

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary artery bypass graft (CABG) surgery was first attempted in humans in 1960 using the internal mammary artery (IMA).1) Subsequently, percutaneous coronary intervention (PCI) using transluminal balloon angioplasty was introduced as alternative method for coronary artery revascularization in 1977.2) Over the years, percutaneous and surgical revascularization techniques complemented advances in medical therapies to provide contemporary treatment of acute coronary syndrome (ACS) and management of stable coronary artery disease (SCAD) to improve angina, heart failure symptoms, and quality of life (QoL).3)4)5)6) In patients with left main disease (LMD) and multivessel disease (MVD), revascularization has been shown to prolong survival.6)7)8) Historically, CABG was considered the treatment of choice of MVD and LMD. However, remarkable advances in PCI led to higher procedural success rates, decreased procedural myocardial infarction (MI), target lesion revascularization (TLR), in-stent thrombosis, and in-stent restenosis rates. As such PCI became a viable alternative to CABG in treatment of LMD and MVD. Multiple moderate size randomized controlled trials comparing both treatment strategies in LMD and MVD intervention revealed an increase in periprocedural cardiac and cerebrovascular events with CABG but higher long-term need for repeat revascularization in patients managed with PCI.9)10)11)12) The Synergy between PCI with TAXUS and Cardiac Surgery (SYNTAX) trial further advanced our knowledge by dividing outcomes of both strategies based on anatomical complexity of coronary artery disease (CAD) revealing comparable outcomes with first generation drug-eluting stent (DES) and contemporary CABG practice in patients with simpler coronary lesions.13)14) Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease (EXCEL)15) and Nordic-Baltic-British left main revascularization (NOBLE)16) trials were most recent multicenter randomized open-label non-inferiority trials comparing the newest second generation stents versus CABG in intermediate to low risk left main revascularization. The trials showed conflicting results: non-inferiority of PCI for treatment and safety endpoints of death from any cause, stroke, or MI at follow-up was achieved in EXCEL but not in NOBLE as the trial showed higher revascularization rates, MI, and surprisingly more frequent stroke in patients treated with PCI.
This review is focused on revascularization of LMD and MVD in patients who are not presenting with ST-segment elevation myocardial infarction, encompassing the evidence from historic and contemporary trials which shaped up current practices. This review also discusses algorithmic heart team approach to guide decision making, as well as the conundrum of the special populations that are not represented in clinical trials.
Go to : 
LEFT MAIN CAD
LMD with ≥50% stenosis is prevalent in 4–7% of patients who undergo coronary angiography.17) Non-revascularized LMD has been associated with significant comorbidity and 5-year mortality approaching 60%.18) More than 50% of left main (LM) lesions involve the left anterior descending-circumflex coronary artery bifurcation and almost 80% coexist with multivessel CAD.19)20) Historically, the standard of care for these patients was CABG since it has been associated with improved long-term survival and reduced MI when compared to medical therapy alone.7) Subsequent studies showed similar intermediate and long-term mortality and MI between PCI of and CABG of unprotected LMD with a trend toward higher need for revascularization in patients treated with stenting and higher rates of strokes with surgical intervention, Table 1. This led to the SYNTAX multicenter randomized controlled trial which compared first-generation TAXUS Express paclitaxel eluting stent (PES) versus CABG for LMD and MVD. The trial enrolled a total of 705 patients in the LMD subgroup.21)22) Around 95% of patients completed follow-up to 5 years. The rates of major adverse cardiac and cerebrovascular events (MACCE) defined as death, MI, stroke, and repeat revascularization were not significantly different between both treatment modalities (36.9% with PCI and 31% with CABG). However, patients who underwent CABG had higher rates of stroke (4.3% in CABG vs. 1.5% in PCI arm; p=0.03), while more patients managed with PCI needed repeat revascularization (26.7% in PCI arm vs. 15.5% in CABG arm; p<0.01). Stratifying by complexity of the coronary anatomy, this trial showed that the more complex the coronary disease distribution, the lower the MACCE rate with CABG as compared with PCI in LMD, leading to the development of the SYNTAX score. This score uses a point system depending on location of coronary artery atherosclerotic plaque, with a cut-off score of 33 to reflect complex coronary disease that would extract much benefit from CABG over PCI. This benefit was mainly driven by significant decrease in repeat revascularization rates in the surgical arm.
