

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Increased life expectancy is a global trend; over the past two decades, the mean life expectancy has increased from 64 to 71 years of age, and moreover, the mean life expectancy in high-income countries has increased to nearly 80 years.1 The incidence of cancer increases with age, generating an increased interest in treatments for elderly individuals,2 and therefore, researchers have conducted many studies on surgeries for elderly patients with cancer; clinicians have found that most such surgeries are both safe and feasible, with immediate surgical complications, mortality rates, and long-term outcomes comparable with those in younger patients.3456
Researchers have also reported in multiple studies the efficacy of radical surgery for elderly patients with periampullary adenocarcinoma, and some have reported that selected elderly patients could have similar perioperative outcomes and overall survival (OS) to those in younger adults, although others have shown increased morbidity and mortality in elderly versus younger patients.78910 In short, the efficacy of surgery for elderly patients with periampullary adenocarcinoma remains a controversial issue in the hepato-pancreato-biliary surgery field.
There are a number of causes for the controversy. Periampullary cancer tends to occur later in life than other malignancies: The median age at diagnosis is about 70 years.21112 Moreover, pancreatoduodenectomy, the radical surgery that is generally performed for such cancers, causes more morbidity and mortality and results in poorer prognoses than do treatments for other gastrointestinal cancers.213 Therefore, advanced age has been associated with decreased utilization of surgery to treat periampullary cancer, and the mean age of patients who undergo surgery has remained unchanged over the past decade.14
In recent decades, surgical techniques and postoperative care have significantly improved, and morbidity and mortality after radical surgery have decreased dramatically while mean life expectancy has increased.11315 Moreover, radical surgery remains the only potentially curative treatment for periampullary cancer.16 Therefore, it is necessary to evaluate radical surgery for periampullary cancer in elderly patients in light of the recent improvements in techniques. We investigated the oncologic outcomes of periampullary cancer in octogenarians, comparing patients who did not receive surgery with those who underwent radical surgery.
MATERIALS AND METHODS
We retrospectively reviewed the medical records of 133 patients over 80 years of age who were diagnosed with periampullary cancer from January 2005 to December 2014. We excluded 65 patients who were not able to have radical surgery at the time of diagnosis (e.g., those with distant metastasis) or who were not confirmed by pathology to have periampullary cancer, and we divided the remaining patients into two groups based on whether or not they underwent radical surgery. The surgical criteria for the elderly patients were the same as those for non-elderly patients, and those who were deemed to be operable through preoperative study underwent the surgery. We analyzed immediate postoperative complications and mortality in the patients who had surgery and compared the OS period between the patients who underwent surgery and those who did not.
We used SPSS version 20.0 (IBM Corp., Armonk, NY, USA) for all statistical analyses, and we compared nominal data with χ2 tests, continuous parametric data with t-test, and nonparametric data with Mann-Whitney U tests. We assessed survival parameters by the Kaplan-Meier method and compared them using the log-rank test. The criterion for statistical significance was p<0.05.
RESULTS
Patient distribution
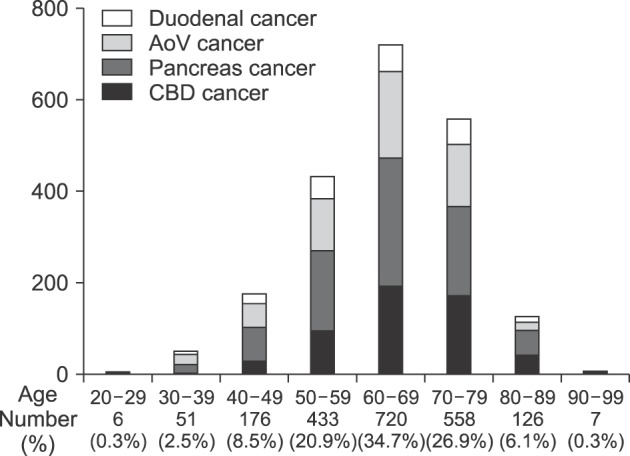
From January 2005 to December 2014, 2,077 patients were diagnosed with periampullary cancer in our hospital, and among them, 133 (6.4%) were over 80 years of age. More than half of the patients were age 60 to 70 (1,278 patients, 61.6%), and the oldest patient with pancreatic cancer was 96, although that patient was inoperable at the time of diagnosis (Fig. 1).
