

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Liver transplantation (LT) is an established treatment for patients with liver cirrhosis and/or hepatocellular carcinoma (HCC). Patient selection according to institutional eligibility criteria contributes to reduction of HCC recurrence after LT, but a considerable number of LT recipient deaths are still associated with HCC recurrence.12345 HCC recurrence usually happens during the first a few years after LT, although very late recurrence has been reported sporadically. Because of the rarity of very late HCC recurrence that occurs at least 10 years after transplantation,67 early detection is difficult and a therapeutic strategy for such tumors has not yet been established. Currently, there are no clear recommendations or consensuses for the management of recurrent HCC, particularly peritoneal metastasis. Here, we describe two cases of peritoneal metastasis of HCC that occurred 10 and 12 years after LT and discuss a therapeutic strategy for such patients.
Go to : 
CASE
Case 1
A 67-year-old male underwent deceased-donor LT for hepatitis B virus-associated liver cirrhosis and HCC (Fig. 1A and 1B). Before LT, the patient underwent two sessions of transarterial chemoembolization and one session of radiofrequency ablation. The extent of HCC within the explanted liver met the Milan criteria. The pre-transplant serum α-fetoprotein (AFP) level was 7 ng/ml.
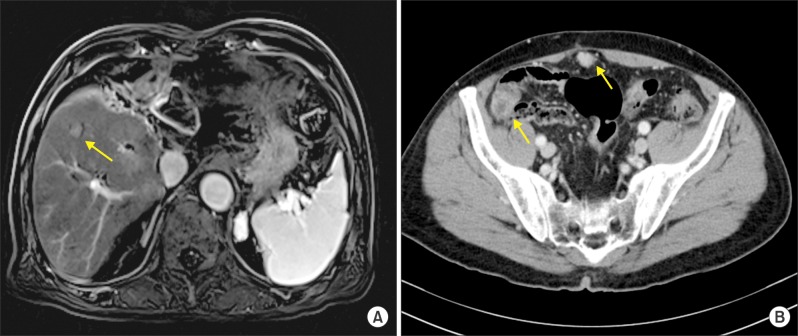
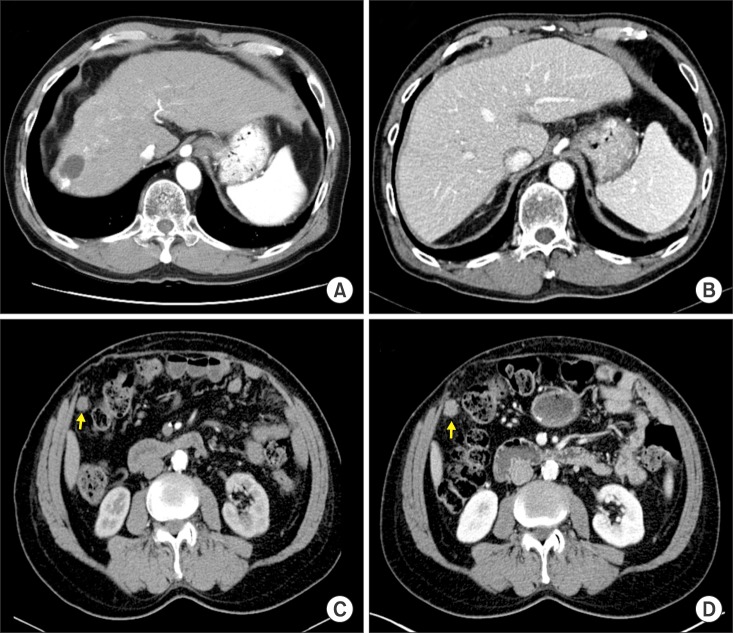 | Fig. 1Computed tomographic images of Case 1. (A) Pre-transplant finding. (B) Early posttransplant finding. (C) Image taken 2 months before the diagnosis of HCC recurrence. The arrow indicates the metastatic lesion. (D) Image taken at the time of diagnosis of HCC recurrence. The arrow indicates the metastatic lesion.
