

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Total splenectomy (TS) is associated with severe peri-and post-operative complications such as infections, intra-abdominal abscess, portal vein thrombosis, pulmonary hypertension, thrombocytosis and venous thromboembolism.123456 It is widely acknowledged that individuals with anatomical or functional asplenia are at high risk of developing severe and potentially fatal infections caused by encapsulated bacteria (OPSI).7 Phagocytic activity of splenic macrophages and synthesis of anti-polysaccharide antibodies by splenic B-lymphocytes play important roles in providing defense against infections.7 The reported prevalence of OPSI after TS is around 4%, and the overall mortality is 2%.7
Some studies have shown that the preservation of 25–30% of splenic parenchyma is adequate to ensure a satisfactory immunological response to an antigenic stimulus.789 In addition, it has been hypothesized that additional knowledge about the surgical anatomy will facilitate the surgeons in performing partial resection of the spleen.10 The advantage of partial splenectomy (PS) is the removal of the lesion and at the same time, preservation of the splenic function. Christo11 first reported partial regulated splenectomy, then, Morgensten and Shapiro12 formally described PS in 1980, and finally, laparoscopic PS was performed by Poulin in 1995.13 Consequently, the indications of PS were extended to cystic diseases, hydatid cyst, benign splenic tumors, hematological disease, and splenic trauma.141516171819 Laparoscopic,20 single-port21 and robotic PS1822 are reported in selected patients, despite this, there exist only limited researches about the mini-invasive and open surgical approach.23
In the present study, we report our experience over the last four years with PS. Additionally, we performed a systematic review of the literature with an aim of assessing the number, the perioperative characteristics and postoperative complications related to the surgical approach of PS.
Go to : 
MATERIALS AND METHODS
Case series
Patients
From January 2014 to August 2017, five PS were performed in our department. Three of the five (60%) PS cases were conducted with an open approach and two (40%) laparoscopically. Preoperative workup included abdominal computed tomography (CT) scan with 3-dimension vascular reconstruction for all patients. Indications for resection of benign splenic masses were apparent by the presence of symptoms or a tumor greater than 5 cm located on the upper or lower pole of the spleen. Hydatid serology was performed in patients with suspected hydatid disease. All patients received prophylactic Pneumococcus, Meningococcus and Haemophilus immunization before surgery. After discharge, all the patients were followed up using a classic screening protocol including imaging studies (ultrasound or abdominal CT) and routine biological tests every 6 months during the first 12 months, and then every 12 months during the following years.
The demographic parameters, clinical manifestation, preoperative evaluation, intraoperative details, tumor data and postoperative complications were collected for analysis. All patients have been contacted by telephone until end of study date.
Surgical procedure
All operations were performed by the same surgeon (FC).
- Open approach: The abdominal cavity was opened by a xiphoid-pubic incision. Dissecting the gastro colic ligament leads to the retrocavity of the epiplon through the translucent area of Bouchet.24 The short gastric vessels were ligated using an ultrasonically activated scalpel (Harmonic scalpel, Ethicon Endo-Surgery, Inc. Cornelia, GA) or a vessel sealant (LigaSure; Medtronic, Covidien products, Minneapolis, MN). The artery and the splenic vein were identified and clamped, the spleen was then mobilized through Jinnai's manoeuver. Identification and section of the upper or lower polar splenic vessels were performed. During unclamping the artery and splenic vein, a demarcation line was identified. The preservation of the vascularization of the remaining pole was verified by intraoperative Doppler ultrasound. Subsequently, the sectioning of the parenchyma 1 cm away from the demarcation line was performed using the chosen surgical device. The bleeding was controlled with bipolar device (Erbe Elektromedizin, Germany) and a hemostatic sponge (TachoSil®-Nycomed, Konstanz, Germany) or a fibrin sealant (Tissel® Baxter, Vienna, Austria). The remaining spleen was inserted into a mesh of re-absorbable material and attached to the diaphragm. An abdominal drainage was placed next to the spleen remnant.
