

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Accurate knowledge of the positions of facial foramina becomes important for diagnostic and clinical procedures such as the administration of regional anaesthesia, orthognathic, and cleft surgeries, and other invasive procedures in the maxillofacial region [123]. These facial foramina transmit neurovascular bundles between the cranium and facial region. The nerves that emerge from these foramina are blocked at their exits to induce local anesthesia during various maxillofacial and cosmetic surgical procedures [4]. Traumatic or iatrogenic injury to the neurovascular bundles at the point of emergence through these foramina may result in bleeding and hypoesthesia or paraesthesia or even anaesthesia in the region of supply depending on the degree of the injury [35].
The supraorbital notch and foramen (SON/F) in the frontal bone transmit the supraorbital neurovascular complex, containing the supraorbital nerve and vessels. The supraorbital nerve is given off by the frontal nerve, which is the largest branch of the ophthalmic division of the trigeminal nerve [6]. The supraorbital artery is a branch of the ophthalmic artery, which in turn arises from the internal carotid artery. The supraorbital vessels and nerve, supply the skin of the forehead, scalp, upper eyelid, and nose [6]. The supraorbital nerve, solely a sensory nerve, supplies sensory innervation to a considerably large area including, the upper eyelid, forehead and scalp as far as the lambdoidal suture, and thus, a prime candidate for a regional nerve block. The supraorbital neurovascular bundle is frequently encountered in a multitude of surgical procedures such as open and endoscopic brow lift and other cosmetic facial surgeries, and when performing the supraorbital nerve block. An understanding of the anatomy of the orbitofrontal region is of profound importance for the identification and preservation of these structures during surgery.
According to the descriptions in standard anatomy textbooks, the SON/F is present at the junction of the medial one third and lateral two-thirds of the supraorbital margin [6]. However, most published studies in the recent literature have demonstrated that significant variations exist in the occurrence, form and position of the supraorbital nerve exits through the frontal bone [1789101112131415]. Attempts have also been made to identify satisfactory references for localizing the SON/F. Evidence has shown clear variation in the relative position of the supraorbital nerve exits to surgically important reference points among different population groups such as Thai, Korean, Kenyan, White, Black, and the Japanese [1101112131415]. Further, population specific linear measurements from surgically important landmarks have a clinical implication as it might help precise localization of SON/F, thus avoiding injury to the neurovascular bundle that exits through this notch or foramen during surgery or administration of anaesthesia.
Limited availability of literature for localization of the precise position of SON/F in the Sri Lankans together with marked population variations raises the necessity to evaluate the location of SON/F in the local population. Hence, the present study was undertaken to ascertain the morphological characteristics of the SON/F and its relative position in relation to surgically important anatomical landmarks.
Materials and Methods
Supraorbital nerve exits from 116 sides of 58 dry adult skulls of known gender (37 male and 21 female) constituted the study material. The skulls were collected from the Division of Anatomy, Faculty of Dental Sciences, and the Department of Anatomy, Faculty of Medicine, University of Peradeniya, Sri Lanka. Approval from the institutional ethical committee was obtained before pursuing the study (number FDS-FRC/2014/06). The skulls of known sex with no apparent gross pathology, deformity, or traumatic lesions were included in the study. The skulls with damage in the orbital and nasal cavity region and those of less than 18 years of age were excluded. Both sides of the skulls were visually assessed and the presence, type (foramen or notch), and number of exit points of the supraorbital neurovascular bundle were determined. The relative position of the SON/F in relation to the infraorbital foramen (IOF) was recorded as lying in the same vertical plane as the IOF or lying lateral or medial to this plane.