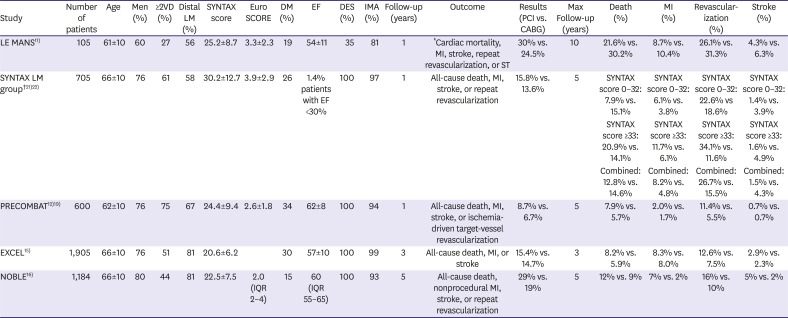
Table 1
Summary of most important randomized controlled trials in left main disease revascularization
| Study | Number of patients | Age | Men (%) | ≥2VD (%) | Distal LM (%) | SYNTAX score | EuroSCORE | DM (%) | EF | DES (%) | IMA (%) | Follow-up (years) | Outcome | Results (PCI vs. CABG) | Max Follow-up (years) | Death (%) | MI (%) | Revascularization (%) | Stroke (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LE MANS11) | 105 | 61±10 | 60 | 27 | 56 | 25.2±8.7 | 3.3±2.3 | 19 | 54±11 | 35 | 81 | 1 | *Cardiac mortality, MI, stroke, repeat revascularization, or ST | 30% vs. 24.5% | 10 | 21.6% vs. 30.2% | 8.7% vs. 10.4% | 26.1% vs. 31.3% | 4.3% vs. 6.3% |
| SYNTAX LM group†21)22) | 705 | 66±10 | 76 | 61 | 58 | 30.2±12.7 | 3.9±2.9 | 26 | 1.4% patients with EF <30% | 100 | 97 | 1 | All-cause death, MI, stroke, or repeat revascularization | 15.8% vs. 13.6% | 5 | SYNTAX score 0–32: 7.9% vs. 15.1% | SYNTAX score 0–32: 6.1% vs. 3.8% | SYNTAX score 0–32: 22.6% vs 18.6% | SYNTAX score 0–32: 1.4% vs. 3.9% |
| SYNTAX score ≥33: 20.9% vs. 14.1% | SYNTAX score ≥33: 11.7% vs. 6.1% | SYNTAX score ≥33: 34.1% vs. 11.6% | SYNTAX score ≥33: 1.6% vs. 4.9% | ||||||||||||||||
| Combined: 12.8% vs. 14.6% | Combined: 8.2% vs. 4.8% | Combined: 26.7% vs. 15.5% | Combined: 1.5% vs. 4.3% | ||||||||||||||||
| PRECOMBAT12)19) | 600 | 62±10 | 76 | 75 | 67 | 24.4±9.4 | 2.6±1.8 | 34 | 62±8 | 100 | 94 | 1 | All-cause death, MI, stroke, or ischemia-driven target-vessel revascularization | 8.7% vs. 6.7% | 5 | 7.9% vs. 5.7% | 2.0% vs. 1.7% | 11.4% vs. 5.5% | 0.7% vs. 0.7% |
| EXCEL15) | 1,905 | 66±10 | 76 | 51 | 81 | 20.6±6.2 | 30 | 57±10 | 100 | 99 | 3 | All-cause death, MI, or stroke | 15.4% vs. 14.7% | 3 | 8.2% vs. 5.9% | 8.3% vs. 8.0% | 12.6% vs. 7.5% | 2.9% vs. 2.3% | |
| NOBLE16) | 1,184 | 66±10 | 80 | 44 | 81 | 22.5±7.5 | 2.0 (IQR 2–4) | 15 | 60 (IQR 55–65) | 100 | 93 | 5 | All-cause death, nonprocedural MI, stroke, or repeat revascularization | 29% vs. 19% | 5 | 12% vs. 9% | 7% vs. 2% | 16% vs. 10% | 5% vs. 2% |
Continuous variables presented as mean value and standard deviation except for EuroSCORE and ejection fraction in NOBLE trial which reported in median and interquartile range. Crush technique for bifurcation lesions was performed only in 6% of cases in SYNTAX trial and 4% of cases in NOBLE trial.
CABG = coronary artery bypass graft; DES = drug-eluting stent; DM = diabetes mellitus; EF = ejection fraction; EXCEL = Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease; IMA = internal mammary artery; MACCE = major adverse cardiac and cerebrovascular events; MI = myocardial infarction; NOBLE = Nordic-Baltic-British left main revascularization; ST = stent thrombosis; STS = Society Thoracic of Surgeons; SYNTAX = Synergy between PCI with TAXUS and Cardiac Surgery; PCI = percutaneous coronary intervention; PRECOMBAT = Premier of Randomized Comparison of Bypass Surgery Versus Angioplasty Using Sirolimus-Eluting Stent (SES) in Patients With Left Main Coronary Artery Disease2VD = Two vessel disease.
*MACCE was a secondary endpoint in LE MANS trial; †Predefined and powered subgroup analysis in randomized clinical trial.
![]()
Similar intermediate and long-term results were observed in the Premier of Randomized Comparison of Bypass Surgery Versus Angioplasty Using Sirolimus-Eluting Stent (SES) in Patients With Left Main Coronary Artery Disease (PRECOMBAT) study which compared the other first generation Sirolimus DES to CABG for the treatment of unprotected LMD12)19) This study demonstrated a 2-fold increase in the rates of ischemia driven target vessel revascularization (TVR) in the PCI arm, albeit without differences in composite MI, stroke or death rates. Nevertheless, in a subgroup analysis, MACCE was 2-fold higher in patients with condominant LMD and 3 vessel disease.