Baseline patient characteristics
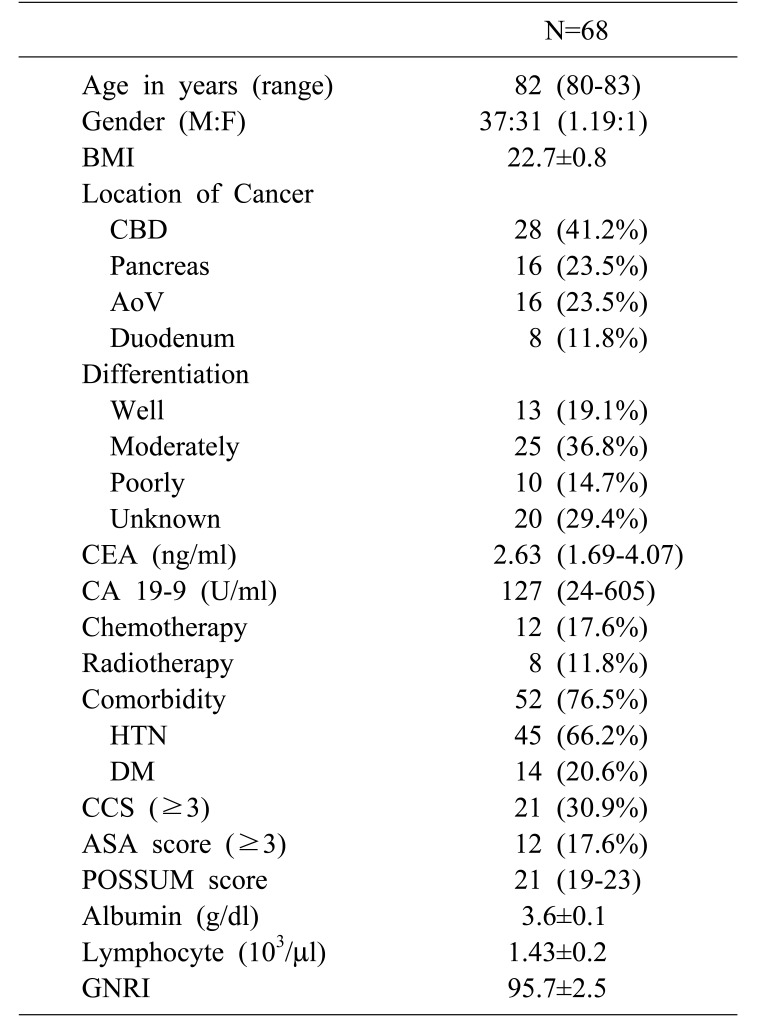
The clinicopathologic characteristics of the 68 patients over age 80 who were diagnosed with periampullary cancer are shown in Table 1. The median patient age was 82 years, and the oldest was 90; this patient was in the surgery group. Fifty-two patients (76.5%) had at least one comorbidity. The mean geriatric nutritional risk index (GNRI) was 95.7 (95% confidence interval [CI]: 93.2–98.2).
Characteristics of the non-surgery group
Most patients (n=31, 72.1%) refused the surgery due to their old age, and the other patients' data did not exist in the medical records (n=12, 27.9%). Among the patients who refused the surgery, 14 decided independently, and family members made the decision for the other 17 (Fig. 2).
