

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Upper extremity musculoskeletal disorders (UEMDs) are common in the general population. Point prevalence rates for UEMDs range from 2–53%, while 12-month prevalence rates range from 2–41%, depending on the setting, definition, and classification used.12 Upper extremity pain can cause substantial disability, need for health care, and loss of work time.3 Studies in the general population, as well as those involving workers, report that UEMDs have a negative impact on quality of life (QOL).45
The UEMDs include cervical disc disease, myelopathy, rotator cuff disease, lateral and medial epicondylitis, carpal tunnel syndrome, ulnar nerve entrapment syndrome, osteoarthritis (OA), myofascial pain syndrome, and other conditions.6 In a recently published systematic review, the most frequently identified work-related UEMD was rotator cuff disease.7 A rotator cuff tear not only causes pain, but can lead to declines in muscle strength and shoulder mobility. These symptoms can have a negative impact on activities of daily living, work, and leisure activities.8 Other common UEMDs include lateral and medial epicondylitis and hand OA, which have also been reported to have a negative impact on upper extremity function and activities of daily living.910
However, diagnostic criteria for UEMDs have varied among studies, and inconsistent results have been reported.111 Furthermore, most previous studies have been based on questionnaires, with or without physical examination. There is little research on how the occurrence of simultaneous UEMDs affects upper extremity-related QOL. In addition, there is no literature about the prevalence of UEMD on the dominant side and its effect on upper extremity-related QOL in the general population.
The purpose of this study was to evaluate the prevalence of rotator cuff tear, epicondylitis, and hand OA on the dominant side and to evaluate the impact of these UEMDs on QOL using the disability of arm, shoulder, and hand (DASH) outcome measure for assessing upper extremity-related QOL.
MATERIALS AND METHODS
Selection of subjects
This study was conducted as part of the farmers' UEMD investigation (Namgaram study). Participants in this study were enrolled from members of rural communities in Gyeongsangnam- do, Korea, who were over 40 years of age. After selecting six villages in the rural area, the survey was conducted among villagers who agreed to participate. The study was conducted from July 2013 to November 2015. Researchers visited the six villages and informed the population about the purpose of the study and related processes, and those who agreed to participate were enrolled. Inclusion criteria for the study were 1) literacy level sufficient to complete the questionnaire, 2) unaffected activities of daily living, 3) being socially active, and 4) not receiving medical services for UEMDs within the previous 12 months. Each participant completed a questionnaire and underwent physical examination, laboratory tests, simple radiographic evaluations of bilateral upper extremities, and bilateral shoulder magnetic resonance imaging (MRI) studies. Three research nurses knowledgeable in the purpose of the study and related data collection procedures interviewed each participant using a questionnaire. The total number of participants completing all aspects of the study was 987, including 295 non-agricultural workers (29.88%) and 692 agricultural workers (70.11%). The study was approved by the Institutional Review Board of Gyeongsang National University (IRB No. GNUH 2015-02-001).
Demographic and health-related characteristics
Demographic information collected from study participants included gender, age, marital status (dichotomized as “yes” and “no”), and educational level (categorized as “less than elementary school,” “middle school,” and “more than high school”). The dominant side was categorized as “right,” “left,” or “both.” If the participant was ambidextrous, one side was randomly selected for study regardless of the presence of a UEMD.
Hypertension, diabetes mellitus, waist circumference, depression, and laboratory test findings were also considered in the study. The presence of comorbidities was evaluated through history taking, blood pressure (BP) measurement, and laboratory tests. Hypertension was diagnosed based on medical history and detection of BP above 140 mm Hg systolic or above 90 mm Hg diastolic pressure. BP was measured twice in a seated position after ≥5 minutes of rest using an automatic electronic sphygmomanometer (HBP-1300, Omron Healthcare®, Kyoto, Japan).12 A prior diagnosis of diabetes was accepted for study purposes. New cases of diabetes were also diagnosed upon confirming serum level of HbA1c higher than 6.5%.13 Waist circumference was measured parallel to the midline between the lowest border of the rib cage and the iliac crest at the end of a normal expiration, with participants standing with their feet 25–30 cm apart.14 Waist circumference was measured using a measuring tape. Depressive symptoms were measured with the Patient Health Questionnare-2 (PHQ-2), a two-item questionnaire that uses a four-point scale (0=not at all to 3=nearly every day).15 A higher score indicates greater depression. Laboratory tests performed for study purposes included hemoglobin and total cholesterol.
