

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Abuse experienced by older adults is a serious public health issue around the world. Major global institutions, such as the World Health Organization (WHO) and United Nations, have emphasized the severity of abuse in older adults in their reports.12 Abuse is a stressful life event that adversely affects the physical and mental health of older adults. It is also associated with premature morbidity, increase in hospitalization rate, and increased likelihood of death, according to existing research.345 Physical abuse is the most commonly recognized form of abuse in older adults, although sexual and emotional abuse, as well as financial exploitation and neglect, are prevalent. A recent meta-analysis estimated an overall incidence of elder abuse of 15.7% in community-dwelling in older adults, and that of psychological abuse was 11.6%, accounting for 73.8% of all instances of abuse in older adults.6
Increases in older adult populations are a global trend. South Korea, in particular, has experienced an unprecedented increase therein, and is faced with many dilemmas resulting therefrom. In this aging society, many elderly persons suffer from chronic diseases, loneliness, disability, and dementia; they need support from their families and society more than ever. Moreover, psychiatric problems and emotional distress, such as suicide, depression, etc. are common.7 Therefore, this study aimed to investigate the relationship between emotional abuse and depression in a large, representative sample of community-dwelling older adults in Korea.
Our study analyzed the dataset of the Survey of the 2011 Living Conditions and Welfare Needs of Korean Older Persons conducted by the Korea Institute for Health and Social Affairs.8 This survey is a government-approved statistical survey (Statistics Korea, approval No. 11771), which has been conducted every 3 years since 2008 with representative samples using a stratified two-stage cluster sampling design of non-institutionalized in older persons in Korea. This survey collected information via face-to-face interviews. All participants provided written informed consent. A total of 11542 persons aged over 60 years completed the survey (response rate=76.2%). We limited our analysis to 10674 persons over 65 years of age. This study was approved by the Research Ethics Committee of Chonbuk National University Hospital (CUH 2017-12-020).
We collected information on socio-demographic (age, gender, living alone, educational status, economic status), health-related (number of chronic illness, functional impairment), and psychological variables (social support, depression, emotional abuse). Emotional abuse was assessed via one question “Have you ever been emotionally hurt by other's word or action?” and possible responses were yes/no. The number of chronic illnesses was ascertained with the question “Do you currently have a chronic illness for more than 3 months that was diagnosed by a physician?” The type of chronic illness included hypertension, stroke, hyperlipidemia, ischemic heart disease, etc., and their numbers were categorized into no chronic illness, 1, 2, or more than 3. Functional impairment was defined as the need for help with personal care in at least one item in the Korean Instrumental Activities of Daily Living (K-IADL),9 which categorizes activities into 10 domains (personal grooming, doing housework, preparing meals, doing laundry, going out for a short distance, using transportation, shopping, managing money, using a telephone, and taking medicine).
Social support was assessed with the question “How many close friends and relatives do you have (people with whom you can talk about what is on your mind)?” and answers were categorized into none, 1–2, 3–5, or more than 6 persons. Depression was assessed using the Korean version of the Short Geriatric Depression Scale (SGDS),1011 a 15-item self-administered questionnaire with scores ranging from 0 to 15. Participants who scored higher than 8 were defined as having depression. This questionnaire has shown high sensitivity (0.8548) and specificity (0.6957) for depression in a previous study.11
Descriptive statistics (including frequencies and percentages) were used to describe demographic, health-related, and psychological variables. Univariate analyses were performed to identify associations between emotional abuse and each dependent variable using chi-square tests. A multivariate logistic regression analysis was used to calculate adjusted odds ratios (ORs) of emotional abuse after controlling for confounding variables.