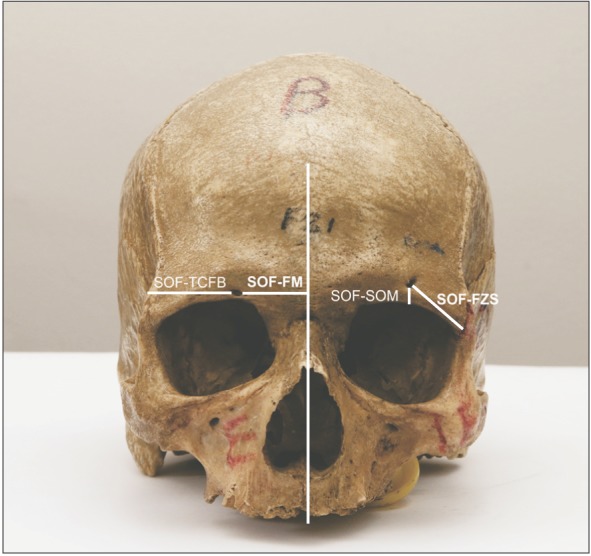
In order to analyze the size and the relative position of the supraorbital notch (SON) or supraorbital foramen (SOF), the following parameters (Fig. 1) on the right and left sides were measured using a digital vernier caliper to the nearest 0.01 mm (Mitutoyo Corporation, Japan) after aligning the skull in the Frankfurt horizontal plane:
- The maximum transverse diameter of the SOF
- The maximum vertical diameter of the SOF
- The vertical distance from the inferior margin of the SOF to the superior orbital margin, in a line parallel to the facial midline
- The distance from the medial margin of the SON/F to the facial midline (FM), in a line perpendicular to the facial midline (SON/F-FM)
- The distance from the lateral margin of the SON/F to the temporal crest of the frontal bone (TCFB), in a line perpendicular to the facial midline (SON/F-TCFB)
- The distance from the lateral margin of the SON/F to the frontozygomatic suture (FZS)
All measurements were recorded by one investigator. To minimize the intraobserver error three repeated measurements were made for each observation at different sittings and the average of the three measurements was taken for further analysis. Results were expressed as means and standard deviations, and analyzed using the SPSS ver. 19 (IBM Corp., Armonk, NY, USA). A comparison of the mean values between sides and genders was performed using the t test. P<0.05 was considered statistically significant.
Results
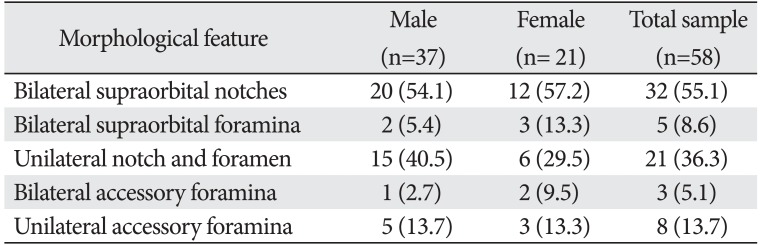
Supraorbital exits were present in the form of a notch or foramen in all 116 sides of skulls examined. The SON (72.4%) was present more frequently than a SOF (27.6%). Accessory supraorbital foramina were seen in 11 (18.9%) skulls (Table 1). In three of the 58 skulls, accessory foramina were present bilaterally. In one female skull, bilateral double accessory foramina were found. The position of the accessory supraorbital foramina relative to the main SON/SOF was lateral in 56.4% of the sides, medial in 31.3% and superior in 12.5%. Of the skulls investigated, 55.1% displayed bilateral supraorbital notches, whereas 8.6% had bilateral supraorbital foramina, and 36.3% had a notch on one side and a foramen on the contralateral side (Table 1).
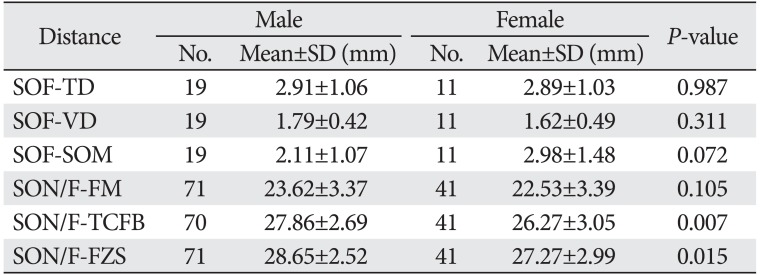
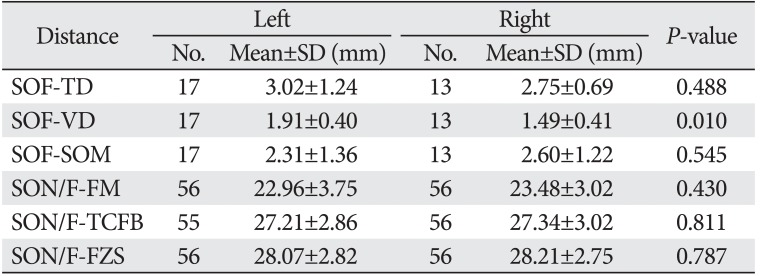
The dimensions of the supraorbital foramen and the linear measurements from the SON/F to various anatomical landmarks with respect to the sexes and sides are summarized in Tables 2 and 3, respectively.