The introduction of second generation zotarolimus and everolimus eluting stents (ZES and EES) with chromium alloy and thinner struts led to the reduction of MI, stent thrombosis, and TVR when compared to first generation DESs.23)24) More so, the integration of intravascular imaging during PCI was shown to reduce TLR and MI by assisting proper stent sizing, coverage of the length of the lesions, and adequate stent apposition.25) In parallel to advances in equipment, studies have shown that techniques for stent placement in the LM, particularly the LM bifurcation stent, can impact outcomes. Recent trials showed that the double kissing (DK) crush technique for LM bifurcation stenting had a lower rate of TLR and stent thrombosis compared to Culotte double stenting and a single stent provisional stenting, commonly used in non-LM bifurcation stenting.26)27)28)
EXCEL and NOBLE trials are the 2 most recent randomized multicenter trials that compared second generation stents versus CABG for the treatment of unprotected LMD. The second generation EES (XIENCE; Abbott Vascular, Abbott Park, IL, USA) and Biolimus-eluting stents (BESs) (Biomatrix Flex; Biosensors International, Bulach, Switzerland) were used in EXCEL and NOBLE trials, respectively. EXCEL included patients with ≥70% LM stenosis or ≥50% disease that is hemodynamically significant by invasive or non-invasive assessment.15) Low to intermediate site-determined SYNTAX score was prerequisite for inclusion. Patients with ≥50% LM stenosis or fractional flow reserve ≤0.80 with no more than 3 additional non-complex lesions were enrolled in NOBLE trial.16) Use of contemporary stenting techniques and intravascular ultrasound (IVUS) guided treatment in the stent arm and arterial grafts in the CABG group were strongly encouraged in both trials. The primary endpoint was the cumulative events of all-cause death, stroke, or MI at 3 years in EXCEL study, while repeat revascularization was also included in composite primary outcomes at 5 years in NOBLE trial.
The simultaneously published trials showed conflicting results. In the EXCEL trial, PCI was non-inferior for primary endpoint to CABG at 3 years with comparable rates of composite end points of death, stroke, or MI (15.4% in the PCI arm versus 14.7% in the CABG arm; p<0.02 for non-inferiority). The rates of early death, MI, or stroke at 30 days were higher in the CABG (7.9%) versus PCI treatment (4.9%). Moreover, major periprocedural events at 30 days, such as, early MI, major bleeding, infection, and major arrhythmias, were 15% more frequent after CABG (23.0%) when compared to PCI (8.1%) (p<0.001 for superiority). At 3 years, the rates of ischemia driven repeat revascularization were 5% higher in the PCI arm (12.6% vs. 7.5% in CABG arm; p<0.001), but lower rates of stent thrombosis were seen when compared to acute graft occlusion. Overall, the results of EXCEL were more or so consistent with the previously published SYNTAX trial. Eighty percent of cases were distal LM bifurcation disease and around half of patients had 2 or 3 vessels disease in EXCEL trial. IVUS was utilized in 77.2% of cases and the majority (98.8%) had IMA in the CABG arm. The study had some limitations such as the inclusion of 24% of patients with high SYNTAX score after further angiographic review in core laboratory. Moreover, the length of follow-up is shorter than NOBLE trial, although 5-year assessment of outcomes is undergoing.
On the other hand, the results of the NOBLE trial favored CABG over PCI at 5 years follow-up (primary endpoint of 29% in PCI vs. 19% in CABG; p=0.007). The events in the PCI arm were driven by a statistically significant higher nonprocedural MI, repeat revascularization, and surprisingly a higher trend for stroke, which is contrary to the results of prior LMD and MVD trials. All of the stroke events occurred 30 days after PCI. Non-procedural MI was 5% higher (hazard ratio [HR], 2.88; 95% confidence interval [CI], 1.40–5.90) and repeat revascularization was 6% more frequent (HR, 1.50; 95% CI, 1.04–2.17) in PCI compared to CABG group. The rates of repeat revascularizations in PCI were driven by de novo lesions rather than repeat left main intervention. There was no difference in mortality over 5-year duration. There were few differences between both trials. First, periprocedural MI within 30 days were excluded in NOBLE which could explain the significantly higher MI observed with PCI in the study. Moreover, the first 73 patients enrolled (10% of PCI arm) received first generation stents before BES was recommended as a primary stent. IVUS (75%) and mammary grafts (92%) were not frequently utilized in NOBLE study. One caveat was the low utilization of DK-crush technique (≤6%) in both trials.
