

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Although the prevalence of gastroesophageal reflux disease (GERD) is relatively low in Korea, it is rapidly increasing. GERD has recently been recognized as a significant health concern in Korea, and the use of proton pump inhibitor (PPI) is consequently on the rise [1].
However, antireflux surgery has not been widely adopted as a treatment for GERD in Korea, and few Korean studies have reported the use of this operation. Therefore, the surgical options for GERD are not well known, even among surgeons [23].
Since laparoscopic Nissen fundoplication (LNF) for GERD was first advocated [4], laparoscopic total fundoplication has been regarded as an alternative treatment modality for GERD. Several randomized studies have found that its effect is similar to those of long-term treatment with a PPI, improving the symptoms in 85%–90% of patients [56].
LNF with a total wrap that completely surrounds the esophagus is the most commonly used gold standard technique worldwide for antireflux surgery [7]. However, it is associated with a high incidence of postoperative dysphagia and gas-bloat syndrome [89]. Therefore, partial fundoplications including the Toupet (posterior 270°) and Dor (anterior 180°) methods were introduced to avoid these adverse outcomes [101112].
Recently, the Korean Anti-Reflux Surgery (KARS) study group performed a nationwide survey of antireflux surgery in Korea. Furthermore, they announced their plans to investigate partial fundoplication to fore-gut surgeons. Here, we evaluate the short-term surgical outcomes and postoperative adverse outcomes of partial fundoplication in Korea and compared the data with corresponding data for total LNF.
Go to : 
METHODS
The nationwide survey of KARS study group identified 32 cases of partial fundoplication from 8 hospitals including Incheon St. Mary's Hospital (16 cases), Ajou University Medical Center (4 cases), Chung-Ang University Hospital (3 cases), St. Vincent's Hospital (2 cases), Kosin University Gospel Hospital (2 cases), Chosun University Hospital (2 cases), Uijeonbu St. Mary's Hospital (1 case), and Korea University Ansan Hospital (2 case). All operations were performed between September 2009 and January 2016. Approval to perform research on human subjects in this survey was provided by the Institutional Review Board of each Hospital.
Survey data included patient characteristics, duration of typical and atypical symptoms, responses to PPIs, preoperative endoscopic findings, and presence of hiatal hernia. Among operative findings, the reason for partial fundoplication or combination with other procedure was assessed. Among postoperative findings, short-term surgical outcomes including the operation time, time to start liquid diet, time to start soft diet, hospital stay, and the morbidity at the time of discharge and 3-month postoperative follow-up data were recorded.
GERD symptoms were categorized as typical and atypical. The former included heartburn, regurgitation, and epigastric pain, while the latter included cough, globus sensation, and throat pain. Postoperative symptom resolution was graded as poor, fair, good, or excellent. “Poor” indicated treatment failure, while “fair” implied partial symptom control. “Good” and “excellent” indicated complete symptom control. Postoperative adverse outcomes such as dysphagia, difficult belching, gas bloating, and flatulence were graded with 5-point scores (no symptom, 0; mild, 1; moderate, 2; severe, 3; very severe, 4).
Partial fundoplication data were compared with previous data collected by KARS regarding 86 total fundoplications. Short-term outcomes and symptom resolution (at the time of discharge and at 3 months postoperatively) were compared between the groups using chi-square and Student t-test. In addition, postoperative adverse outcome scores were compared between the 2 groups.
IBM SPSS ver. 18.0 (IBM Co., Armonk, NY, USA) were used for statistical analysis. For all data analyses, P < 0.05 was considered statistically significant.
Go to :
RESULTS
Patient characteristics of partial fundoplication cases
A total of 32 patients underwent partial fundoplication between September 2009 and January 2016 (Table 1). The mean age was 56.3 ± 16.5 years (range, 19–88 years), and the ratio of male to female was 0.8:1. The mean body mass index was 23.9 ± 3.9 kg/m2 (range, 17.4–33.8 kg/m2).