The comparison between the measurements of the males and females revealed that the size of the SOF and linear distances from the SON/F to anatomical landmarks were larger in males than in females. However, the differences were statistically significant only for the distances from the SON/F to the temporal crest (P<0.01), and SON/F to the FZS (P<0.05) (Table 2). Further, the observed parameters were greater on the right side than those on the left side. However, none of the differences were statistically significant (P>0.05).
The left SOF had larger dimensions than the right SOF. A statistically significant difference between the left and right side was observed for the vertical diameter of SOF (P<0.05).
The position of the SOF in relation to the position of IOF is presented in Table 4.
It is evident that the majority of supraorbital foramina (80.2%) are located medial to the vertical plane passing through the IOF. Both SON/F and IOF were located in the same vertical plane in 14.9% and in 5.0% of skulls the SON/F were located lateral to the IOF.
Discussion
Numerous studies have examined the exit points of the supraorbital nerve and vessels in various populations [789101112131415]. The exit point may appear as a notch or a foramen. In the present study of adult crania of Sri Lankans, the supraorbital passage was found more frequently as a notch (72.6% and 70.9% on the right and left side, respectively) than as a foramen (27.4% and 29.1% on the right and left side, respectively), a result which is consistent with observations reported in previous studies [11011]. Previous studies have shown an incidence of the SON ranging from 47.50% to 92.5% [1911121416]. The frequency of SOF has been reported to vary from 8% to 51% in different populations [17]. The presence of the supraorbital exit as a foramen rather than as a notch has a clinical implication. In the event of a foramen, the supraorbital neurovascular bundle is relatively fixed in position to the cranium and therefore more likely to be stretched during retraction [9]. Further, it will be encountered at a much higher position relative to the superior orbital rim and thus merits caution, in these populations where the incidence of SOF is high.
Typically, all fibers of the SON exit through the SON/F. However, some fibers may leave the nerve within the orbit and exit separately through accessory exits. The occurrence of accessory supraorbital nerve exits is well documented in the literature [10111718]. A wide variation in the occurrence of accessory nerve exits among different populations has also been reported [10]. The occurrence of accessory supraorbital exits in the present study was found to be 18.9%. Among other studies, Gupta [18] has found them in 14% of skulls whereas Saylam et al. [8] have observed them 21.2% of skulls. Ashwini et al. [11] observed them in 66.25% of cases which is a much higher incidence than reported in other studies. As to the location of these accessory exits, in the present study, a majority of them (56.4%) were found lateral to the main SON/F. This observation is consistent with the findings of some previous studies [1118]. Gupta [18] observed 84.6% of them lateral to the main SON/F while in a study done by Ashwini et al. [11], 62.22% and 50% of accessory nerve exits on the right side on left side respectively, were located lateral to the main SON/F. The existence of accessory nerve exits has a clinical implication. It explains the cause of incomplete analgesia or anaesthesia as the branches passing through these exits may escape during a regional nerve block of SON. Furthermore, accessory nerve exits raise a mark of caution, as there is a potential risk of iatrogenic injury to the nerve fibers passing through them during surgery in this region of the face, with resultant sensory deficits.
In the present study, the occurrence of bilateral supraorbital notches was higher than the occurrence of bilateral supraorbital foramina, a result which is in agreement with previous studies [31011]. Bilateral supraorbital notches were seen in 55.1% of skulls (54.1% in males, 57.2% in females) whereas 8.6% (5.4% in males and 13.3% in females) had bilateral supraorbital foramina, and 36.3% (40.5% in males and 29.5% in females) had a notch on one side and a foramen on the contralateral side. In a study on Caucasians, Malet et al. [3], observed bilateral notches in 65% of skulls, bilateral foramina in 20.0%, and a notch on one side and a foramen on the contralateral side in 10.0% of skulls. Apinhasmit et al. [10] who examined Thai skulls, observed bilateral notches in 50%, bilateral foramina in 17%, and a notch on one side and a foramen contralaterally in 33% of skulls. In a study conducted by Cheng et al. [9] in a Chinese population, bilateral notches were observed in 40.2%, bilateral foramen in 24.8%, and notch on one side and foramen on other in 24.8%. It is clearly evident that there is a wide variation in the form of supraorbital exits among different population groups. The neurovascular bundle may exit through a notch, or a foramen located well above the supraorbital margin, and a combination of a notch and a foramen may exist in the same skull. This fact indicates that locating the SON/F by palpation alone is not sufficient and not reliable [11]. Hence, localizing the SON/F with reference to palpable anatomical landmarks is more accurate and reliable.
