

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Background and Objectives
Septoplasty is a commonly performed operation in otolaryngological practice. In cases of septal mucosal tearing, septal perforation can easily occur. The aim of this study was to investigate patients who underwent an autologous cartilage securing suture technique to prevent nasal septal perforation.
Subjects and Methods
A total of 403 patients who underwent septoplasty alone or with endoscopic sinus surgery for the past three years were enrolled in this study. Septal mucosal tearing occurred in 27 patients. In group 1 (15 patients), autologous cartilage was inserted between the injured mucosa. In group 2 (12 patients), autologous cartilage was inserted between the injured mucosa with a securing suture technique. We investigated the septal perforation rate between the two groups.
Figures and Tables
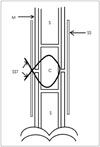
Fig. 1
After a Vicryl 5-0 suture is made intranasally through the upper edge of the site of the ipsilateral septal mucosal rupture, the suture is then passed through the mark on the graft on the outside of the nasal cavity and back through the lower edge of the septal mucosal rupture site intranasally.

Fig. 2
Placement of a cartilage interposition graft for repair of bilateral septal mucosal ruptures (A). Use of bayonet forceps for controlling the placement of the graft (B). Properly positioned cartilage interposition graft (C). The loose ends of the suture are then tied for securing the graft in place without tension (D).


References
1. Fairbands DN, Fairbanks GR. Nasal septal perforation: prevention and management. Ann Plast Surg. 1980; 5(6):452–459.

2. Yun DH, Kim YJ, Kim JH, Lee BJ. Causes and characteristic of the nasal septal perforation. J Rhinol. 2000; 7(1):64–68.
3. Kridel RW. Septal perforation repair. Otolaryngol Clin North Am. 1999; 32(4):695–724.
4. Choi YS. Diagnosis and treatment of nasal septal perforation. Korean J Otolaryngol-Head Neck Surg. 2006; 49(6):586–592.
5. Lee JY, Lee SW, Lee JD, Lee YM, Shin JM, Lee JY. Usefulness of autologous cartilage and fibrin glue for the prevention of septal perforation during septal surgery: a preliminary report. Korean J Otolaryngol-Head Neck Sur. Korean J Otolaryngol-Head Neck Surg. 2006; 49(6):611–615.
6. Choi JS, Jin KH, Park MW, Kang SH, Lim DJ, Yu MS, et al. Prevention technique using inferior turbinate mucosal flap for septal perforation after septoplasty. J Rhinol. 2014; 21(1):37–40.
7. Hong SK, Min YG. Repair of nasal septal perforation by intranasal approach using a free composite graft of the auricular cartilage and the temporalis muscle fascia. Korean J Otorhinolaryngol-Head Neck Surg. 2002; 45(10):969–974.
8. Kuriloff DB. Nasal septal perforation and nasal obstruction. Otolaryngol Clin North Am. 1989; 22(2):333–350.
9. Butz DR, Warner J. Transcutaneous securing technique for nasal onlay grafts. JAMA Facial Plast Surg. 2015; 17(2):149–150.
 XML Download
XML Download