|
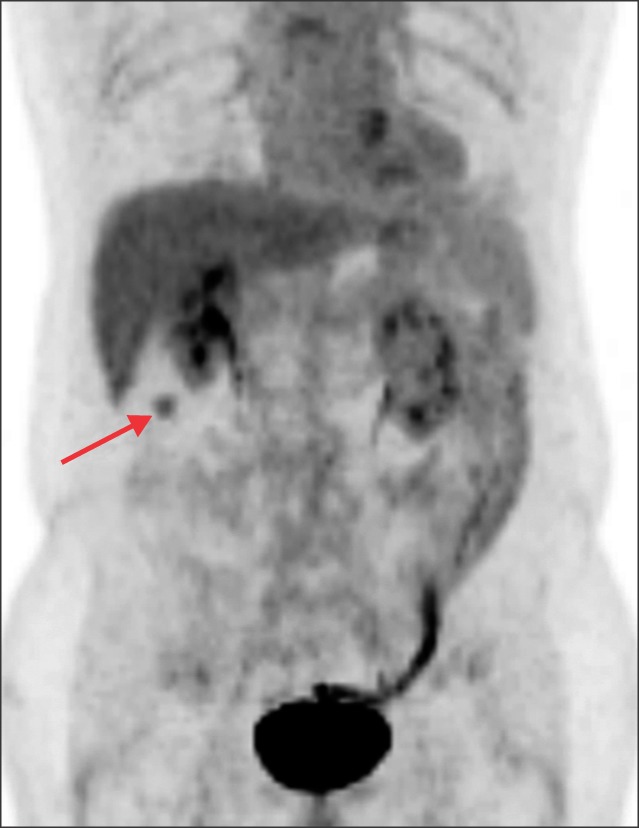
At the age of 77 years (10 years after LT), the patient showed slow elevation of tumor marker levels during 6 months of outpatient clinic follow-ups. Because of slow but progressive elevations of the levels of AFP and protein induced by vitamin K antagonist or absence-II (PIVKA-II) (Fig. 2), the patient was closely observed by bimonthly computed tomography (CT) analyses of the chest and abdomen-pelvis, as well as monthly tumor marker tests. After observation for 6 months, a single 2 cm-sized mass was found around the transverse colon (Fig. 1C and 1D). The lesion was visible on the CT scan taken 2 months previously, but we had missed it at that time (Fig. 1C). There was only a slight growth of the mass during the 2 month period. A positron emission tomography (PET) scan using [18F]-fluorodeoxyglucose revealed that the mass showed hypermetabolic uptake (Fig. 3). During this work-up, serum levels of AFP and PIVKA-II were gradually elevated. These findings suggested that the mass was likely to be metastatic HCC.

Open laparotomy was performed, and the mass was excised with tumor-negative resection margins. A pathological analysis confirmed that the mass was metastatic HCC. After excision, the patient's tumor marker levels rapidly returned to normal ranges (Fig. 2). Considering his age of 77 years, the patient was prescribed everolimus monotherapy and half-dose sorafenib therapy (200 mg twice per day). Over the past 10 months, he has been doing well and has not shown any serious adverse side-effects or signs of HCC recurrence. In this patient, tumor marker testing is highly diagnostic and the current surveillance protocol comprises tumor marker tests every 2 months and CT scans every 6 months.
Case 2
A 53-year-old male underwent living-donor LT for hepatitis B virus-associated liver cirrhosis and HCC (Fig. 4A and 4B). Before LT, he did not receive any HCC treatment. The resected liver had a single 1.5 cm-sized HCC without microvascular invasion, and therefore met the Milan criteria. The pretransplant serum AFP level was 16 ng/ml.
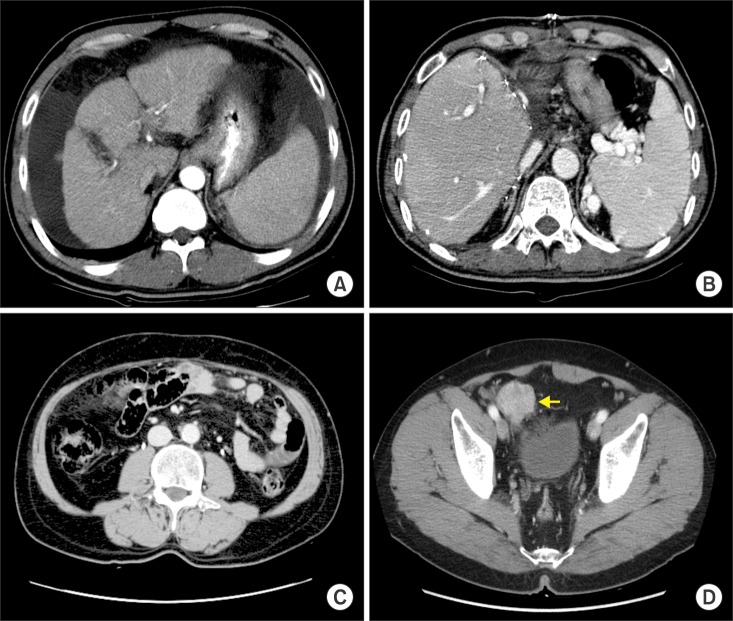
At the age of 65 years (12 years after LT), the patient showed very slow elevation of AFP levels, albeit within the normal range, over 3 months of outpatient clinic follow-ups (Fig. 5A). A CT scan of the abdomen was taken 6 months prior to the observed increase in AFP levels, but no abnormalities were detected (Fig. 4C). The pelvis was not examined at that time. A subsequent CT scan of the abdomen-pelvis was performed after detection of the slow rise in the AFP level and identified a 4 cm-sized mass at the pelvis (Fig. 4D). A PET scan using [18F]-fluorodeoxyglucose revealed that the mass showed hypermetabolic uptake (Fig. 6). At this time, the AFP level was gradually elevated but was still within the normal range (Fig. 5A). These findings suggested that the mass was likely to be metastatic HCC.