- Laparoscopic approach: The patient was placed in semi-lateral right decubitus after general anesthesia. Laparoscopy was performed using the open technique, under CO2 pneumoperitoneum with 12 mm Hg insufflation pressure. First, a 12-mm periumbilical optical port was positioned by the Hasson technique. Subsequently, the other 3 ports (one 12-mm and two 5-mm ports) were visualized directly and placed along the costal margin at a distance depending on the spleen size. The lesion, if cystic, was punctured with the needle, and the fluid was aspirated. The splenocolic ligament was dissected to expose the lower pole of the spleen, and the gastrosplenic ligament was dissected to expose the splenic hilum. An ultrasonically activated scalpel (Harmonic scalpel, Ethicon Endo-Surgery, Inc., Cornelia, GA) was used to mobilize the spleen after sectioning the short gastric vessels. The upper or lower polar branches of the splenic vessels were identified, dissected and cut by laparoscopic linear stapler (EndoGia®) with a 45 mm white cartridge. As a result, a demarcation line was defined. Ultrasonic shears were used to transect the splenic parenchyma at 1 cm from the demarcation line. Small bleeds were controlled by bipolar device (Erbe Elektromedizin, Germany) and a hemostatic sponge (TachoSil®- Nycomed, Konstanz, Germany) or fibrin sealant (Tissel® Baxter, Vienna, Austria). The spleen remnant was not routinely fixed or sutured. The specimen was put into a retrieval bag and removed from the incision of the 12 mm port. Finally, the surgical site was carefully checked and an abdominal drainage was placed next to the spleen remnant.
A systematic review of the literature
The methodological approach included the development of the selection criteria, the definition of the search strategy, an assessment of the study quality and abstraction of the relevant data. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement checklist for reporting a systematic review was applied.25
Study inclusion criteria
The study selection criteria were defined before starting the data collection to consent correct identification of the studies eligible for the analysis. All studies reporting PS were retrieved and checked for eligibility. The selection criteria included the following:
- Types of study: epidemiological studies, interventional trials, case-control studies, cross-sectional studies and case series including more than two patients were considered eligible for inclusion in this systematic review. Case reports, review articles, systematic reviews, meta-analyses, conference abstracts, letters and commentaries were not considered.
- Types of participants: adult or adolescent patients (aged over 13 years) undergoing open, mini-invasive PS due to splenic mass or cyst were considered.
Literature search strategy
A literature search was performed on the following online databases: MEDLINE (through PubMed), EMBASE, Google Scholar, Scopus, Cochrane Oral Health Group Specialized Register and ProQuest Dissertations and Thesis Database. To increase the probability of identifying all the relevant articles, a specific research equation was formulated for each database, using the following keywords and/or MeSH terms: partial splenectomy, laparoscopic partial splenectomy, hemisplenectomy, subtotal splenectomy, partial spleen resection and hemi-splenectomy.
In addition, the reference lists from the eligible studies and relevant review articles (not included in the systematic review) were cross-checked to identify additional records. The literature search was performed in August 2017 and was restricted to articles published since January 1997. Only studies written in English and meeting the selection criteria were reviewed.
Study selection and quality assessment
The titles and abstracts of the retrieved studies were independently and blindly screened for relevance by two reviewers (FE and AN). To enhance sensitivity, records were removed only if both the reviewers excluded the record at the title screening level. All disagreements were resolved based on the discussion with a third reviewer (FC). Subsequently, both the reviewers performed a full-text analysis of the selected articles. Two reviewers independently assessed the risk of bias and study quality using appropriate tools. The Grading of Recommendations Assessment Development and Evaluation (GRADE) system26 was used to enable consistent judgment of the “body of evidence” included in the systematic review. GRADE specifies four categories: high, moderate, low, and very low. In the context of a systematic review, the quality of evidence reflects the confidence that the estimates of the effect are correct and overpasses the individual study risk of bias by evaluating the following aspects: study design, imprecision, inconsistency, indirectness of study results and publication bias.
Data extraction
Data extracted from the studies included in the systematic review were processed for qualitative and possibly quantitative analyses. Outcome measures (mean and median values, standard deviation and ranges) were extracted for each variable. Average morbidity and mortality rates were calculated.