Clinical evaluation
We evaluated DASH and performed a functional assessment of each region of the dominant side and related UEMDs based on data from study participants. Prior to evaluation of UEMDs, functional assessment of each region was performed. Shoulder joints were assessed with the Constant-Murley score (CMS), elbow joints were assessed with the Mayo elbow performance score (MEPS), and hands were assessed with the Australian/Canadian Hand Osteoarthritis Index (AUSCAN).161718 Upper extremity- related QOL was assessed based on DASH,19 a 30-item questionnaire composed of 21 physical function items, six symptom items, and three social/role function items. Each item is rated on a five-point Likert scale (1=least disability to 5= most disability). All 30 response scores were added together, producing a raw score, which was then transformed into a maximum score of 100. A higher score indicates greater disability. Cronbach's α was 0.95 in this study. CMS, MEPS, and AUSCAN scores were assessed by two experienced orthopedic surgeons, each with more than 10 years of experience.
Diagnostic criteria
For the purposes of the current study, rotator cuff tears included partial and full thickness tears and were diagnosed by MRI. A 3.0 Tesla MRI system (Ingenia; Philips Medical Systems®, Eindhoven, the Netherlands) was used to obtain MRI images, which included axial, sagittal, and coronal T2-weighted images [repetition time (TR)/echo time (TE)=2800/60]; coronal T1-weighted images (TR/TE=500/20); and coronal fat-saturated fast spin-echo images. Slice thickness was 3 mm without gaps. In MRI findings, a partial-thickness tear of the rotator cuff was diagnosed when a focus of high signal intensity was apparent on T2-weighted images in either the bursa or the joint surface of the tendon that did not involve the entire thickness of the cuff. A full thickness tear of the rotator cuff was diagnosed when focal or diffuse high signal intensity on T2-weighted images extended from the bursa to the joint surface of the tendon or when the tendinous portion of the cuff was not visualized.20 MRI scans were interpreted by a radiologic specialist with 20 years of experience and an orthopedic surgeon with 15 years of experience. Among total participants, 438 (44.4%) had partial thickness tears and 89 (9.0%) had full thickness tears.
Epicondylitis included lateral and medial epicondylitis. Epicondylitis was defined as self-reported pain at either epicondyle area on two or more days in the previous month and one of the following during the exam: presence of pain at the lateral epicondyle with resisted active wrist extension, pain at the medial epicondyle with resisted active wrist flexion, or tenderness to palpation over the medial and lateral epicondyle regions during physical exam.21 Physical examination was performed by an orthopedic surgeon and a rheumatologist with more than 10 years of experience each. Epicondylitis was present in 333 (33.7%) of the total participants.
For diagnosis of hand OA, anterior-posterior plain radiographs of both hands were obtained from all participants. The second to fifth distal interphalangeal, proximal interphalangeal, first to fifth metacarpophalangeal, thumb interphalangeal, and first carpometacarpal joints for each hand were graded for OA using the modified Kellgren-Lawrence (KL) scale. This scale assesses the existence and severity of osteophytes (OPs), joint space narrowing (JSN), sclerosis, and erosion. The modified KL scale was graded from 0 to 4, where 0=no OA; 1=questionable OPs and/or JSN; 2=definite small OPs and/or mild JSN; 3=moderate OPs and/or moderate JSN, sclerosis, and possible presence of erosion; and 4=large OPs and/or severe JSN, sclerosis, and possible presence of erosions.22 Radiological hand OA was defined as a case wherein the result of plain radiography was determined to be higher than KL grade 2 for at least one joint.23 These radiographs were interpreted by a musculoskeletal radiologic specialist with 20 years of experience in radiographic evaluation and a rheumatologist with 10 years of experience in radiographic evaluation. Hand OA was present in 440 (44.6%) of all participants.