Open laparotomy was performed, and two masses were excised with equivocal tumor-negative resection margins (Fig. 7). A pathological analysis confirmed that the masses were metastatic HCCs. After excision, the patient's AFP level dropped rapidly (Fig. 5A); however, 6 months later, it increased again, although it was still within the normal range. Follow-up CT and PET scans revealed multiple seeding nodules at the pelvis (Fig. 8). The patient underwent treatment with low-dose calcineurin inhibitor, sirolimus, and full-dose sorafenib, and displayed no serious adverse side-effects. Growth of the peritoneal seeding nodules was visualized on follow-up CT scans, and sorafenib therapy was stopped after 2 years of administration. The patient changed to receive everolimus monotherapy because its Korean National Health Insurance coverage for LT recipients. During the 6 years since HCC recurrence was diagnosed, the patient has shown very slow growing tumors, alongside elevated AFP levels (Fig. 5B and Fig. 9), but has been doing well without significant deterioration of his quality of life. Recently, he has been hospitalized twice due to deterioration of his general condition. We expect that supportive care will prolong his life further.
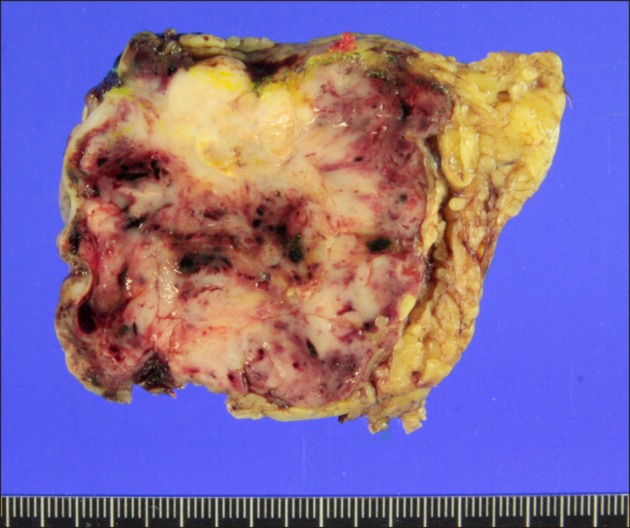 | Fig. 7Gross image of the resected metastatic mass with equivocal tumor-negative resection margins in Case 2.
|

Go to :
DISCUSSION
Although the majority of HCC recurrence happens during the first a few years after LT, a small number of patients display very late recurrence, sometimes as late as 10 years after transplantation. Advanced HCC beyond the Milan criteria is often associated with early HCC recurrence; however, like the two cases described here, the majority of patients showing late recurrence have HCCs within the Milan criteria.6 Because of its rarity, early diagnosis of delayed or very late HCC recurrence is difficult to detect. In the real-world practice, such very late recurrence is often diagnosed after overt manifestation of symptoms, or is incidentally detected during routine follow-up studies. From 10 years post-transplantation onwards, our institution performs surveillance imaging of LT recipients once every 2 years. This interval period, which was determined based on cost-effectiveness and patient compliance, makes it difficult to detect delayed HCC recurrence at an early stage.
