

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
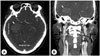
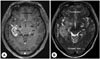
Phantosmia is defined as the false perception of odors without any environmental odor stimulus. It is a very rare phenomenon, but it can be caused by a wide variety of conditions, such as viral or allergic rhinosinusitis, head trauma, brain tumor, migraine, temporal lobe epilepsy, stroke, and psychiatric conditions. If it is caused by a brain tumor such as glioblastoma, it can be controlled with steroids or antiepileptic drugs. Phantosmia can also be treated with surgical resection or adjuvant radiotherapy combined with chemotherapy. We report a case of glioblastoma presenting with phantosmia.
Figures and Tables
References
1. Jion YI, Grosberg BM, Evans RW. Phantosmia and Migraine With and Without Headache. Headache. 2016; 56:1494–1502.

2. Morrissey DK, Pratap U, Brown C, Wormald PJ. The role of surgery in the management of phantosmia. Laryngoscope. 2016; 126:575–578.
3. Landis BN, Burkhard PR. Phantosmias and Parkinson disease. Arch Neurol. 2008; 65:1237–1239.
4. Seok J, Shim YJ, Rhee CS, Kim JW. Correlation between olfactory severity ratings based on olfactory function test scores and self-reported severity rating of olfactory loss. Acta Otolaryngol. 2017; 137:750–754.
5. Leopold D. Distortion of olfactory perception: diagnosis and treatment. Chem Senses. 2002; 27:611–615.
6. Sjolund S, Larsson M, Olofsson JK, Seubert J, Laukka EJ. Phantom Smells: Prevalence and Correlates in a Population-Based Sample of Older Adults. Chem Senses. 2017; 42:309–318.
7. Henkin RI, Potolicchio SJ, Levy LM. Olfactory Hallucinations without Clinical Motor Activity: A Comparison of Unirhinal with Birhinal Phantosmia. Brain Sci. 2013; 3:1483–1553.
8. Royet JP, Plailly J. Lateralization of olfactory processes. Chem Senses. 2004; 29:731–745.
9. Menini A, Lagostena L, Boccaccio A. Olfaction: from odorant molecules to the olfactory cortex. News Physiol Sci. 2004; 19:101–104.
10. Omuro A, DeAngelis LM. Glioblastoma and other malignant gliomas: a clinical review. JAMA. 2013; 310:1842–1850.
11. Capampangan DJ, Hoerth MT, Drazkowski JF, Lipinski CA. Olfactory and gustatory hallucinations presenting as partial status epilepticus because of glioblastoma multiforme. Ann Emerg Med. 2010; 56:374–377.
12. Pinder RM, Brogden RN, Speight TM, Avery GS. Sodium valproate: a review of its pharmacological properties and therapeutic efficacy in epilepsy. Drugs. 1977; 13:81–123.
13. Kong X, Wang Y, Liu S, Lu Z, Wu H, Mao X, et al. Dysphasia and phantosmia as first presentation of multifocal cerebral anaplastic astrocytomas: case report and review of the literatures. Medicine (Baltimore). 2015; 94:e877.
14. Chamberlain MC. Treatment options for glioblastoma. Neurosurg Focus. 2006; 20:E19.
15. Rulseh AM, Keller J, Klener J, Sroubek J, Dbaly V, Syrucek M, et al. Long-term survival of patients suffering from glioblastoma multiforme treated with tumor-treating fields. World J Surg Oncol. 2012; 10:220.
 XML Download
XML Download