Clinicopathologic characteristics according to radical surgery
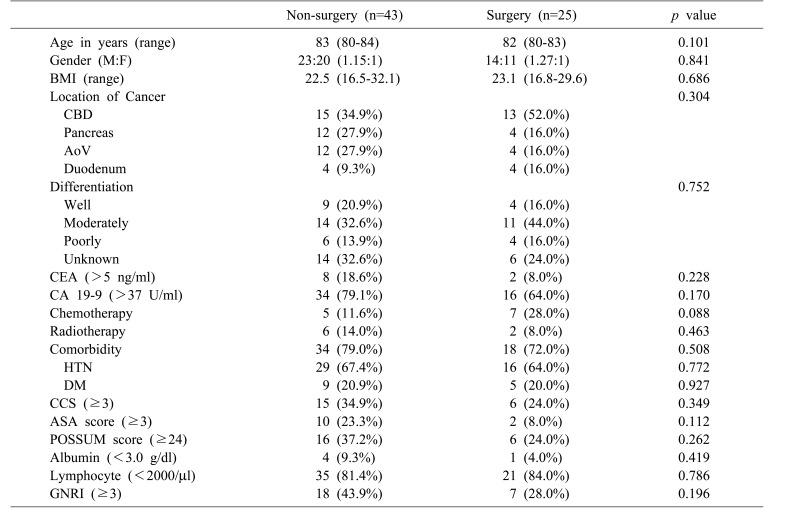
We divided the 68 patients into two groups based on whether or not they underwent radical surgery. Forty-three patients did not undergo surgery, and the other 25 did, and there was no significant difference in median age between the two groups (non-surgery: 83 years, surgery: 82; years p=0.101). There were also no significant differences in tumor characteristics (tumor location and differentiation), comorbidity status (Charlson comorbidity score [CCS] and American Society of Anesthesiologist [ASA] classification), or nutritional status including GNRI (Table 2).
Characteristics of the surgery group
Most of the patients who underwent radical surgery were within TNM stage II; only two were beyond stage II, and both of them were confirmed to have duodenal cancer (Fig. 3A). Twenty-two patients (88.0%) had immediate postoperative complications; however, most of the complications were minor, and only five (20.0%) had major complications that exceeded Clavien-Dindo grade III17 (Fig. 3B). Between the elderly and non-elderly (n=678) groups, there were no significant differences in complication rates (elderly: 11.5%, non-elderly: 20.0%; p=0.202).
Oncologic outcomes of elderly patients
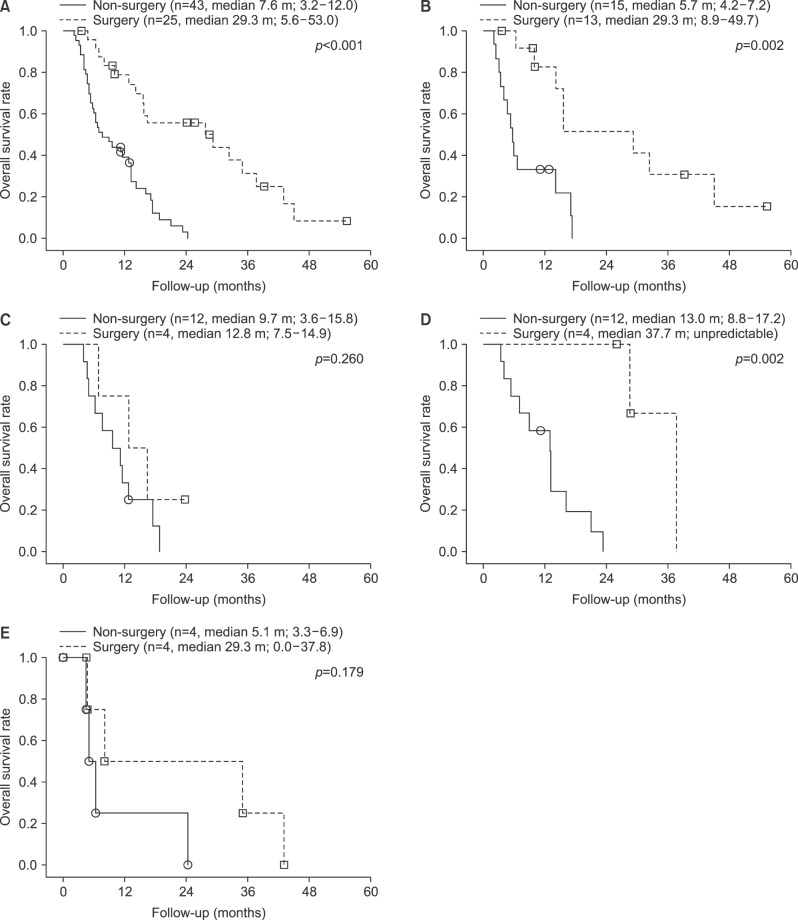
The mean OS was 37.7 months (range: 26.1–49.3 months), and there was a significant difference in OS between the two groups (non-surgery vs. surgery: 7.6 months vs. 29.3 months; p<0.001). Fifty-six patients (82.4%) expired, and all of the causes of death were cancer related (Fig. 4A).