Go to :
RESULTS
Case series
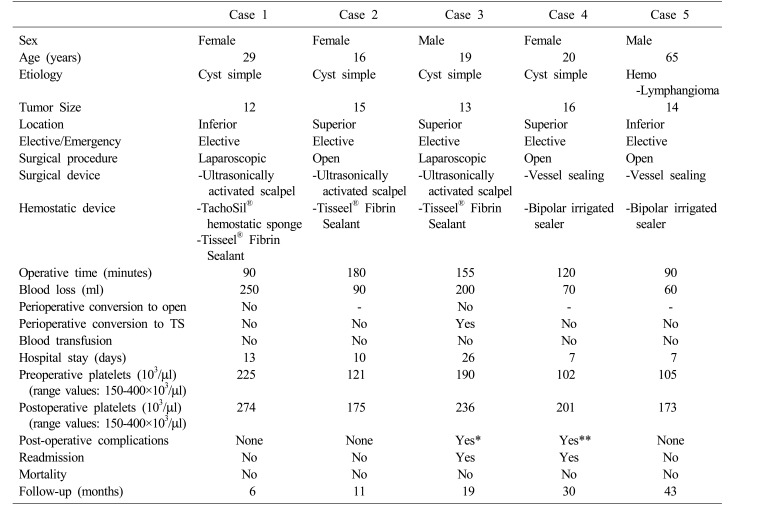
During the study period, five patients underwent elective PS (Table 1) at S.G. Moscati Hospital. In all the cases, the symptoms reported were abdominal pain and three cases (60%) were reported to be suffering from mild thrombocytopenia. There were 3 (60%) women and 2 (40%) men, and the median age of the subjects was 20 years (16–65 years). Three (60%) patients underwent open PS and, in two cases (40%), PS was performed laparoscopically. Four patients (80%) underwent PS for a simple cyst and one patient underwent PS (20%) for hemo-lymphangioma (Fig. 1). The median tumor size was 14 cm (12–16 cm) and in three (60%) cases, it was located in the upper pole of the spleen.
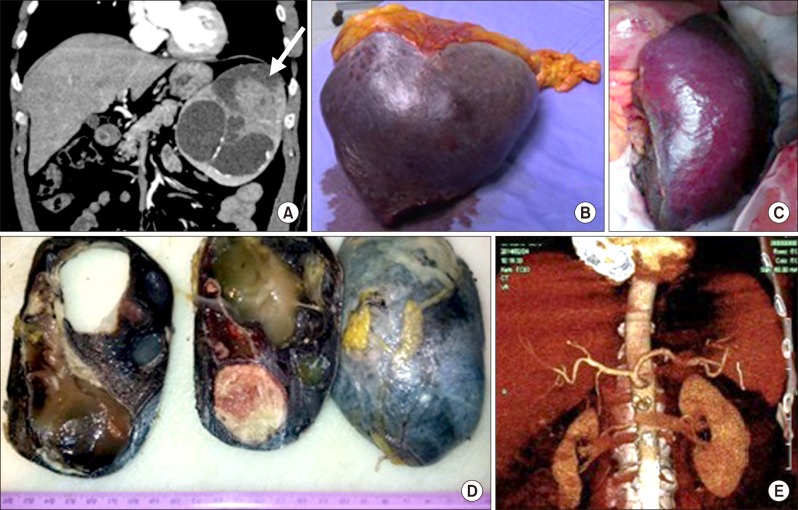 | Fig. 1Case no. 5. (A) Preoperative computed tomography: the arrow shows the splenic mass. (B) Intraoperative view of the splenic mass after removal. (C) Intraoperative view of the splenic residual parenchyma. (D) Macroscopic examination of the surgical piece. (E) 3D reconstruction of the remaining splenic parenchyma at three months after surgery.
|
Table 1
Characteristics of patients treated with PS in our department
*On the 8th postoperative day, the patient underwent laparoscopic emergency surgery for hematoma with active bleeding that required control of haemostasis and a placement of drainage. Three months later, the occurrence of infected fluid collection required a TS using an open approach after failures in placement of percutaneous drainage and the laparoscopic approach
**One month after surgery, a follow-up scan revealed a fluid collection (78×48 mm) which did not result in clinical evidence requiring the placement of radiological drainage
TS, total splenectomy; PS, partial splenectomy
![]()
During surgery, an ultrasonically activated scalpel (Harmonic scalpel, Ethicon Endo-Surgery, Inc., Cornelia, GA) was used in 3 cases (60%) and in 2 cases (40%) a vessel sealant (LigaSure; Medtronic, Covidien products, Minneapolis, MN) was used. A bipolar irrigated sealer (Aquamantys®) was used to improve hemostasis in 2 patients (40%) and in the remaining cases, a hemostatic sponge (TachoSil) or a fibrin sealant (Tisseel) was applied. The median operative time was 120 minutes (90−180 minutes), the estimated blood loss was 90 ml (60–250 ml) and in 1 case (20%) blood transfusions were required in postoperative course. No perioperative conversion to TS or change in approach was necessary.