Statistical analysis
We assessed differences in each UEMD in terms of demographics and existing comorbidities using the independent-samples t-test for continuous variables. For categorical variables, we used the chi-square test for analysis. Continuous variables are described as mean and standard deviation and categorical variables as percentage.
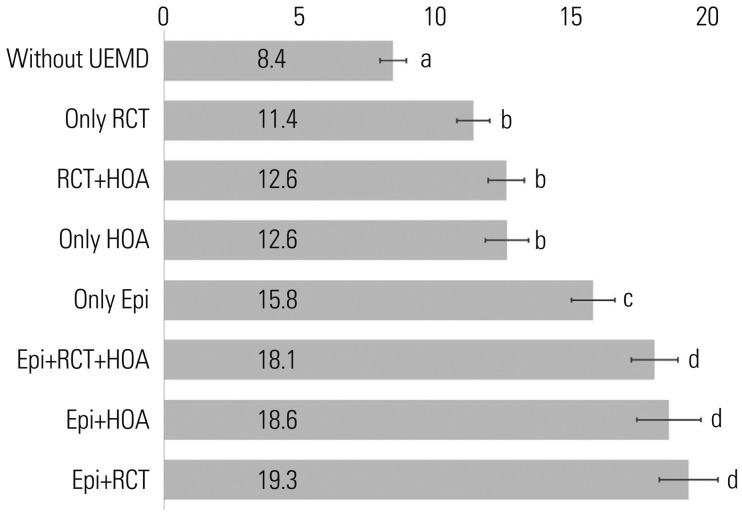
Differences in DASH score according to UEMDs were evaluated in two ways. First, differences in DASH score according to the presence or absence of epicondylitis, rotator cuff tear, and hand OA was examined. Second, participants were classified as follows: 1) participants without UEMD, 2) participants with only epicondylitis, 3) participants with only rotator cuff tear, 4) participants with only hand OA, 5) participants with epicondylitis and rotator cuff tear (epicondylitis+rotator cuff tear), 6) participants with epicondylitis and hand OA, 7) participants with rotator cuff tear and hand OA, and 8) participants with all three UEMDs (epicondylitis+rotator cuff tear+ hand OA). The significance of differences in DASH scores among these groups was evaluated using t-test or ANOVA, and only significant factors were adjusted. The Tukey method was utilized for post-hoc testing.
Multiple regression analysis was performed to determine the association between UEMDs and regional functional assessment scores. Each group with at least one disease based on the absence of UEMD was dummy variable. Regression analysis was used to identify how each variable was associated with DASH score. All regression analyses were adjusted for demographics and comorbidities that differed in each disease as primitive variables. Univariate analysis was performed to determine the association between DASH and UEMD or regional functional assessment score. Multiple regression analysis was performed to determine the association between DASH and UEMD and each regional functional assessment score. Multiple regression analysis was also used to determine the association between DASH and UEMD and all regional functional assessment scores. All regression analyses were assessed for multicollinearity.
IBM® SPSS Statistics software, version 23.0 (IBM Corp., Armonk, NY, USA) was used to analyze the data, and p<0.05 was considered to indicate statistical significance.