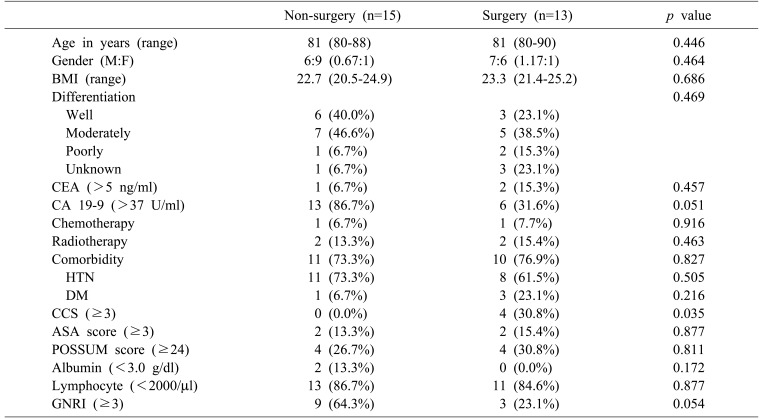
Subgroup analysis showed that patients with common bile duct (CBD) cancer who underwent surgery (n=13) had better OS than did those with CBD cancer who did not (n=15): 5.7 months vs. 29.3 months (p=0.002). However, there were no significant differences between the two groups in clinicopathologic parameters except for CCS (non-surgery vs. surgery: 0.0% vs. 30.8%, p=0.035; Table 3). Comparisons among other subgroups either showed no significant differences between patients in the surgery and non-surgery groups or could not provide statistical results because of the small sample sizes of the subgroups (Fig. 4B–E).
DISCUSSION
As the human body ages, there is a progressive decline in physiologic functioning that affects all organ systems and places elderly individuals at increased risk of disease. Although the gastrointestinal system is less affected than other systems, aging can lead to a decline in metabolism, 18 and moreover, aging is a risk factor for most cancers. There is abundant literature that explains the relationship between aging and cancer. Carcinogenesis often occurs over a long period of time and is promoted by the increased susceptibility of older tissues to environmental carcinogens and by changes in the body environment that occur with aging, such as chronic inflammation and increased resistance to insulin.1920 Therefore, elderly patients should not be considered to be the same as younger patients.
