, endothelial function, and vascular remodeling via the modulation of signaling cascades in cells of the vasculature. A plasma adiponectin concentration of less than 4.0 µg/mL was associated with a twofold increase in the incidence of coronary artery disease, and adiponectin is a useful marker for identifying individuals at risk of developing metabolic syndrome and early-stage atherosclerosis.9
Inflammation may contribute to cognitive decline and dementia. Higher levels of high-sensitivity C-reactive protein (hsCRP), a biomarker of inflammation, were associated with worse performance in cognitive tests after stroke.10 Serum amyloid A (serum AA) is an acute-phase protein that acts as a biomarker of inflammation, and previous studies have produced data on the local production of serum AA proteins in histologically normal, atherosclerotic, AD, inflammatory, and tumor tissues.11 Lipid biomarkers are frequently used to assess the risk of cardio-cerebrovascular disease, such as high-density lipoprotein (HDL) and low-density lipoprotein (LDL). HDL performs a wide range of functions, including antioxidation, anti-inflammation, and proendothelial functions and the modulation of immune function.12 High levels of LDL lead to atherosclerosis, which increases the risks of heart attack and IS.13
The aim of the present study was to determine the different expression levels of and associations between plasma fatty acids (EPA and DHA), adiponectin and reptin, plasma markers of inflammation (hsCRP and serum AA), plasma lipids (HDL and LDL), and peripheral arterial tonometry among AD, MCI, VaD, and IS patients and normal controls. Data on these different expression levels may represent useful information for analyzing the different pathological mechanisms underlying these diseases.
Go to : 
METHODS
Participants
This was a retrospective case–control study performed in the outpatient clinic of Okayama University Hospital and affiliated hospitals from April 2011 to April 2016 that investigated AD (n=295), MCI (n=47), VaD (n=34), and IS (n=200). Two hundred and thirty age- and sex-matched individuals in whom no neurological or psychiatric diseases were found in medical examinations were included as normal controls (102 males and 98 females).
The clinical information on the normal controls and the patients is summarized in Table 1. A diagnosis of AD was established based on clinical criteria and diagnostic guidelines as described previously.14 MCI was diagnosed according to the well-known Petersen's criteria. VaD was diagnosed based on recommendations of the Neuroepidemiology Branch of the National Institute of Neurological Disorders and Stroke and the Association Internationale pour la Recherche et l'Enseignement en Neurosciences. IS was diagnosed by neurologists based on the clinical history, general physical and neurological examinations, and ancillary tests such as radiological examinations (CT/MRI), according to the WHO Monitoring of Trends and Determinants in Cardiovascular Disease projects.15

Ethical permission for this study was provided by the Ethics Committee on Epidemiological Studies of the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences (approval #777), and written informed consent was obtained from all participants prior to enrollment.
Serological laboratory tests
Blood samples were collected in the fasting state. Serological data for EPA, DHA, adiponectin, reptin, hsCRP, serum AA, HDL, and LDL were obtained from 696 participants (normal controls, n=130; AD, n=266; MCI, n=44; VaD, n=33; IS, n=200). Serum samples were analyzed for routine biochemical parameters immediately after collection, while aliquots of the samples were also stored at −20℃ for subsequent assays of EPA, DHA, adiponectin, reptin, and serum AA. EPA and DHA were assayed using gas chromatography/mass spectrometry. Adiponectin, reptin, and serum AA were assayed by solid-phase sandwich ELISA using commercial kits.
Statistical analysis
Continuous demographic and clinical data are presented as mean±SD values in Table 1. Statistical analyses were performed using standard statistical software (SPSS 22.0, IBM Corp., Armonk, NY, USA). After checking for normality, we performed Kruskal-Wallis tests to compare eight serum data values (EPA, DHA, adiponectin, reptin, hsCRP, serum AA, HDL, and LDL) between the normal controls and the four disease groups. Differences with a probability value of p<0.05 were considered statistically significant.
Go to :
RESULTS
Participant characteristics
The demographic and clinical features of the normal controls and the four disease groups (AD, MCI, VaD, and IS patients) are presented in Table 1. The sex ratio was well matched across these five groups, and the age of the participants was mainly concentrated around the mid-70s.