A recent meta-analysis by Giacoppo et al.,29) focusing on DES versus CABG for the treatment of unprotected LM disease with clinical follow-up of 3 or more years showed comparable safety results with the 2 revascularization strategies in lesions with low to intermediate complexity. The study included a total of 4,394 patients from SYNTAX, PRECOMBAT, NOBLE, and EXCEL trials. PCI and CABG were associated with comparable all cause death, MI, or stroke (HR, 1.06; 95% CI, 0.90–1.24; p=0.48). These results were consistent with previously published meta-analysis studying both BMS and DES versus CABG showing no differences in major adverse cardiovascular events but higher trend of stroke rates with CABG and repeat revascularization rates with PCI.30)
Go to :
MULTIVESSEL CAD
Multiple studies compared the safety and effectiveness of PCI and CABG for MVD revascularization; these studies are summarized in Table 2. Medicine Angioplasty, or Surgery Study (MASS II),4)10) Arterial Revascularization Therapies Study (ARTS),9) and Stent or Surgery (SoS)31)32) trials compared BMS and CABG for MVD revascularization. MASS II trial included a total of 605 patients with MVD randomized to medical therapy, CABG, or PCI. At 10-year follow-up, patients had a 1.46-fold increase in cardiovascular events with PCI compared to surgery driven by higher rates of Q-wave MI (13.3% vs. 10.1%; p<0.010) and repeat revascularization (41.9% vs. 7.1%, p<0.001). The larger ARTS trial enrolled 1,205 patients with MVD and showed a similar 5-year rate of death, MI, and/or stroke (18.2% in PCI vs. 14.9% in CABG; p=0.14), but 3.46-fold higher repeat revascularization rates in the PCI group (p<0.001). SoS was the only trial showing survival benefit of CABG over PCI in 988 patients with MVD at 6 years follow-up.
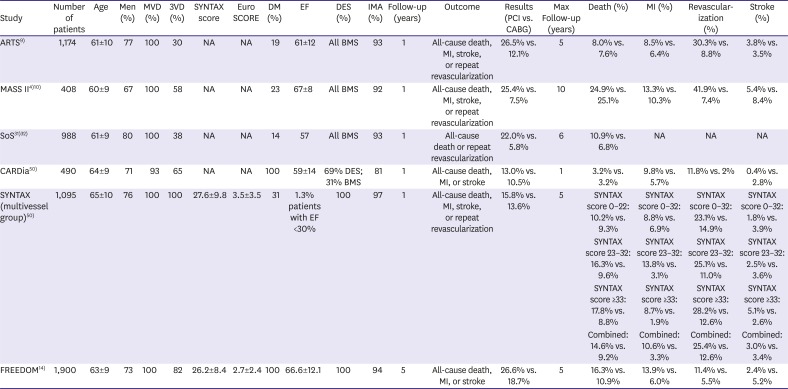
Table 2
Summary of most important randomized controlled trials in multivessel disease revascularization. Continuous variables presented as mean value±standard deviation.
| Study | Number of patients | Age | Men (%) | MVD (%) | 3VD (%) | SYNTAX score | EuroSCORE | DM (%) | EF | DES (%) | IMA (%) | Follow-up (years) | Outcome | Results (PCI vs. CABG) | Max Follow-up (years) | Death (%) | MI (%) | Revascularization (%) | Stroke (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ARTS9) | 1,174 | 61±10 | 77 | 100 | 30 | NA | NA | 19 | 61±12 | All BMS | 93 | 1 | All-cause death, MI, stroke, or repeat revascularization | 26.5% vs. 12.1% | 5 | 8.0% vs. 7.6% | 8.5% vs. 6.4% | 30.3% vs. 8.8% | 3.8% vs. 3.5% |
| MASS II4)10) | 408 | 60±9 | 67 | 100 | 58 | NA | NA | 23 | 67±8 | All BMS | 92 | 1 | All-cause death, MI, stroke, or repeat revascularization | 25.4% vs. 7.5% | 10 | 24.9% vs. 25.1% | 13.3% vs. 10.3% | 41.9% vs. 7.4% | 5.4% vs. 8.4% |
| SoS31)32) | 988 | 61±9 | 80 | 100 | 38 | NA | NA | 14 | 57 | All BMS | 93 | 1 | All-cause death or repeat revascularization | 22.0% vs. 5.8% | 6 | 10.9% vs. 6.8% | NA | NA | NA |
| CARDia50) | 490 | 64±9 | 71 | 93 | 65 | NA | NA | 100 | 59±14 | 69% DES; 31% BMS | 81 | 1 | All-cause death, MI, or stroke | 13.0% vs. 10.5% | 1 | 3.2% vs. 3.2% | 9.8% vs. 5.7% | 11.8% vs. 2% | 0.4% vs. 2.8% |
| SYNTAX (multivessel group)50) | 1,095 | 65±10 | 76 | 100 | 100 | 27.6±9.8 | 3.5±3.5 | 31 | 1.3% patients with EF <30% | 100 | 97 | 1 | All-cause death, MI, stroke, or repeat revascularization | 15.8% vs. 13.6% | 5 | SYNTAX score 0–22: 10.2% vs. 9.3% | SYNTAX score 0–32: 8.8% vs. 6.9% | SYNTAX score 0–32: 23.1% vs. 14.9% | SYNTAX score 0–32: 1.8% vs. 3.9% |
| SYNTAX score 23–32: 16.3% vs. 9.6% | SYNTAX score 23–32: 13.8% vs. 3.1% | SYNTAX score 23–32: 25.1% vs. 11.0% | SYNTAX score 23–32: 2.5% vs. 3.6% | ||||||||||||||||
| SYNTAX score ≥33: 17.8% vs. 8.8% | SYNTAX score ≥33: 8.7% vs. 1.9% | SYNTAX score ≥33: 28.2% vs. 12.6% | SYNTAX score ≥33: 5.1% vs. 2.6% | ||||||||||||||||
| Combined: 14.6% vs. 9.2% | Combined: 10.6% vs. 3.3% | Combined: 25.4% vs. 12.6% | Combined: 3.0% vs. 3.4% | ||||||||||||||||
| FREEDOM14) | 1,900 | 63±9 | 73 | 100 | 82 | 26.2±8.4 | 2.7±2.4 | 100 | 66.6±12.1 | 100 | 94 | 5 | All-cause death, MI, or stroke | 26.6% vs. 18.7% | 5 | 16.3% vs. 10.9% | 13.9% vs. 6.0% | 11.4% vs. 5.5% | 2.4% vs. 5.2% |
ARTS = Arterial Revascularization Therapies Study; BMS = bare-metal stent; CABG = coronary artery bypass graft; CARDia = Coronary Artery Revascularization in Diabetes; DES = drug-eluting stent; DM = diabetes mellitus; EF = ejection fraction; FREEDOM = Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease; IMA = internal mammary artery; MASS II = Medicine Angioplasty, or Surgery Study; MI = myocardial infarction; MVD = multivessel disease; NA = not available; PCI = percutaneous coronary intervention; SoS = Stent or Surgery; STS = Society Thoracic of Surgeons; SYNTAX = Synergy between PCI with TAXUS and Cardiac Surgery; 3VD = Three vessel disease.