There are few evidence-based guidelines for elderly patients with cancer, and oncologists are often faced with special challenges when managing these patients;21 most oncologists agree, however, that estimating life expectancy is of primary importance. In addition, clinicians should determine whether the assumed treatment benefits will likely occur within the patient's remaining life span. Because life expectancy is heterogeneous among elderly patients, it is not a simple issue to determine the likely efficacy of a given treatment; comorbidities, disability, and geriatric syndromes have a substantial impact on life expectancy.22
Because of the complexities of cancer management in elderly patients, comprehensive geriatric assessment (CGA) is in the interest of oncologists. CGA is a global, multidisciplinary approach to elderly patients that covers functional status, cognitive capacities, emotional status, comorbidities, nutritional status, polypharmacy, and social and environmental circumstances.23 Recently, several studies showed that CGA could help to adapt cancer management to each patient's fitness or frailty.2425 Although CGA can predict morbidity and mortality in elderly patients with cancer, its implications are more complex for surgical oncologists;23 surgery is one of the most invasive treatments and can cause more complications than other treatment modalities.26 Above all, radical surgery for periampullary cancer is generally associated with high morbidity and mortality rates and requires many days of hospitalization, leading to fears among surgical oncologists about treatment-related adverse effects.13
To avoid unwanted postoperative morbidity and mortality, researchers have conducted many studies on predictive preoperative indexes for elderly patients,26272829 and comorbidities are one of the risk factors. Eighty-three percent of elderly patients have at least one comorbidity, although two thirds have acceptable preoperative functional and mental status.2628 In addition, the ASA grade and the GNRI can predict postoperative complications;272930 in our study, there was no significant difference in ASA grade or GNRI between the patients who underwent radical surgery and those who did not. The CCS and the Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM) are additional predictive factors, although their predictive value has not been validated in elderly patients;3132 in our study, there was no significant difference in these scores between the elderly and non-elderly patients.
Many studies that evaluated safety, feasibility, and outcomes in elderly patients with periampullary cancer have been conducted, but most of these studies defined elderly patients as septuagenarians;7333435 there are only a few reports on octogenarians, and these showed major postoperative complication rates from 32.2 to 50.0%.103637 In our study, the major complication rate was 20.0%, and the lower rate in our study was likely because we included recent operations; our rate was similar to the rate in another recent report of complication rates.38 In addition, with the exception of the patients with duodenal cancer, the TNM stages of periampullary adenocarcinoma in our study were below stage III. Our results suggest that the patients in our study who underwent surgery were surgically and oncologically appropriate for the treatment they received.
Although we could not directly know the TNM stages of the patients in the non-surgery group, there were no significant differences in tumor markers or tumor differentiation between the surgery and non-surgery groups; we therefore inferred indirectly that there were likely not significant differences in TNM stages between the two groups. In addition, we performed a subgroup analysis to compensate for the heterogeneity of the study group, and that analysis showed that patients with distal CBD cancer who underwent surgery had better OS than did those who did not, although there were no differences in baseline characteristics between the two groups except for CCS, which was higher in the surgery subgroup than in the non-surgery group.
The main focus of the previous articles on octogenarians was not oncologic outcomes but rather surgical safety and feasibility,83739 whereas we evaluated not only surgical safety and feasibility but also surgical oncologic outcomes; moreover, the control group in our study consisted of elderly patients who did not undergo surgery. Most of the previous studies compared elderly patients with younger patients to evaluate the oncologic outcomes, 7834353739 whereas comparison between two elderly groups in our study excluded potential confounding factors related to aging and showed the effectiveness of radical surgery for elderly patients with periampullary cancer. What we found was that the octogenarian patients with periampullary cancer who were operable and did not have physiologic conditions that precluded radical surgery had good oncologic outcomes without serious complications.
Our study has major limitations due to its retrospective design and its heterogeneous study group, which was affected by various diseases; although the subgroup analysis accounted for the heterogeneity of the study group, we were only able to statistically analyze the subgroup with distal CBD cancer because of the small sample size. Moreover, in elderly patients, quality of life is as important as life expectancy, and because of the retrospective study design, we could not include parameters that estimated the elderly patients' quality of life.
Nevertheless, our study provides significant results concerning radical surgery for elderly patients with periampullary cancer. Specifically, radical surgery for certain octogenarian patients with periampullary cancer is safe and feasible and can be expected to result in better survival outcomes, especially for patients with CBD cancer. Further study is warranted to develop a more sophisticated system for selecting elderly patients to obtain better outcomes.


 XML Download
XML Download