The median hospital stay was 7 days (6–26 days). Platelet counts returned within the normal range on the fifth postoperative day and no incidence of mortality was observed. No thrombosis of the splenic and portal veins and no total splenic infarction occurred. Furthermore, in 2 (40%) cases there were postoperative complications. In 1 patient (Case 3), on the 8th postoperative day, the patient underwent laparoscopic emergency surgery for hematoma with active bleeding that required control of hemostasis and a placement of drainage. Moreover, his postoperative course was prolonged by an allergic reaction to antibiotics. Three months later, due to the collection of infected fluid, a TS was required using an open approach subsequent to failures in the placement of percutaneous drainage and the laparoscopic approach. In another patient (Case 4), one month after surgery, a follow-up scan revealed fluid collection (78×48 mm) which did not result in clinical evidence requiring the placement of radiological drainage. It was removed 7 days later and at the final follow-up (30 months), no recurrence was observed.
The median follow-up was 19 months (6−43 months). None of the patients pursued antibiotics-prophylaxis in the long term, with the exception of the case which required procedural conversion to TS. The patients appeared to be clinically well at final follow-up.
Literature review
Literature search and selection
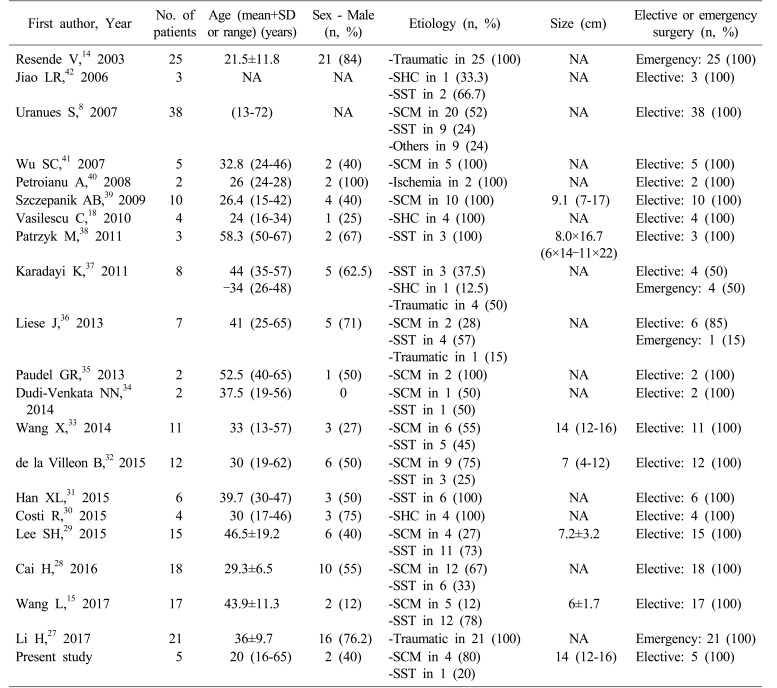
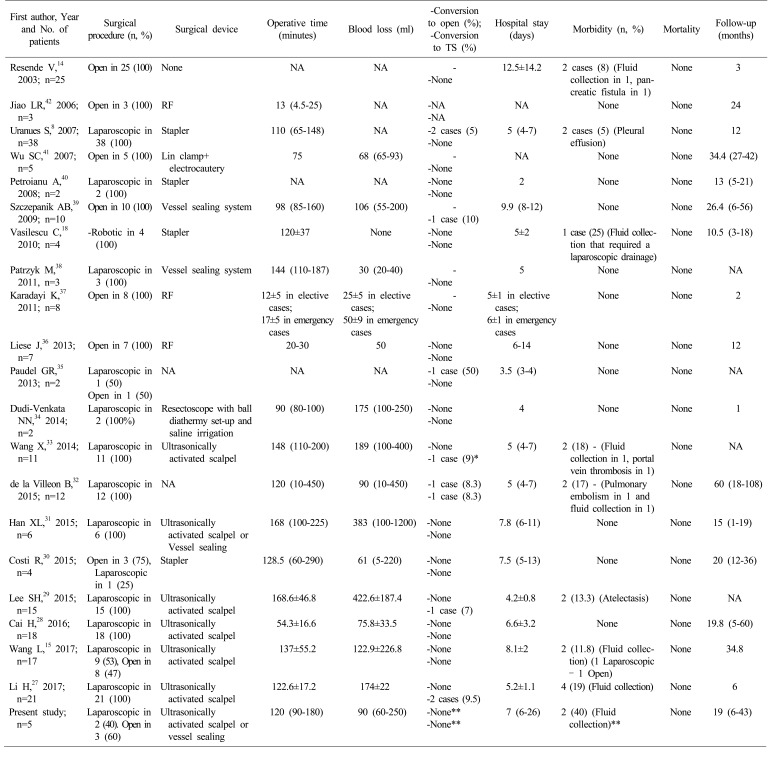