RESULTS
Population demographics and comorbidities
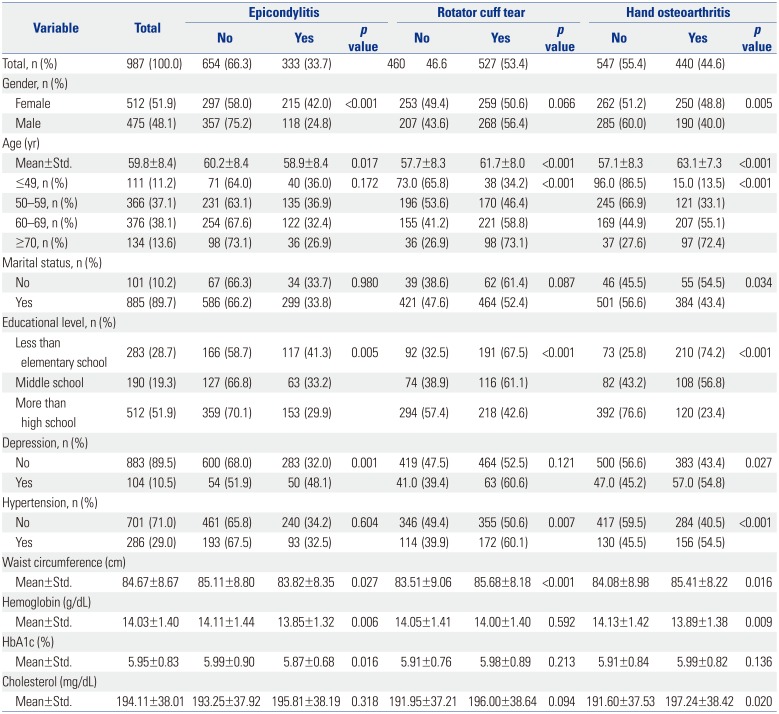
Findings related to study population demographics and comorbidities and differences according to disease are shown in Table 1. Of all participants, 475 (48.1%) were male and 512 (51.9%) were female. The mean age of participants was 59.8±8.4 years.
The prevalences of epicondylitis, rotator cuff tear, and hand OA among all subjects were 33.7%, 53.4%, and 44.6%, respectively. Epicondylitis was significantly associated with gender, mean age, education level, depression, waist circumference, hemoglobin, and HbA1C, while rotator cuff tear was significantly associated with age, education level, hypertension, and waist circumference. Hand OA was significantly associated with gender, age, marital status, education level, depression, hypertension, waist circumference, hemoglobin, and total cholesterol.
UEMD and DASH scores
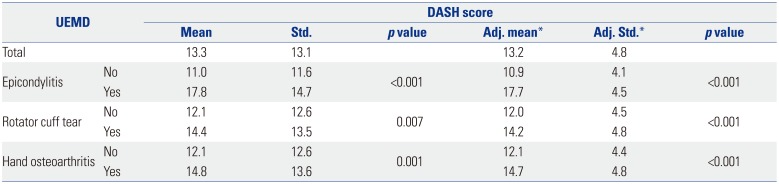
The DASH scores according to UEMD are shown in Table 2. There were significant DASH score differences according to the presence or absence of epicondylitis, rotator cuff tear, and hand OA. The same results were obtained when adjusting for primitive variables, including age, gender, educational level, marital status, depression, hypertension, waist circumference, hemoglobin, HbA1c, and total cholesterol. Each of these factors was associated with significant differences in outcome according to UEMD. DASH scores also differed between participants classified with only one UEMD and those with multiple UEMDs. DASH scores also differed in the four subgroups when adjusted for primitive variables in post-hoc tests (Fig. 1).
Regression analysis
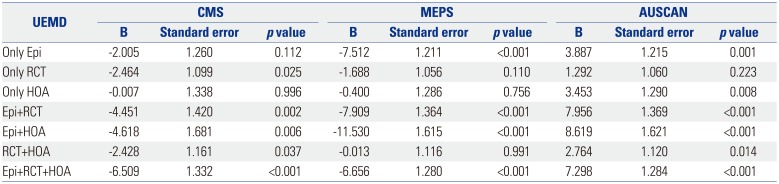
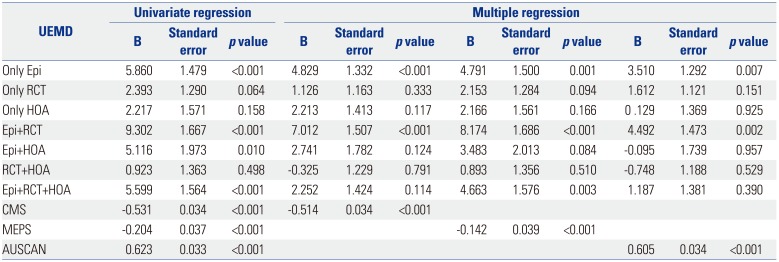
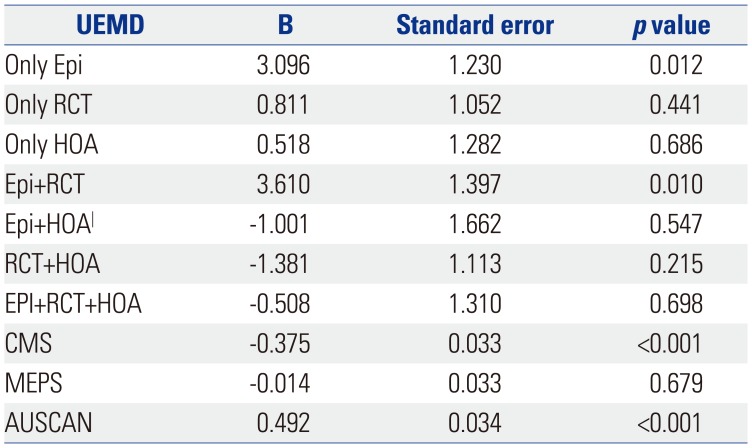
Multiple regression analysis results for the associations between UEMDs and regional functional assessment scores are presented in Table 3. Only rotator cuff tear, epicondylitis+rotator cuff tear, epicondylitis+hand OA, and epicondylitis+rotator cuff tear+hand OA were significantly associated with CMS. Epicondylitis, epicondylitis+rotator cuff tear, epicondylitis+hand OA, and epicondylitis+rotator cuff tear+hand OA were significantly associated with MEPS. Except for rotator cuff tear, all