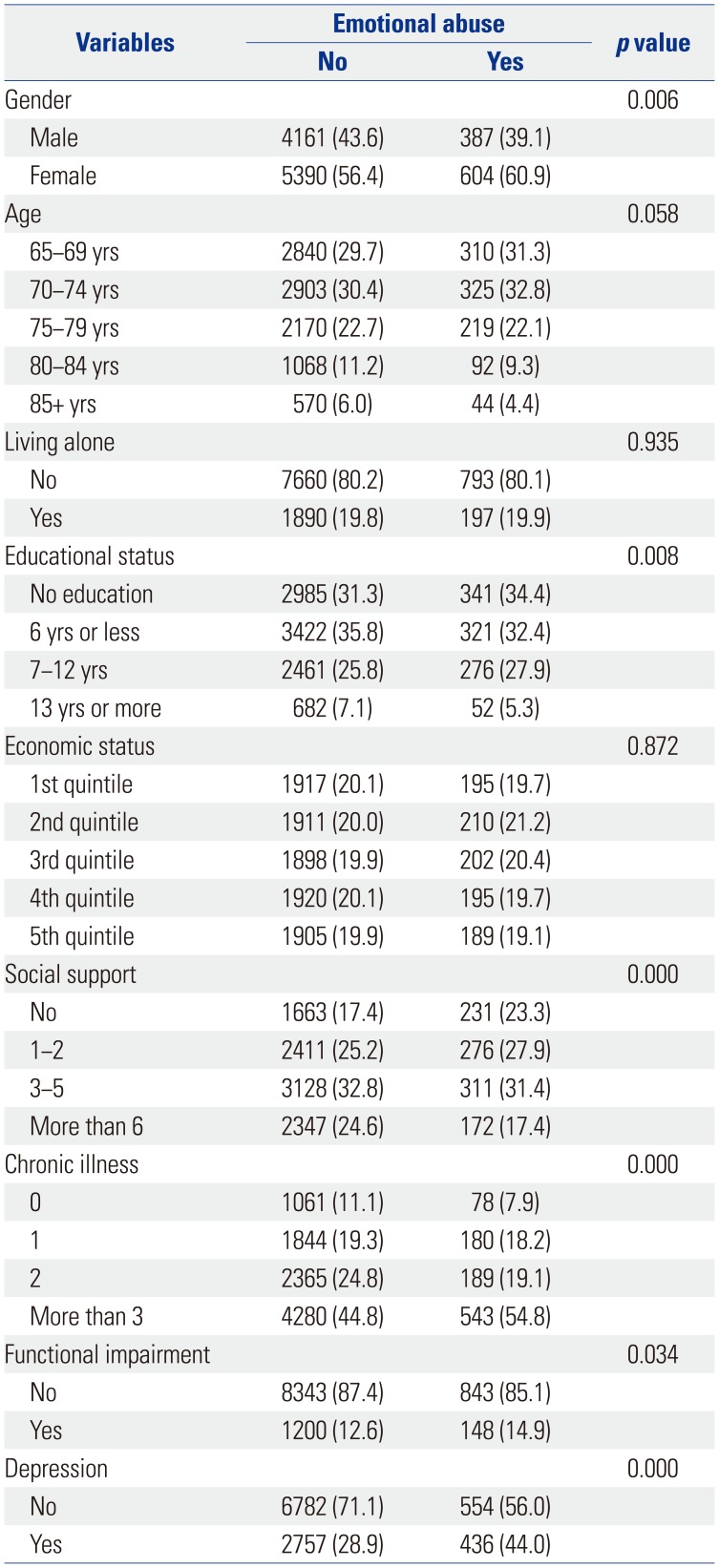
Of the 10541 older adult participants assessed in the present study, 9.4% had experienced emotional abuse in the last 12 months. The univariate analyses revealed independent variables that were associated with emotional abuse (Table 1). Participants who had experienced emotional abuse were more likely to be female, less educated, and functionally impaired and to have poor social support, chronic illnesses, and depression. The prevalence of depression was significantly higher in elderly persons with emotional abuse than in those without emotional abuse (44.0% vs. 28.9%, p<0.001).