Out of the 252 articles initially identified, 20 articles814151827282930313233343536373839404142 (Tables 2, 3) met the inclusion criteria and were selected for the systematic review. The flowchart representing the identification of the studies and inclusion/exclusion process is shown in Fig. 2.
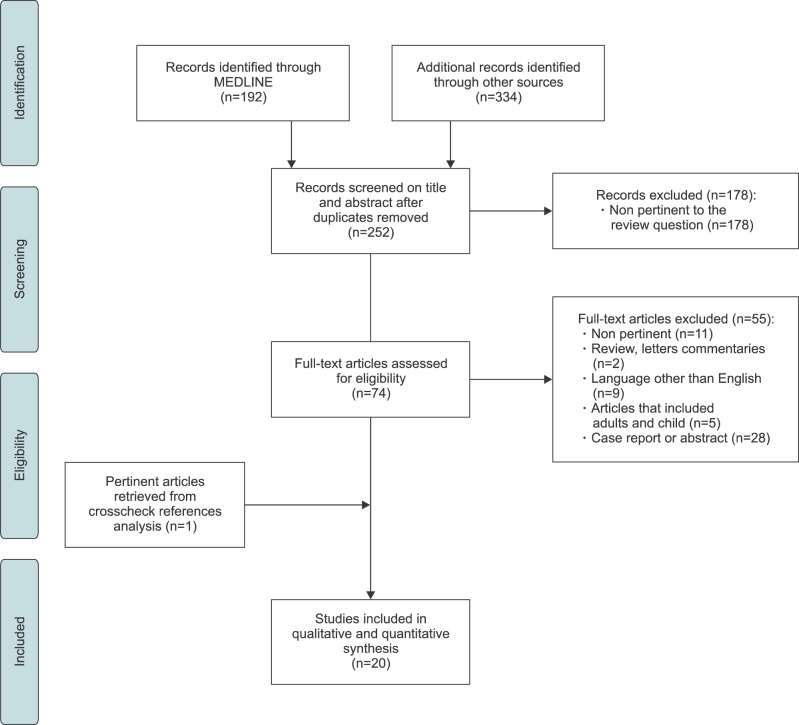 | Fig. 2Flow chart demonstrating study search, selection and inclusion criteria. Example of search equation: (Partial splenectomy [Title/Abstract]) OR (laparoscopic partial splenectomy [Title/Abstract]) OR (Hemisplenectomy [Title/Abstract]) OR (subtotal splenectomy) OR (partial spleen resection [Title/Abstract]) OR (hemi-splenectomy [Title/Abstract]) AND (Humans [Mesh]) AND (adult [MeSH]).
|
Study characteristics
The selected studies were published between 2003 and 2017 and consisted of 4 original articles14152729 and 16 case series8182830313233343536373839404142 (Table 2). They were carried out in fourteen different countries, particularly in Asia and Pacific regions (n=10),15272829313334353741 Europe (n=7)18303236383942 and North and South America (n=3).81440
Excluding our 5 cases, overall, 213 patients undergoing PS are described (Table 2). The most common indication of PS were as follows: splenic cyst in 76 cases (35.6%), splenic solid tumor (hemangioma, lymphangioma, hamartoma and metastases) in 65 cases (30.5%), traumatic in 51 cases (24%), splenic hydatic cyst in 10 cases (4.7%) and others in 11 cases (5.2%). PS was performed electively in 162 (76%) patients and as an emergency in 51 (24%) of the cases.