Numerous studies have documented various soft tissue [1920] and bony landmarks [1591011121621] that would define a safe zone during surgical procedures in the supraorbital region. The facial midline is the widely used bony landmark to predict the location of the SON/F [15910111214161821]. A wide variation has been documented in the position of the supraorbital nerve exit with regard to various anatomical landmarks in different population groups [591011121621]. According to Cheng et al. [9] in the Chinese population the median distance between the supraorbital exits and the facial midline was 24.56 mm. In their study, 80% of the supraorbital exits were found to lie between 20.77 mm and 30.52 mm from the facial midline. In another study, Webster et al. [7] reported that the distance from the SON/F to midline varied between 15 to 38 mm with an average of 32.02 mm. In the present study, in addition to the facial midline, we utilized the temporal crest of the frontal bone and the frontozygomatic suture to localize the SON/F.
The present study supports the presence of gender differences in the position of SON/F as reported in previous studies on different populations [9101216]. The linear distances from all selected landmarks were greater in males than in females, and the distances from the SON/F to the FZS, and TCFB showed statistically significant differences between the genders. This dimorphism in relation to gender is not unusual as similar gender differences have been reported in other parts of the craniofacial complex [22]. Thus, the present findings together with the findings of previous studies [101216] suggest that gender should be taken into account during localization of SON/F.
Previous studies have reported that the position of the SON/F in relation to FM, TCFB, and FZS display side related differences [916]. The present study did not demonstrate any significant differences between the left and right-sided measurements (Table 3). In a study done on the Chinese population, statistically significant right-left asymmetry has been reported in the location of the SOF relative to the superior orbital rim [9]. In a Brazilian population, Chrcanovic et al. [16] demonstrated statistically significant differences between the left and right sided distances of SON/F-FM and SON/F-TCFB. However, in studies done by Agthong et al. [12] and Apinhasmit et al. [10] on Thai skulls, Barker et al. [5] on Caucasian skulls, Singh et al. [23] and Ashwini et al. [11] on Indian skulls, side related differences were statistically not significant.
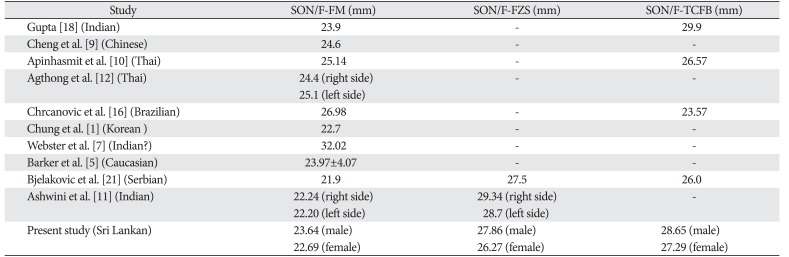
The mean distances of the supraorbital passage to the facial midline, temporal crest of the frontal bone and frontozygomatic suture in diverse population groups are summarized in Table 5. It is evident from the data presented that the distance from the facial midline to the SON/F shows a wide variation, and varies from 21.9 to 32.02 mm. Although the facial midline of the skull has been reported as a useful landmark in localizing the SON/F, Cutright et al. [14] reported that the intraoperative identification of this line could be difficult. Further, it was stated that the temporal crest of the frontal bone which can be palpated at the anterior border of the temporalis muscle would be a more reliable landmark for intraoperative localization of the supraorbital nerve and vessels. In their study, the mean distance of the SON/F to the temporal crest of the frontal bone was 2.6 cm. In the present study, in addition to the facial midline, we utilized both the frontozygomatic suture and the temporal crest of the frontal bone to localize the supraorbital exits.
The standard texts in Anatomy cite that both the supraorbital and infraorbital foramina are located on the same sagittal plane [6]. Although this is in concurrence with some populations, it disregards a mass of evidence with reference to other positions of the SON/F exits described in different studies [110]. Such diversity in the location of supraorbital foramen may be attributed to ethnic factors [114]. According to the results of the present study, the majority of supraorbital notches and foramina (80.2%) were located medial to the IOF. Five per cent were located laterally, and only 14.9% of the sides displayed both SON/F and IOF in the same sagittal plane. Previous studies too have demonstrated a predominance of SON/F to be located medially to the IOF [110].
In conclusion, this study demonstrated a wide range of variation in the exit points of the supraorbital neurovascular bundle, among genders and population groups. The frequency of occurrence of notches and foramina and accessory foramina, and the position of SOF in the Sri Lankan varied from other populations. This information and the method to localize the foramen utilizing easily palpable anatomical landmarks introduced in this study would be useful to clinicians during surgery of the orbital region in a Sri Lankan population.

 XML Download
XML Download