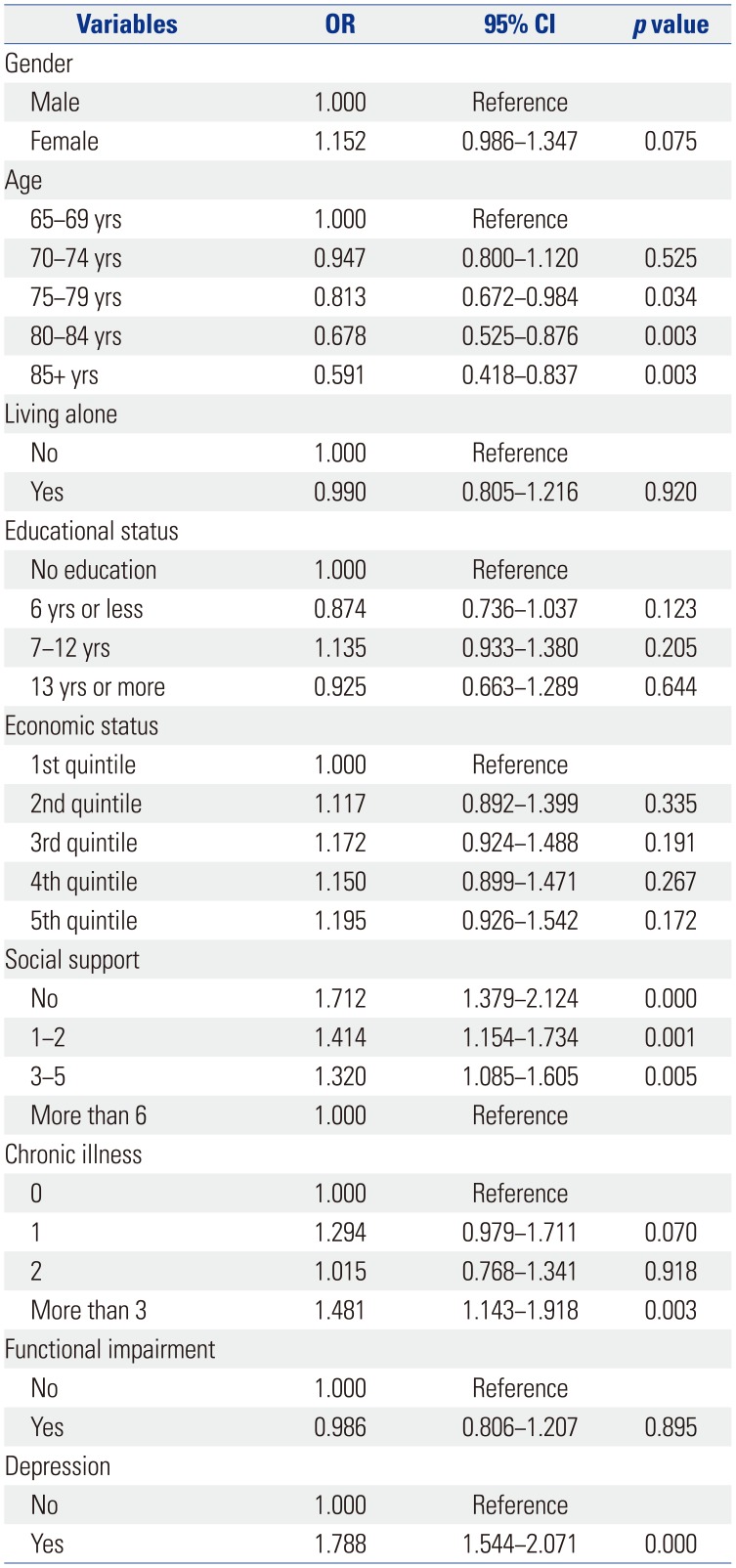
Multivariate regression analysis revealed that emotional abuse was independently associated with older age (ORs=0.813, 0.678, and 0.591 for participants aged 75–79, 80–84, and ≥85 years, respectively), poorer social support (ORs=1.320, 1.414, and 1.712 for 3–5 persons, 1–2 persons, and no social support, respectively), a higher number of chronic illnesses (ORs=1.294 and 1.481 for 1 and more than 3 chronic illnesses, respectively), and depression (OR=1.788) after controlling for confounding variables (Table 2).
This study sought to examine the relationship between depression and emotional abuse in a sample of older Korean adults. Studies on emotional abuse and depression among elderly persons in the community have been conducted mainly in Western countries. There have been few studies conducted in Asia, and no study has been conducted using a large sample. The fact that research related to older adults abuse in Korea is in its early stage makes this study especially important. The population of older adults in Korea has been rapidly increasing due to an increase in life expectancy and a decrease in the fertility rate. South Korea will be an aged society, with 14% of the total population over 65 years of age, and will account for 14.3% of the total population by 2018, which is a very rapid change, compared to other developed and less developed countries'. It is expected that South Korea will enter a post-aged society with 20% of its population over 65 years by 2026.12 Concerns surrounding emotional abuse of elderly persons increase when the support system for elderly persons becomes deficient, owing to sudden changes in the social structure, in the family structure from extended to nuclear families, and decreased supporting attitude toward the care of older persons.