Plasma fatty-acid changes
The serological tests indicated that the EPA levels were significantly lower in AD and IS patients than in the normal controls (Fig. 1A). On the other hand, DHA was remarkably lower in the four disease groups than in the normal controls (Fig. 1B). However, neither EPA nor DHA differed among the four disease groups.
 | Fig. 1Plasma fatty-acid levels in the normal controls and the four disease groups: AD, MCI, VaD, and IS. Intergroup comparisons of EPA (A) and DHA (B) levels. *p<0.05, †p<0.01 vs. normal. AD: Alzheimer's disease, DHA: docosahexaenoic acid, EPA: eicosapentaenoic acid, IS: ischemic stroke, MCI: mild cognitive impairment, VaD: vascular dementia.
|
Reptin and adiponectin changes
The reptin level was significantly higher in the AD and IS patients than in the normal controls (Fig. 2A), while the adiponectin level was significantly lower in the IS patients than in the AD and MCI patients (Fig. 2B). The reptin/adiponectin ratio was significantly higher in the IS patients than in the normal controls and the AD, MCI, and VaD patients (Fig. 2C), with no significant difference among the latter four groups.
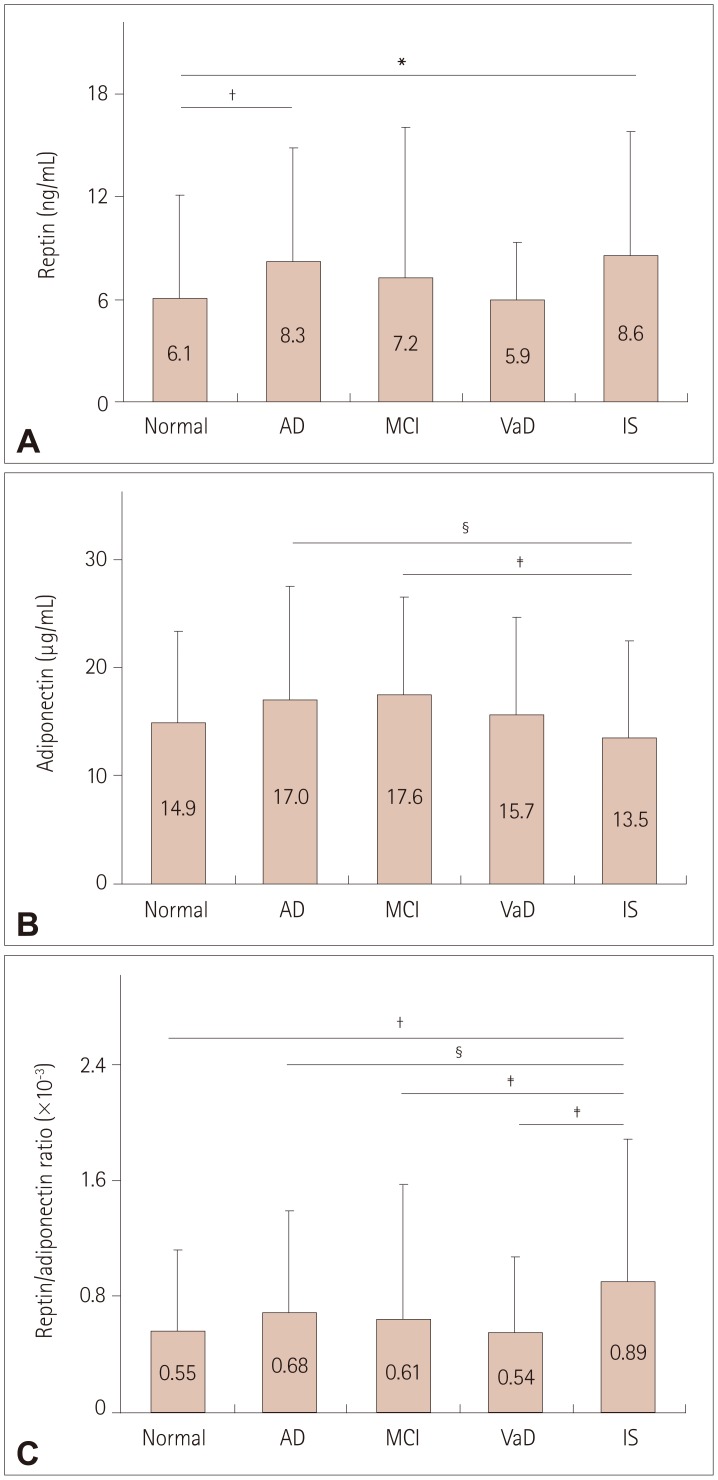 | Fig. 2Comparison of reptin (A), adiponectin (B), and reptin/adiponectin ratio (C) levels in the normal controls and the four disease groups. *p<0.05, †p<0.01 vs. normal, ‡p<0.05, §p<0.01 within the disease groups. AD: Alzheimer's disease, IS: ischemic stroke, MCI: mild cognitive impairment, VaD: vascular dementia.