Laparoscopic, open and robotic approaches were used in 65.2% (139/213), 32.8% (70/213) and 2% (4/213) of patients, respectively. The rate of conversion from laparoscopic to open surgery in each series ranged from 5%8 to 50%.35 Overall, the surgical approach was converted into the open in 3% (4/139) of patients and the reasons were bleeding and adherence. A case which required conversion was the formation of pneumothorax due to inflammatory adhesions between the spleen and the diaphragm.32
In 3% (6/213) of cases (range, 7%–10%), PS was converted intraoperatively in TS and the causes included insufficient blood supply,39 intraoperative splenic injury,33 hemodynamic instability of patients27 and risk of malignancy.32
The overall morbidity rate was 8% (17/213) with a range in the studies that went from 5%8 to 25%.18 The most common complications were: fluid collection in 58.8% (10/17)1415182733 of cases, atelectasis and pleural effusion in 23.6% (4/17),829 pulmonary embolism in 5.8% (1/17),32 pancreatic fistula in 5.8% (1/17)14 and portal vein thrombosis in 5.8% (1/17)33 of patients.
With regard to the fluid collection, 20% (2/10) of cases required the placement of a radiological drainage, in 10% (1/10) laparoscopic drainage was necessary, while in the remaining cases medical therapy was adequate. No mortality was reported.
Regarding the morbidity rate related to the surgical approach, postoperative complications occurred in 4.3% (3/70) of patients undergoing open PS versus 9.8% (14/143) of patients undergoing minimally invasive (laparoscopic and robotic) PS. However, the only study15 included in this review that compared laparoscopic PS and laparotomy PS did not show any difference between the two groups in terms of postoperative complications (p=1.000).
With respect to the overall rate of conversion to TS, 3.5% (5/143) of patients among those operated laparoscopically finally received a TS versus 1.4% (1/70) of patients operated by laparotomy. There exists no study detailing the aforementioned comparative aspects. Perioperative and postoperative data of studies are summarized in Table 3.
Study quality assessment
Two reviewers (FE and AN) scored the methodological qualities of the included studies according to the criteria described above. No randomized controlled trial was found. The studies were case series or original articles with different methods and aims. Based on the GRADE system,43 4 studies14152729 (20%) were judged as being of low quality and the remaining 16 studies8182830313233343536373839404142 (80%) of very low quality of evidence. Of note, all the studies were retrospective, which, by definition, are susceptible to major selection bias, as well as misclassification, detection, or information bias due to the indefinite accuracy in record keeping.
Go to :
DISCUSSION
The aim of this study was to provide a comprehensive overview of splenic partial resections and the occurrence of postoperative complications in relation to the surgical approach. In our recent experience, two laparoscopic and three laparotomies PS were carried out. There was no perioperative need to perform TS or to modify the surgical approach. Nevertheless, in a patient undergoing laparoscopic PS, there were several postoperative complications requiring globally two other surgical procedures, blood transfusion, readmission, and finally TS by laparotomy. All patients were followed over time and no further complications were observed.
In addition, this systematic review involving 20 articles and 213 patients showed that mini-invasive PS is a reliable procedure but burdened by a conversion to laparotomy rate of 3% (range, 5–50%), a conversion to TS rate of 3.5% and a morbidity rate of 9.8% compared with 1.4% and 4.3% in the open approach, respectively. Only a single comparative study15 found that laparoscopic PS required a longer operative time but a lower hospital stay compared to laparotomic PS. No statistical differences were observed in other parameters, such as blood loss, time of drainage removal and incidence of complications. It should also be noted that the incidence of incisional hernia after laparoscopy was lower than that of laparotomy20 and moreover, the surgeon's level of experience with laparoscopic surgery cannot be ignored.