In the present study, a substantial proportion of older persons (9.4%) reported experiencing emotional abuse in the past year. The rate of depression in older adults who experienced emotional abuse (44.0%) was higher than in those who did not (28.9%). The results of the regression analysis after controlling confounding variables showed that age, social support, chronic illness, and depression were factors associated with emotional abuse in older adults in Korea, among which depression had the greatest effect (OR=1.788).
The identification of depression as a factor associated with emotional abuse is consistent with the results of previous studies. Older patients who visited the Baylor College of Medicine Geriatric clinic in Texas, USA were found to have depression (based on DSM-IV criteria13); there was a statistically significant, higher prevalence rate of depression among those who experienced abuse (62% vs. 12%), compared to the comparison group who did not have such experience.14 The Chicago Health and Aging Project, a large-scale research with community-dwelling persons in the US (n=7841), reported that a higher level of depressive symptoms, measured using a modified version of the Center for Epidemiologic Studies of Depression Scale,15 was associated with an increased mortality rate among older persons who had experienced abuse.16 An ad hoc study of 4000 older adults aged 65 years or older who were receiving health and/or social community services in 11 European countries showed that the presence of depression (indicated by a cut-off score of 3 on the Minimum Data Set Depression Rating Scale17) predicted the occurrence of abuse in older adults.18
Relevant research on the subject conducted in Asia also identified significant associated factors. A study of 441 urban Chinese elderly persons reported that the risk of abuse in older adults was higher among those with depression (OR=4.47 for men, OR=8.54 for women), defined as more than 3 points for five questions of the Geriatric Depression Scale.19 A study showed that the dependency of Korean elderly persons (n=246) whose spouses had passed away was affected directly or indirectly by emotional abuse.20 In a study of abuse and its related factors among elderly stroke patients (n=934) living in the community, the risk of abuse was higher in participants with depression (SGDS score 8 or higher, OR=2.72).21 The fact that depression is an associated factor for emotional abuse among older adults has several important implications. Because depression in elderly persons is often found together with executive dysfunction, it is difficult for seniors to make appropriate judgments in major decision-making processes related to medical treatments, institutional care, and other kinds of care they might receive.1422 Depression could lead to suicidal ideation and attempts in severe cases. Based upon the possibility of recovery through various approaches, such as pharmacotherapy and psychosocial therapy, it is important to offer treatment opportunities and a systematic approach through which to treat elderly depression with emotional abuse. In addition, screening for depression in older adults suffering emotional abuse and developing preventive strategies for depression may reduce the distress caused by emotional abuse.
The results of this study verified that, along with depression, the number of chronic illnesses and lack of social support were also associated with a higher risk of emotional abuse among elderly persons. It was reported that physical illness and lack of social support were major factors associated with abuse in older adults,1923 which implies that chronic diseases and social support as associated factors are also associated with depression in elderly persons experiencing abuse. Social support is also a major factor influencing elderly depression and suicide, and depressive patients may not receive adequate medical treatment for physical illnesses due to depressive symptoms or not being treated on time. Therefore, it is important to examine social support systems for older adults who are experiencing emotional abuse, to address any shortcomings, and to approach the treatment of chronic diseases appropriately. Furthermore, it is necessary to discuss societal problems and solutions, to strengthen support services for the older adult population, and to establish preventive programs for abuse in older individuals.
This study has several limitations, and as a result, the findings should be interpreted cautiously. First, our study design was cross-sectional, and we did not investigate the onset of emotional abuse and depressive episode. Therefore, we could not infer a causal relationship. Further longitudinal study is required to explore the diverse relationship between emotional abuse and the main variables of interest. Second, questions about emotional abuse were non-validated and self-reported, which might lead to recall bias.
In conclusion, the results of this study indicate that emotional abuse among older persons in Korea is a serious issue. The major factors associated with emotional abuse were social support, chronic illness, and depression. In order to reduce the level of emotional distress among abused older persons, it is imperative to create a systematic method to approach these associated factors. Further research is essential to develop efficient and systematic prevention strategies and a management system for abuse in older adults.
 XML Download
XML Download