|
Plasma markers of inflammation changes
The hsCRP level was significantly higher in the VaD and IS patients than in the normal controls (Fig. 3A), and higher in the VaD than the AD patients. The serum AA level was significantly higher in the four disease groups than in the normal controls (Fig. 3B), with no difference among the four disease groups.
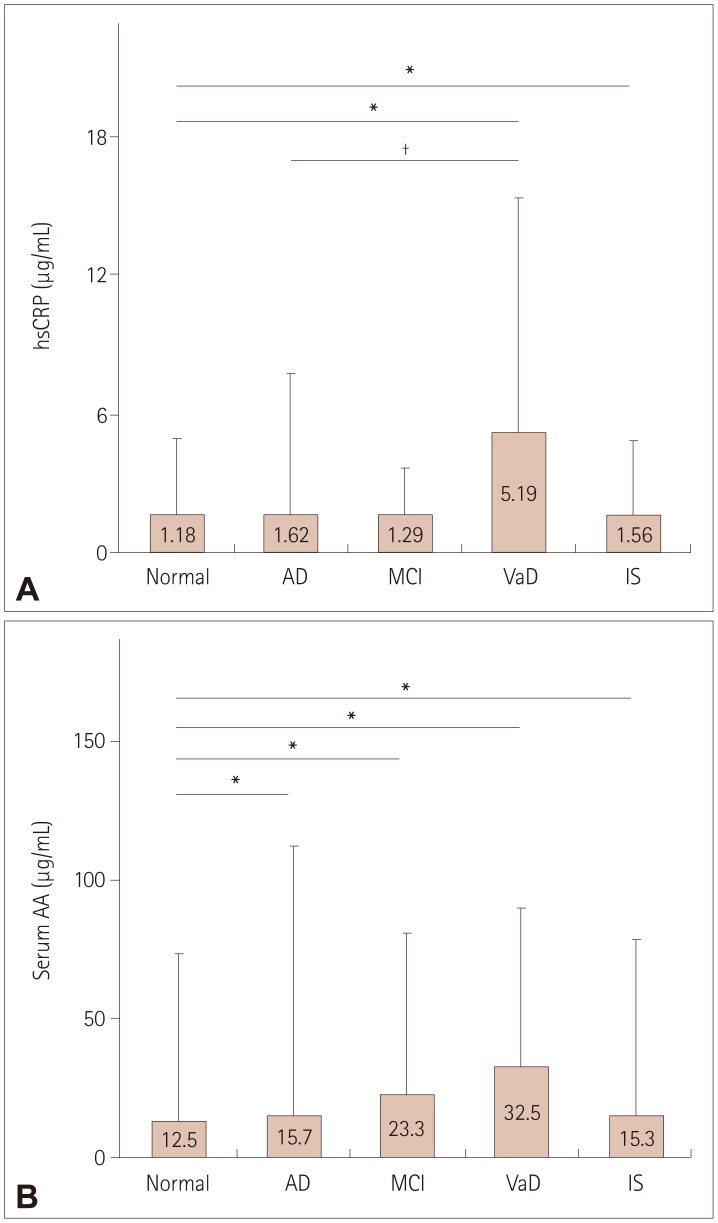 | Fig. 3Levels of plasma markers of inflammation in the normal controls and the four disease groups. Intergroup comparisons of hsCRP (A) and serum AA (B) levels. *p<0.01 vs. normal; †p<0.05 within the disease groups. AD: Alzheimer's disease, hsCRP: high-sensitivity C-reactive protein, IS: ischemic stroke, MCI: mild cognitive impairment, serum AA: serum amyloid A, VaD: vascular dementia.
|
Plasma lipid levels and peripheral arterial tonometry analyses
The HDL level did not differ significantly between the normal controls and the four disease groups, but it was significantly lower in the AD and IS patients than in the MCI patients (Fig. 4A). The LDL level was significantly higher in the AD and IS patients than in the normal controls (Fig. 4B), and higher in the IS than the MCI patients.