*Second generation DESs were used; †MASS II trial involved 3 different arms (CABG, PCI, and medical therapy) for the treatment of multivessel coronary artery disease.
![]()
Subgroup analysis from SYNTAX trial looking at outcomes of 3 vessel CAD without LMD demonstrated a significantly higher 5-year MACCE in the PCI group compared to CABG arm (37.3% vs. 26.9%; p<0.001) driven by higher repeat revascularization (25.9% vs. 13.7%; p<0.001) and MI (9.8% vs. 3.7%; p<0.001) in the PCI arm. There was a non-significant trend toward higher stroke with CABG (3.7% vs. 2.4%; p=0.09). However, patients with 3 vessel disease and low anatomical complexity (SYNTAX score <22) had comparable outcomes at 5 years with either strategy.14)
A large meta-analysis included 6,055 patients with MVD patients from MASS II, ARTS, SoS, Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM) and Coronary Artery Revascularization in Diabetes (CARDia) trials demonstrated significantly lower all-cause mortality (relative risk [RR], 0.73; 95% CI, 0.62–0.89), MI (RR, 0.58; 95% CI, 0.48–0.72), and repeat revascularization (RR, 0.29; 95% CI, 0.21–0.41) in patients treated with CABG compared to PCI over an average of 4 years of follow-up.33) There was a trend toward higher stroke rates with CABG (RR, 1.36; 95% CI, 0.99–1.86). The favorable outcomes of CABG were thought to be related to the more complete revascularization offered by surgery34)35) and the high (90%) patency rates of mammary grafts at 10 years.36)37) However, several limitations were present in this meta-analysis. First, BMS and first generation DES were used in the PCI arms which could potentially add to the higher rates of repeat revascularization. Moreover, a large percentage of patients included in the meta-analysis were diabetic by the inclusion of FREEDOM and CARDia trials; stents are known to be associated with inferior clinical outcomes in diabetic patients with higher rates of TLR and cardiac events. Clinical outcomes were not described based on anatomical complexity such as SYNTAX score. Lastly, physiologic assessment of stenosis using fractional flow reserve was not performed in these trials which could have resulted in further reduction in repeat revascularization in the PCI group.38)
Several studies have shown that second generation DESs have lower TLR compared to first generation stents and their use is considered the standard of care in MVD PCI. As for CABG, full arterial grafting was once considered a promising strategy for CABG given the theoretical advantage of arterial grafting as compared to saphenous vein grafts (SVGs). However, the results of the large Arterial Revascularization Trial (ART), which enrolled 3,102 patients who underwent CABG for MVD, raised questions regarding this strategy. The trial failed to show significant differences in all-cause death, MI, or stroke at 10 years (12.7% for single mammary vs. 12.1% for bilateral mammary; p=0.69).39) Bilateral mammary utilization was also associated with worse wound healing outcomes. Similar patency rates at 1 year were also observed among 11 Veterans affairs centers enrolling patients for radial versus SVG during CABG.40) The Canadian multicenter Radial Artery Patency Study (RAPS),41) which enrolled 163 patients for radial versus SVG grafting, did not show differences of the rates of ≥50% stenosis in the radial grafts and SVG at 5-year. However, the burden of graft stenosis was significantly higher in the SVG arm compared to radial graft arm suggesting potential better long-term patency with radial grafts. Longer follow-up is warranted to help guide best grafting strategies in CABG in MVD.