disease categories were associated with AUSCAN. Univariate regression analysis results of the associations between DASH score and UEMD are shown in Table 4. Only epicondylitis, epicondylitis+rotator cuff tear, epicondylitis+ hand OA, and epicondylitis+rotator cuff tear+hand OA were significantly associated with DASH score. All regional functional assessments were significantly associated with DASH score, even when adjusted for primitive variables and each UEMD. Multiple regression analysis results evaluating associations between DASH scores, UEMD, and regional functional assessment scores are shown in Table 5. Only epicondylitis, epicondylitis+rotator cuff tear, CMS, and AUSCAN scores were associated with DASH score.
DISCUSSION
In this study, DASH scores were higher in the presence of any UEMD than in the absence of any UEMD. The reported minimal clinically important difference for the DASH outcome measure is 10–10.81.2425 On the basis of this, differences in DASH scores according to the presence or absence of any UEMD were not clinically significant for UEMDs as evaluated in this study. However, DASH scores for epicondylitis+hand OA, epicondylitis+rotator cuff tear, and epicondylitis+rotator cuff tear+hand OA were 9.7–10.9 higher than in normal participants. Furthermore, according to multivariate regression analysis incorporating UEMD and regional functional assessment scores, CMS was more strongly associated with epicondylitis+rotator cuff tear than with only rotator cuff tear, and was most strongly associated with epicondylitis+rotator cuff tear+hand OA. Even in the absence of rotator cuff tear, CMS was associated with epicondylitis+hand OA. MEPS was associated with epicondylitis+rotator cuff tear, epicondylitis+hand OA, and epicondylitis+rotator cuff tear+hand OA, as well as with epicondylitis only. AUSCAN was associated with all UEMDs, with the exception of rotator cuff tear. Constant, et al.26 stated that strength could be underestimated during evaluation of CMS in the presence of elbow disease. Our findings suggest that regional functional assessments can be affected by disease in an adjacent area. This seems clinically significant and suggests that, when clinically significant loss of upper limb function occurs, UEMDs, including epicondylitis, are likely to be present.