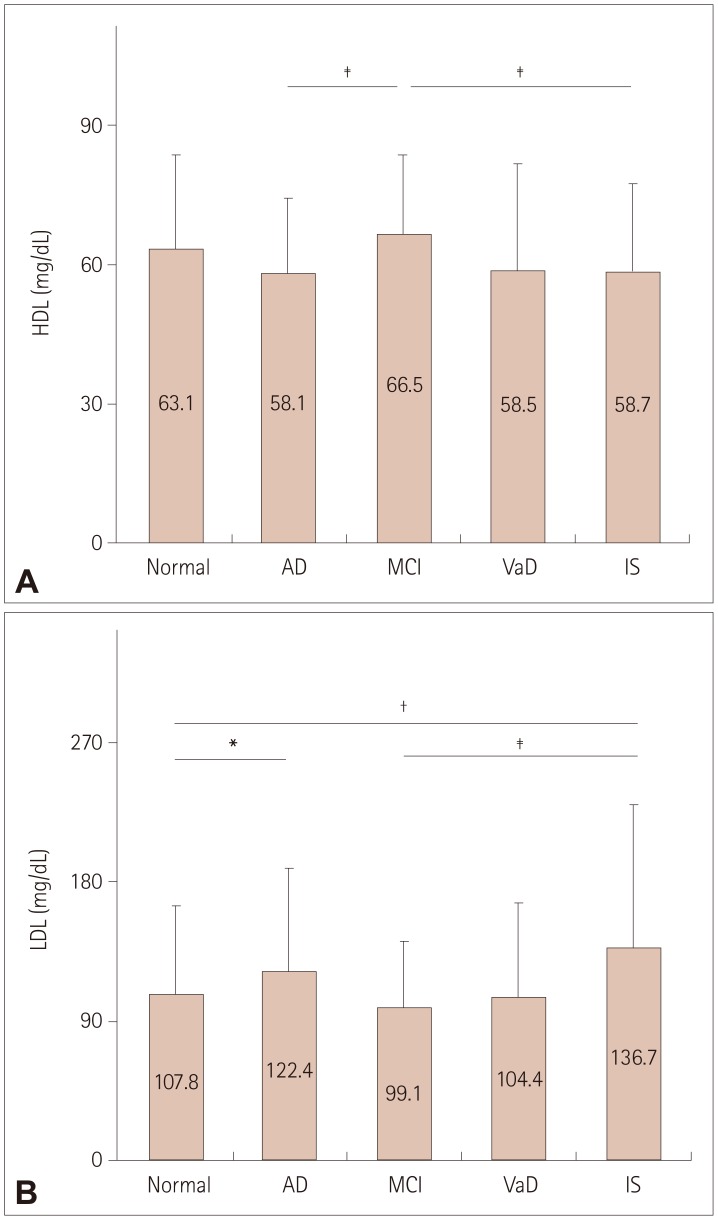 | Fig. 4Plasma lipid levels in the normal controls and the four disease groups. Intergroup comparisons of HDL (A) and LDL (B) levels. *p<0.05, †p<0.01 vs. normal, ‡p<0.05 within disease groups. AD: Alzheimer's disease, HDL: high-density lipoprotein, IS: ischemic stroke, LDL: low-density lipoprotein, MCI: mild cognitive impairment, VaD: vascular dementia.
|
Go to :
DISCUSSION
Blood-based biomarkers span a massive dynamic range of proteins in blood, but their use in clinical diagnostic practice is still far from optimal despite considerable research into their diagnostic utility in discriminating cognitive and cardiovascular diseases. In this study we examined differences in the expression levels of several plasma biomarkers in elderly AD, MCI, VaD, and IS patients and elderly normal controls, and found differences in expression levels that are indicative of the diverse pathological mechanisms underlying these diseases.