Hybrid coronary revascularization by combining minimally invasive coronary artery bypass (MICAB) with arterial graft and non-LAD multivessel PCI emerged as potential favorable strategy to overcome the shortcomings of vein grafts which have <50% patency rates over 10 years42) by placement of durable second generation DES which have a low risk of restenosis (<5% per 1 year). Hybrid revascularization was shown to be safe and feasible in small observational studies.43) In a multicenter observational study, Puskas et al.44) compared 200 patients who underwent hybrid procedure versus 98 patients with MVD PCI. The composite rates of all cause death, MI, stroke, and repeat revascularization over 18 months were not significantly different (HR, 0.86; p=0.56). Most recently, preliminary results from the Hybrid Revascularization Versus Standards (HRVES) trial were presented at Transcatheter Cardiovascular Therapeutics. This trial enrolled 155 patients with MVD who underwent PCI, hybrid approach, or CABG for revascularization. The study showed similar reduction in ischemia at 12 months measured by single photon emission computed tomography (SPECT) in all revascularization arms. Clinical outcomes were similar but the study was not powered to detect outcomes such as MACCE. A large multicenter randomized controlled trial is currently enrolling patients with MVD to Hybrid versus multivessel PCI to further shed the lights on safety and effectiveness of this treatment approach over 5 years follow-up.
Go to :
QoL AND COST-EFFECTIVENESS OF REVASCULARIZATION STRATEGIES
QoL is an important metric when comparing revascularization strategies. In the SYNTAX trial, angina relief using the Seattle Angina Questionnaire (SAQ) and physical function were improved with CABG compared to PCI, but the absolute benefit was small at 5 years.45) In patients with high SYNTAX score, angina relief was more pronounced with CABG. Treatment with CABG was also associated with further improvement of New York Heart Association (NYHA) score in NOBLE trial, but no statistical differences were observed in Canadian Cardiovascular Society (CCS) class score between the 2 revascularization strategies.16) Such results could be explained by the more complete revascularization offered by CABG compared to PCI. In the EXCEL trial, short term QoL at 1 month was better with PCI; however, no significant difference was seen at 3 years.46)
Both treatment strategies account for about $12 billion direct cost yearly in United States. Results from SYNTAX studies47)48) showed higher initial hospitalization cost $10,036 per patient with CABG for LM or 3 vessel disease, but the overall costs were higher with PCI over 5 years likely driven by higher rates of repeat revascularization, higher rates of hospitalization, and higher medication costs. However, no differences in cost were observed when patients with LMD or MVD with low SYNTAX score were analyzed underscoring the importance of heart team approach and integrating SYNTAX scores to apply the most appropriate and cost-effective treatment for each patient.
Go to :
SPECIAL POPULATIONS
Patients with diabetes mellitus
Patients with diabetes represent a high-risk group for cardiovascular events and death. Subgroup analysis in SYNTAX trial revealed higher cumulative cardiovascular events in patients with than without diabetes.49) The CARDia trial was the first trial comparing PCI vs. CABG for MVD revascularization in patients with diabetes.50) The study included 510 patients and revealed inferiority of PCI as revascularization strategy in MVD and diabetes at 1 year (cumulative cardiovascular events of death, MI, stroke was 13.0% in PCI vs. 10.5% in CABG group; p=0.39 for non-inferiority). In the larger FREEDOM trial,51) CABG led to 8% absolute risk of reduction in cumulative cardiovascular events compared to PCI with DES driven by lower rates of mortality and nonfatal MI at 5 years. The stroke rates were higher with CABG at 5.2% compared to 2.4% with PCI (p=0.03) during 5-year follow-up. The favorable results of CABG are likely attributed to the high patency rates for the left internal mammary grafts. The DES utilized in FREEDOM was first generation which could lead to inferior PCI results; however, no substantial improvement in clinical outcomes was offered by second generation DES compared to first generation in large meta-analysis studying both stents in diabetic patients.52)
Patients with reduced ejection fraction
Patients with reduced ejection fraction secondary to ischemic heart disease have higher risk for cardiovascular events and mortality approaching 60% over 10-year follow-up with guideline directed medical therapy alone.6) Nevertheless, patients with reduced ejection fraction were seldom included in the RCT. Therefore, less evidence is available to guide the best revascularization approach in patients with reduced ejection fraction. An individual data meta-analysis by Wolff et al.53) included 16,191 patients with CAD and left ventricular ejection fraction (LVEF) ≤40% from 21 studies mostly observational registries showed reduction in mortality with CABG (HR, 0.66; 95% CI, 0.61–0.72; p<0.001) and PCI (HR, 0.73; 95% CI, 0.62–0.85; p<0.001) compared to medical therapy. CABG was also associated with lower mortality (HR, 0.82; 95% CI, 0.75–0.90; p<0.001) compared to PCI. However, the results should be interpreted with caution given the observational nature of the studies. The results on the other hand are not surprising as these patients theoretically extract more benefit from complete revascularization with CABG. The Surgical Treatment for Ischemic Heart Failure (STICH) trial was the only prospective randomized study comparing revascularization with CABG versus guideline directed medical therapy for patients with CAD amenable for surgery and LVEF ≤35%. The primary outcome studied was death from any cause. While both treatment strategies among 1,212 enrolled patients were associated with similar survival at 6 years,5) CABG led to 7% and 9% absolute risk reduction in all-cause mortality and cardiovascular related mortality at 10 years follow-up.6) However, the study did not have PCI arm; therefore, most of evidence of PCI in ischemic cardiomyopathy is based on observational studies.
