

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
There are several anomalies of the main pancreatic duct and pancreatic parenchyma. Pancreas divisum—failure of fusion of the dorsal and ventral pancreatic ducts—is relatively well known as the most common congenital anomaly of the pancreatic duct [1], of with an incidence approximately 10% of all embryos. During the prenatal period, the major pancreatic duct is drained by the dorsal duct via the minor papilla and the minor pancreatic duct by the ventral duct via the major papilla. However, in adults, this setting is reversed, and 70% of the pancreas is drained by the ventral duct.
There is a rare anomaly similar to pancreas divisum in which doubled ducts are formed. Unlike pancreas divisum, these separate 2 ducts are laid from the pancreatic tail to neck. As these separated ducts lie in the pancreas parenchyma, the parenchyma are separated from each other; the ducts generally join at the pancreas head and drain via the major papilla. This condition is a rare developmental anomaly called pancreas bifidum or bifid pancreas or fish tail pancreas. Most cases are detected incidentally by MRI or endoscopic retrograde cholangiopancreatography (ERCP) and do not generally cause symptoms. The course of pancreas bifidum formation and development is unclear. In this report, we describe a patient with pancreas bifidum who had two separated ducts within the pancreas from tail to neck but did not have a separated parenchyma.
CASE REPORT
A 73-year-old man with chronic hypertension, benign prostate hyperplasia, and hyperlipidemia visited a local clinic due to fever in June 2016. Blood tests showed increased liver enzymes and inflammation, and he was hospitalized for 28 days. Abdominal CT scans and upper gastrointestinal endoscopy were performed for further evaluation, and he was diagnosed with a suspicious mixed-type intraductal papillary mucinous neoplasm (IPMN), and he was referred to our center for further evaluation.
Following preoperative work-up, surgery was postponed for several days due to continuous infection and mild kidney injury. The kidney injury was induced by colistin administered for multidrug-resistant Acinetobacter baumannii. After kidney function recovered, pancreaticoduodenectomy was performed. Following resection of the pancreas neck in front of the portal vein, we found 2 pancreatic ducts in the remnant pancreas body. Since the superior duct was smaller than the inferior duct, we considered it to be a minor duct of pancreas divisum. However, we were surprised to find that both ducts were opened from the pancreas tail (Fig. 1). We sutured and ligated the superior duct with 5-0 Prolene. The rest of surgery was routinely performed.
Following surgery, the patient experienced a postoperative pancreatic fistula on postoperative day 5 and drainage color changed from serous to sanguineous—called a sentinel sign [2]—on postoperative day 8. Suspicious contrast leakage was found at the stump of a gastroduodenal artery (GDA) by emergent CT scan and angiography confirmed a pseudoaneurysm of a GDA stump. Emergent stent-graft placement was performed (Fig. 2). The patient recovered and was discharged on postoperative day 24. The pancreatic fistula was controlled and drainage was removed. Final pathological diagnosis was confirmed as IPMN-associated invasive marginal-free carcinoma and two lymph node metastases were found in 12 lymph nodes.
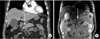
Following patient recovery and discharge, we reviewed the surgical records and preoperative images. In preoperative CT and MRI, we found 2 ducts within the pancreas tail to body (Fig. 3). These doubled-ducts were joined in the pancreas head and flowed into the ampulla of Vater. The diameters of the superior and inferior ducts were 2.81 mm and 4.87 mm, respectively. As endoscopic retrograde biliary drainage was inserted preoperatively, the diameter of ducts was smaller than this size in the operation room. When we first found 2 ducts in the remnant pancreas, we thought it was a type of pancreas divisum. As a general pancreas divisum can be recognized by accessory duct that opened to minor papilla, the specimen was rechecked, but there was no additional opening that could be called minor papilla.
DISCUSSION
At the time, we were unaware of the pancreas bifidum condition. Pancreas bifidum is identified by the division of the pancreatic tail into separate dorsal and ventral buds. It is an extremely rare congenital branching anomaly of the main pancreatic duct. It is also usually benign and incidentally detected on MRI or ERCP and manifests as a duplication of the major duct in the body of the pancreas.
There have been a few cases reported on pancreas bifidum. Dinter et al. [3] reported a female patient who had lung cancer with bony metastasis. The patient had no symptoms and bifid pancreas was detected by abdominal CT for cancer evaluation. Another case reported a patient who underwent pylorus preserving pancreaticoduodenectomy based on a presumptive diagnosis of periampullary malignancy [4]. The author of this report also did not predict the presence of 2 ducts. In this report, the surgeon performed a double duct to mucosa pancreaticojejunostomy.
There are no currently established procedures to follow in the case of this anomaly, like as postoperative pancreatic fistula is not definitively preventative yet. We hope that this report helps pancreatic surgeons to have a knowledge of pancreas bifidum and helps them to be prepared for this anatomical variant.


 XML Download
XML Download