Dietary habits have changed during the last decade, especially in Western countries, with decreases in the intake of ω-3 PUFAs.16 EPA and DHA are considered the most important ω-3 PUFAs, having anti-inflammatory, antioxidant, antiatherogenic, antiamyloid, and neuroprotective properties in the brain.17 Higher intakes of EPA and DHA are associated with lower risks of AD and IS.18 The present study found that the plasma EPA level was lower in AD and IS patients, while the DHA level was markedly lower in all four disease groups (Fig. 1). These data indicate that both EPA and DHA were associated with AD and IS, while DHA is more strongly associated than IS with memory tasks.
Reptin is involved in the regulation of gene transcription, remodeling of chromatin, DNA damage sensing and repair, and tumor biology.19 Higher adiponectin levels have been associated with cognitive decline,20 and the present study found that a higher reptin level was associated with AD and IS (Fig. 2A). Similar to a previous study,21 we found that the adiponectin level did not differ significantly between the normal controls and the four disease groups, while it was lower in IS patients than in AD and MCI patients (Fig. 2B). A recent study has shown that dramatic increases in serum adiponectin in AD are positively correlated with the severity of dementia, which is due to an elevated level of adiponectin being associated with amyloid β-peptide toxicity, inflammatory reactions, and programmed cell death in the AD brain. In contrast, a cross-sectional study found that the adiponectin level was unaltered in AD patients.22 The actions of adiponectin in the central nervous system are still poorly understood, but it does play a protective role against atherosclerotic vascular change and exerts a cerebroprotective effect via an endothelial nitric oxide synthase-dependent mechanism, and the loss of these effects enhances endothelial dysfunction in IS patients.23 Hypoadiponectinemia is concomitantly involved in the pathogenesis of atherosclerosis in subjects with cerebral infarction,24 which might reflect a close relationship between adiponectin-metabolic-syndrome inflammation and the development of atherosclerosis.25 The present study is the first to find a strong association between the reptin/adiponectin ratio and IS (Fig. 2C), which suggests that IS is associated with high levels of DNA damage and repair in cells besides inflammation.
While hsCRP may be a risk factor for cognitive impairment,26 the present results suggest that the hsCRP level is associated with VaD and IS but not with AD (Fig. 3A). Some studies have emphasized the importance of serum AA in inflammation, atherosclerosis, thrombosis, AA-induced amyloidosis, rheumatoid arthritis, and neoplasia.11 Our results indicated that the serum AA level was significantly increased in AD, MCI, VaD, and IS (Fig. 3B). These data suggest that the hsCRP level is mainly associated with primary vascular diseases such as VaD and IS, and that the serum AA level is more generally associated with cognitive diseases and IS.
HDL modulates cognitive function in aging and age-related neurodegenerative disorders.12 High plasma levels of HDL can protect against IS.27 In the present study, the HDL level did not differ significantly between the normal controls and the four disease groups (Fig. 4A), which is probably due to the large amount of fish include in the Japanese diet.28 On the other hand, the LDL level was significantly higher both in AD and IS (Fig. 4B), which supports previous reports.29 Endothelial dysfunction is an early predictor of IS, and the reactive hyperemia index (RHI) is correlated with the risk of IS and cognitive dysfunction.30 Although the differences were not significant, the present study found a tendency for RHI to be lower in the four disease groups than in the normal controls.
This study was subject to several limitations. First, this study had a retrospective case–control design and was performed within a small area of Japan. Second, relatively few patients and controls were included, especially in the MCI and VaD groups, which had the effect of producing relatively wide SD values for the VaD group. Finally, subtypes of IS were not analyzed separately.
In summary, the present study is the first to compare differences between plasma biomarkers in elderly AD, MCI, VaD, and IS patients and elderly normal controls. The findings suggest that lower EPA and DHA levels and higher reptin and LDL levels are both associated with AD and IS, the reptin/adiponectin ratio is strongly associated with IS, the hsCRP level is more strongly associated with VaD and IS, and the serum AA level is associated with all three cognitive diseases and IS.
Go to :
 XML Download
XML Download