Patients with chronic kidney disease (CKD)
Patients with advanced CKD are seldom studied in RCT. Overall revascularization is underutilized in patients with CKD given concern for acute renal failure, and bleeding risk, beside the additional periprocedural complications from significant coexisting comorbidities. Data from Alberta Provincial Project for Outcomes Assessment in Coronary Heart Disease (APPROACH) registry including 41,786 who underwent cardiac catheterization in Alberta, Canada has shown significant significantly improved 8-year survival with CABG or PCI when compared to medical therapy alone in dialysis and non-dialysis patients with advanced kidney disease and CAD.54) Another cohort involving 21,981 patients with ESRD and CAD from the US Renal Data System showed poor 5-year survival approaching 25% regardless of revascularization strategy; however, CABG was associated with lower mortality compared to PCI with BMS.55) In general, revascularization strategy in this highly comorbid population should be offered based on patient surgical risk assessed by Society Thoracic of Surgeons (STS) score or EuroSCORE, frailty, life expectancy, and anatomical complexity measured by SYNTAX score. DES should be offered if patients undergo PCI given its reduced rates of TLF compared to BMS.56) Moreover, off-pump bypass should be considered in patients undergoing CABG since it is associated with lesser degree of acute renal failure and acute morbidity and mortality.57)58)
Elderly patients
In 1990, the US census stated that 12.5% of the total population are 65 years of age or older; It is expected that elderly patients will increase by 65% in 2020 to 52 million in US only. Nevertheless, the elderly population is underrepresented in clinical trials. There are multiple challenges with revascularization of elderly including frailty and complexity of CAD with calcified, chronically occluded and tortuous vessels, as well as higher risk for bleeding complications, especially with antiplatelets and anticoagulation agents. Moreover, elderly patients have significant comorbid conditions that potentially increases their risk for periprocedural complications such as stroke and acute renal failure.
The optimal revascularization technique is unclear, especially in the absence of direct comparisons between PCI and CABG in the elderly. Data from APPROACH registry59) showed that PCI is usually offered to patients with significant comorbidity and frailty and CABG to patients with more complex CAD. The 4-year survival for 70–79 and ≥80 years old patients were 87.3% with CABG and 83.9% with PCI and 77.4% with CABG and 71.6% with PCI respectively. In the Angina With Extremely Serious Operative Mortality Evaluation (AWESOME)60) trial comparing older PCI and CABG technologies, half of the patients studied were older than 70 years of age. The 3-year survival was 80% in PCI and 79% in CABG with a trend toward increased in-hospital mortality in CABG. However, PCI was associated with higher rates of repeat revascularization at 3 years. Similar trade-off of increased 30 days mortality in CABG versus PCI (7.2% vs. 5.4%) and trend toward higher 5-year survival with CABG compared to PCI (68% vs. 62%) was seen in a meta-analysis of 66 older studies focusing on revascularization in patients 80–89 years of age.61) There are no randomized trials comparing safety and efficacy of newer PCI technologies compared to CABG in this population. In the DESs in elderly patients with coronary artery disease (SENIOR)62) trial, DES with short duration of DAPT was compared to BMS for revascularization in 1,200 elderly patients. DES was associated with significant 4% absolute risk reduction of all cause death, MI, stroke, or repeat revascularization at 1 year.
QoL is a very important measure for elderly patients when considering revascularization. Both PCI and CABG strategies have been associated with improved QoL when compared to medical therapy. Trial of invasive versus medical therapy in elderly patients with chronic symptomatic CAD (TIME)63) was the only randomized study comparing invasive (CABG or PCI) versus intensified medical therapy for the treatment of patients ≥75 years of age with CCS class II angina. Revascularization strategies were associated with significant improvement in angina beside reduction in ACS related hospitalization. Moreover, at 1 year, 43% of patients received intensified medical treatment underwent revascularization.
Go to :
CURRENT RECOMMENDATIONS FROM GUIDELINES
European Society of Cardiology (ESC)64) and American Heart Association/American College of Cardiology (ACC/AHA)65)66) guidelines stressed the importance of heart team approach in determining the best revascularization strategy in each case. The assessment of surgical and PCI risks using STS score, EuroScore and SYNTAX score were strongly encouraged. The guidelines also indicated the absence of rigorous randomized controlled trials in CKD, women, and elderly population making it very difficult to provide strong recommendation on best treatment strategy in these circumstances. Both and ESC and ACC/AHA guidelines provided class I recommendation for CABG as preferred revascularization strategy in patients with left ventricular (LV) dysfunction; AHA/ACC document stated that there is insufficient data to recommend PCI in the setting of LV dysfunction; while ESC guidelines gave class IIb recommendation for PCI in patients with LV dysfunction and suitable anatomy. The Europeans upgraded recommendation from class IIb for left main and 3 vessels PCI in patients with low SYNTAX score to class I (Figure 1) given comparable cardiovascular outcomes with PCI and CABG in SYNTAX trial.