All regional functional scores were associated with the DASH outcome measure, even when the analysis was adjusted for UEMDs. Multiple regression analysis showed that epicondylitis and epicondylitis+rotator cuff tear were associated with DASH score. CMS and AUSCAN were also associated with DASH score. The difference in the effects of epicondylitis seen in this study versus in previous studies could be due to differences in diagnostic methods. We diagnosed epicondylitis by physical examination, although rotator cuff tear and hand OA were diagnosed radiologically. Epicondylitis was present in a large number of patients with existing symptoms; however, rotator cuff tear and hand OA were often present in asymptomatic patients. Previous studies reported that rotator cuff tear and hand OA mostly presented with no symptoms.272829 Rotator cuff tear and hand OA are degenerative diseases, and age is the most important risk factor.293031 In conclusion, rotator cuff tear and hand OA are conditions induced by degenerative changes associated with the aging process. Therefore, the progression of rotator cuff tear and hand OA occurs gradually, leading to compensation for other normal tissues, and the disease itself is less likely to immediately affect QOL.3233 For this reason, rotator cuff tear and hand OA do not directly affect DASH. However, the presence of symptoms due to rotator cuff tear or hand OA had a negative impact on CMS and AUSCAN scores, which could affect DASH. In contrast, the primary cause of epicondylitis has been reported to be overuse; thus, the condition is common in the 40- to 50-year-old group.34 Therefore, if epicondylitis is not significantly affected by other factors and is due to overuse, symptoms are likely to be immediately evident and directly affect QOL. In this study, epicondylitis with symptoms was more likely to be selected. Therefore, epicondylitis directly affects DASH and MEPS.
We found that the prevalence of epicondylitis in the dominant arm was 33.7%, which is outside the range of 3.5–20.2% reported in the literature.3536 Our study included 692 agricultural workers, representing 70.11% of total participants. In other studies, the prevalence of epicondylitis was higher in agricultural workers than in factory workers.3536 This suggests that the agricultural work environment induces epicondylitis to a greater extent than a factory work environment. In the current study, the prevalence of rotator cuff tear in the dominant arm was 53.4% (partial thickness rotator cuff tear: 44.4%, full thickness rotator cuff tear: 9.0%), also higher than the 4.7–22.1% reported in the literature.3738 Unlike other studies that evaluated full thickness rotator cuff tears of the bilateral shoulders using ultrasound, we used MRI to evaluate the dominant shoulder only, which could account for the difference in prevalence. Nevertheless, the presence of a partial rotator cuff tear in 44.4% of participants is a surprising result. In this study, prevalence of hand OA in the dominant arm was 44.6%, which is lower than the 47–61.7% reported in the literature.3839 This may be because the mean age of participants in our study is lower than that of participants evaluated in other studies.
This study had several limitations. First, our sample size was fairly small, and because of the cross-sectional nature of the study, we could not assess the long-term effects of UEMD on QOL. Second, we did not evaluate all UEMDs and did not consider the radiologic severity of the disease. Therefore, we could not evaluate the effects of all UEMDs on QOL or if the radiologic severity of disease had an impact on QOL. Nevertheless, the severity of symptoms was reflected in the functional assessment scores, and we also evaluated QOL according to symptoms. Third, the proportion of participants with mild functional impairment was relatively high in our study because participants were residents of rural communities who had not undergone hospital treatment due to UEMDs. Therefore, depending on the UEMD, moderate to severe symptoms might have different effects on upper extremity-related QOL.
The strength of this study is that UEMD evaluation was performed objectively in all participants by questionnaire survey, functional assessment, physical exam, and imaging tests. In particular, evaluation of rotator cuff tear using MRI is more accurate than evaluation using ultrasound, and partial thickness rotator cuff tear was included in the study. Moreover, our study is the first to examine the associations among UEMD, regional functional assessment scores, and upper extremity-related QOL.
In this study, UEMDs other than epicondylitis were predominantly asymptomatic, and epicondylitis was found to significantly affect upper extremity-related QOL, while other UEMDs, such as hand OA and rotator cuff tear, did not. In conclusion, the presence of UEMDs does not often affect upper extremity-related QOL, and it is difficult to detect the presence of disease and receive treatment in advance, even if the patient is affected by the disease. This suggests that it is important to diagnose UEMDs at an early stage to prevent irreversible degenerative changes. When a UEMD impacts upper extremity-related QOL in patients, it is highly likely that another UEMD is also present. Therefore, physicians should meticulously evaluate and diagnose such patients.
 XML Download
XML Download