New mini-invasive techniques have been described, in particular, single-port and robotic surgery. Single-port laparoscopic PS was used for the first time by Hong et al.21 in 2010 and was completed using a homemade single- port,4445 ultrasonic scissors and an articulating dissector for a benign cyst located in the upper pole of the spleen. In one case, the postoperative course was uneventful, and no recurrence or complication was highlighted for six months of follow-up.
Some authors have published their experience with the robot-assisted PS.18224647 The robot-assisted approach might be the most indicated for PS because it allows for a perfect dissection due to the high definition imaging quality, as well as, tremor reduction, stereoscopic vision and greater maneuverability. Vasilescu et al.46 compared laparoscopic PS with robotic PS and reported the statistically significant difference in terms of blood loss (35 vs. 90 ml) and duration of vascular dissection (20 vs. 15 min). The outcomes were in favor of robotic PS. Additionally, the operative time was not significantly different between the two surgical approaches. As reported by Giulianotti et al.22 the robotic technology with 3D vision and ‘wrist-like’ instruments provides better hilar dissection, more accurate vascular isolation and good vascular control. Conversely, the disadvantage of robotic surgery is the high cost involved in the treatment.
The greatest risk during PS is uncontrolled bleeding, which could be reduced by using innovative tools and new techniques. Important technical contributions were provided by new instruments, especially in the parenchyma section. The use of an ultrasonically activated scalpel, vessel sealant, staplers and radiofrequency ablative device were described but no superiority over the other has been demonstrated.484950 A bipolar irrigated sealer, hemostatic sponges, matrix hemostatic agents or fibrin sealants were used to reduce bleeding from residual parenchyma but no specific studies demonstrated better efficacy.51
In selected cases, an alternative to reduce intraoperative bleeding could be preventive arterial embolization.3852 In fact, the splenic artery is divided into a superior artery and a lower polar artery in 86% of cases, and finally, they subdivide into multiple segmental branches.10 A month before surgery, the embolization of these segmental branches at the splenic hilum level leads to focal ischemia of the corresponding splenic parenchyma. Typical indications for a pre-surgical partial splenic embolization include hematological disorders like chronic thrombocytopenic purpura and other thrombocytopenias, osteomyelosclerosis, thalassemias, hereditary spherocytosis, splenic hemangiomas and splenic trauma.3853 On the contrary, embolization in itself is not complication-free, and there exists the potential for abscess formation, spontaneous splenic rupture, along with common post-embolization syndrome of fever, pain and vomiting.5354
As suggested by de la Villeon et al.,32 regardless of the instrument employed or the preoperative procedure, the technical key point to minimize blood loss is placing the parenchymal transection line inside the ischemia demarcation limit. As the ischemia limit is not a clear-cut plane, parenchymal transection crossing this plane may cause bleeding from adjacent segments. It is suggested that cutting the spleen 1 cm inside the ischemic demarcation line could avoid such problems.
Regarding PS in an emergency, the most recent guidelines strongly recommend this procedure for pediatric patients; whereas this issue is still being widely debated in adults.55 Numerous reports have demonstrated that the laparoscopic approach and PS are feasible and safe in hemodynamically stable patients.142756 As reported by Li et al.,27 a laparoscopic PS was performed in patients with: (i) Preoperative CT scan revealing single pole rupture without spleen pedicle injury; (ii) Blood pressure >90/60 mm Hg and heart rate <120 beat per minute; and (iii) No sign of multiple organ injuries. Both laparoscopic TS and laparoscopic PS had a similar intraoperative blood loss and operative time. Two patients (2/21, 9.5%) became hemodynamically unstable during spleen mobilization and conversion to laparoscopic TS was successfully completed. No statistically significant difference in postoperative complications was found in the two groups. However, prospective trials with clear inclusion criteria are needed to demonstrate the benefit of laparoscopic PS in emergency surgery.
In conclusion, in selected cases, PS should be preferred for all patients, especially in the younger ones. The mini-invasive approach seemed to be feasible despite the presence of higher rate of complications than the open technique. In future, further studies on this topic are needed by involving more patients. Furthermore, it is proposed that the development of robotic surgery could make this approach the new gold-standard technique for spleen-preserving surgery.
Go to :
 XML Download
XML Download