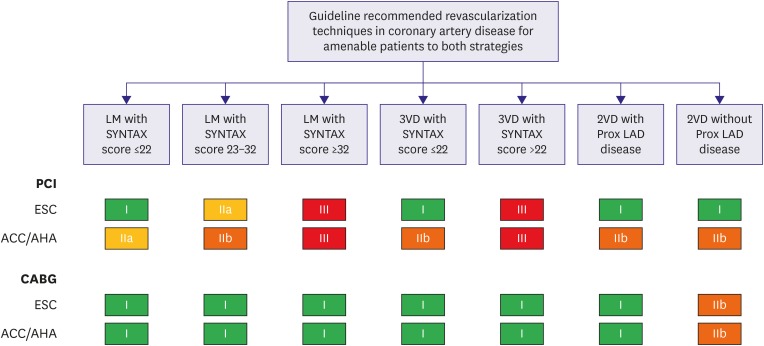 | Figure 1Comparison of ACC/AHA and ESC guidelines recommendations on LMD and MVD revascularizations. Class I: revascularization strategy is recommended or should be performed. Class IIa: revascularization strategy is reasonable and can be useful. Class IIb: revascularization strategy might be reasonable or considered. Class III: revascularization strategy is not recommended.
ACC/AHA = American College of Cardiology/American Heart Association; CABG = coronary artery bypass graft; ESC = European Society of Cardiology; LM = left main; LMD = left main disease; MVD = multivessel disease; PCI = percutaneous coronary intervention; SYNTAX = Synergy between PCI with TAXUS and Cardiac Surgery; 2VD = two vessel disease; 3VD = three vessel disease.
|
Go to :
SUMMARY
Currently, evidence from the literature indicates the importance of both treatment strategies for the management of LMD and MVD. Both revascularization techniques are viable options when selecting the right patient (Figure 2). Each patient should be evaluated using heart team approach, with primary provider, anesthesiologist, interventional cardiologist, and cardiac surgeon. Systematic assessment for feasibility of either strategy, patient ability to recover from surgery and her/his tolerance to medical therapy should be performed during heart team evaluation. Moreover, patient preferences and shared decision making is prudent in choosing the best revascularization strategy. CABG is associated with superior long-term clinical outcomes and more cost effective in patients with complex anatomy and high SYNTAX score. However, not all patients will be candidates for surgery. Both approaches could be instituted in cases with low to intermediate SYNTAX score in LMD and low SYNTAX score in MVD. PCI is associated with lower periprocedural events at 30 days, but significant increase in repeat revascularization rates at 5 years. Moreover, patients should understand that mortality over 5 years is similar if they undergo either treatment; however, longer term data are not available yet. Finally, hybrid revascularization with MIDCAB and non-LAD multivessel PCI is an appealing strategy currently being tested in large randomized controlled trial.
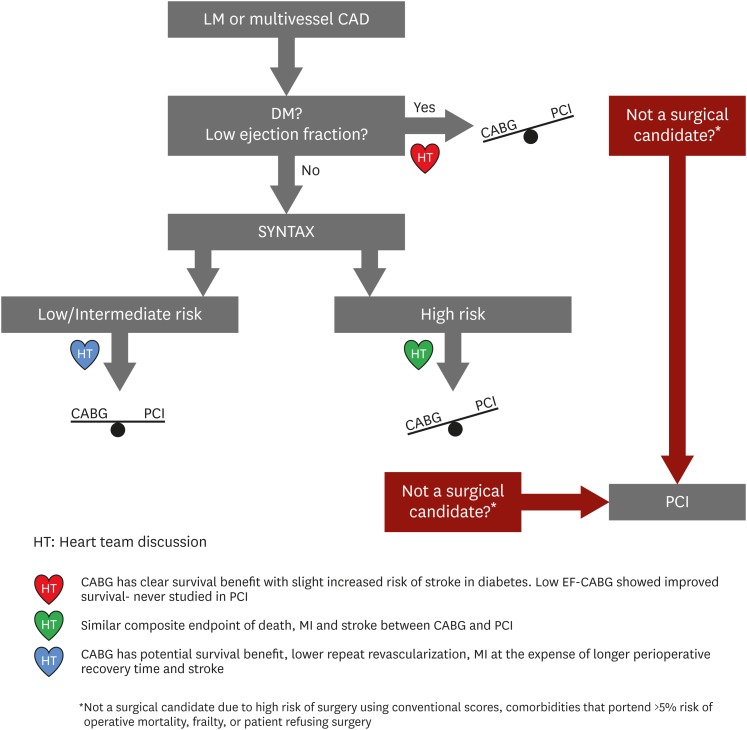 | Figure 2Algorithm integrating heart team approach and evidence from literature to determine best revascularization strategies.
CABG = coronary artery bypass graft; CAD = coronary artery disease; DM = diabetes mellitus; EF = ejection fraction; ESC = European Society of Cardiology; LM = left main; MI = myocardial infarction; PCI = percutaneous coronary intervention; SYNTAX = Synergy between PCI with TAXUS and Cardiac Surgery.
|
Go to :
 XML Download
XML Download