Measurement of serum AFP levels is a simple test that can be done during outpatient clinic visits. In patients who had elevated AFP levels prior to LT, there is a high probability of AFP elevation at the time of HCC recurrence. In fact, we reported previously that the ability of AFP testing to detect post-transplant HCC recurrence is dependent on the pretransplant AFP levels; specifically, we reported HCC detection sensitivities of approximately 40%, 50%, and 90% in patients with pretransplant AFP levels of ≤20 ng/ml, 21–200 ng/ml, and >200 ng/ml, respectively.6 Detection of PIVKA-II levels plays a complementary role in the diagnosis of HCC, although the sensitivity and specificity of PIVKA-II testing are lower than those of AFP testing.8910 Concurrent measurement of AFP and PIVKA-II levels improves the sensitivity of HCC recurrence detection; therefore, we have measured the levels of these proteins during follow-up analyses of HCC patients, including LT recipients, since 2006. In a Japanese study of patients with HCC in the explanted liver, AFP and PIVKA-II levels were measured every 1–2 months after LT, but confirmation of HCC recurrence via imaging took 17–208 days after the observed increases in the levels of tumor markers.11
Compared with those that recur early, post-transplant HCCs showing very late recurrence may have less aggressive tumor biology and may be more responsive to locoregional treatments. However, we emphasize that post-transplant HCC recurrence itself is a strong evidence of aggressive tumor biology. Thus, the therapeutic strategy for very late HCC recurrence is similar to that for early recurrence. Surgical resection of metastatic lesions is the most effective therapy for recurrent HCC in LT recipients. We previously reported a beneficial effect of surgical metastasectomy of metachronous pulmonary and adrenal metastases from HCCs on patient survival.1213 There are only a small number of studies supporting resection of tumors arising from peritoneal seeding of HCC, and resection of peritoneal metastases should only be considered in patients whose primary liver neoplasm is under control and who have no metastases in other organs.141516 Since there was no evidence of tumor recurrence other than localized peritoneal metastasis in the two cases described here, we decided to perform peritoneal metastasectomy in both patients.
In LT recipients with HCC recurrence, metastasectomy is not considered to be curative because it can be compatible with local control methods. There is a high probability of further tumor recurrence from residual tumor cells, as well as inevitable immunosuppression. Thus, conversion to treatment with a mammalian target of rapamycin (mTOR) inhibitor and systemic therapy with sorafenib should be considered in these patients. Alongside their immunosuppressive effects, which are mediated via inhibition of interleukin-2-mediated T-cell proliferation,17 mTOR inhibitors display antitumor effects by inhibiting cell growth and angiogenesis. Treatment with the mTOR inhibitor everolimus is associated with a low rate of HCC recurrence in LT recipients.181920 However, to date, the majority of clinical LT studies have focused on the prevention rather than the treatment of established HCC recurrence. In the cases described here, we switched the primary immunosuppressant therapy to mTOR inhibitor after HCC recurrence and de novo malignancy; however, there is still a lack of strong evidence supporting immunosuppressive treatment regimens using mTOR inhibitors.18192021
The multikinase inhibitor sorafenib is an effective therapy for HCC.2223 Although sorafenib noticeably improves the survival of patients with advanced HCC,2425 its potential mechanisms of action are not well known. It is not recommended to use sorafenib as an adjuvant therapy for HCC following hepatic resection or ablation,26 and its therapeutic effect on post-transplant HCC recurrence is still largely unknown.2728 However, we reasoned that metastasectomy of post-transplant recurrent HCC is associated with a high risk of further recurrence in LT recipients; thus we administered sorafenib as an adjuvant chemotherapy in the two cases described here.
Combination therapy with sorafenib and mTOR inhibitor, in addition to locoregional treatment, has been performed previously. A Korean single institution study found that 12 patients who received combination therapy with sorafenib and sirolimus had better post-recurrence survival outcomes than 27 patients receiving best supportive care for post-transplant HCC recurrence.29 Furthermore, in a Spanish multi-center study involving 31 LT recipients with HCC recurrence, combination therapy resulted in a partial response in a single patient and stable disease in 13 patients, giving an overall clinical benefit rate of 53.8%.30
Lifelong surveillance is necessary for LT recipients because HCC recurrence can occur after prolonged periods, as highlighted in the two cases described here. Since most recurrences are diagnosed subclinically, surveillance via frequent tumor marker testing is the cornerstone of follow-up studies to detect HCC recurrence in a timely manner.
In conclusion, very late peritoneal metastasis of HCC happens sporadically. We suggest that the therapeutic modality for this condition includes local control through surgical resection if possible, everolimus monotherapy, and long-term use of sorafenib.
Go to :
 XML Download
XML Download