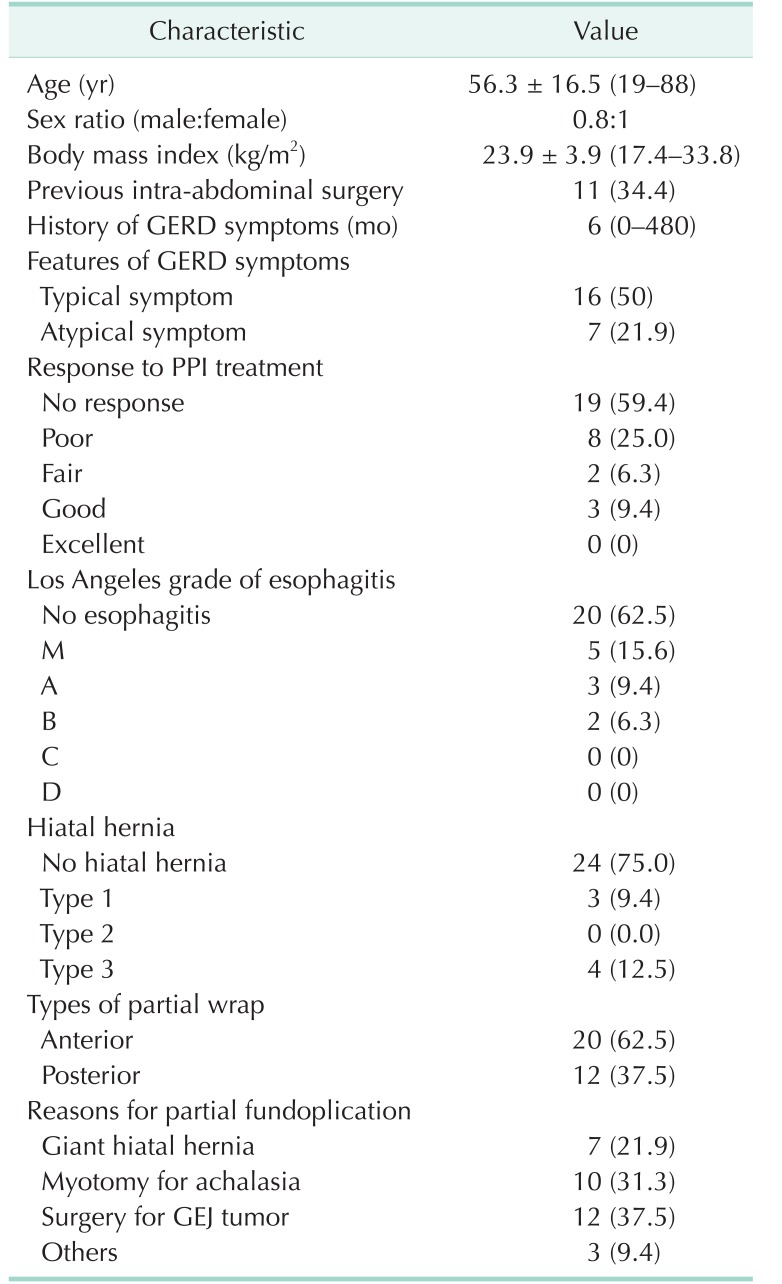
Of these patients, 11 (34.4%) had undergone other intra-abdominal surgeries before partial fundoplication.
The median duration of GERD symptoms was 6 months (range, 0–480 months). One half of GERD symptoms were typical, and 19 of 32 patients (59.4%) did not respond to PPIs. More than half of patients (62.5%) did not have esophagitis based on the Los Angeles grade of esophagitis. In addition, most patients (75%) did not have an associated hiatal hernia.
The anterior (Dor) procedure was used in 20 cases (62.5%) and the posterior (Toupet) procedure was used in 12 cases (37.5%). They were almost secondary procedures after operations for other conditions, such as gastroesophageal junction tumor (12 cases, 37.5%), achalasia (10 cases, 31.3%), and giant hiatal hernia (7 cases, 21.9%).
Total versus partial fundoplication: short-term outcomes
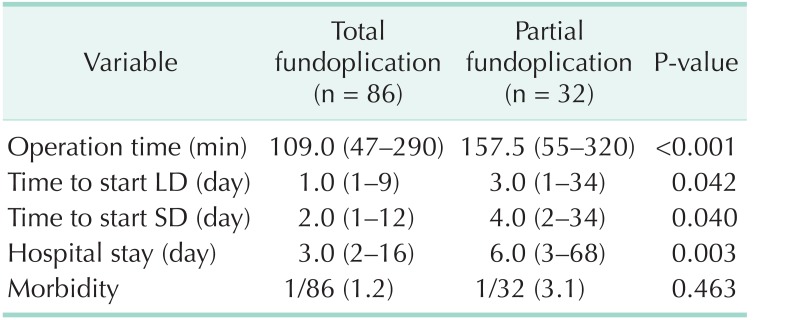
In terms of short-term outcomes (Table 2), partial fundoplication showed longer operation time and hospital stay than total fundoplication (median operation time, 157.5 and 109.0 minutes, respectively, P < 0.001; median hospital stay, 6.0 and 3.0 days, respectively, P = 0.003.). In addition, partial fundoplication was also associated with a significant delay in diet initiation compared to total fundoplication (median time to start liquid diet, 3.0 and 1.0 days, respectively, P = 0.042; median time to start soft diet, 4.0 and 2.0 days, respectively, P = 0.040.). However, no significant difference was found between the 2 procedures in terms of morbidity (3.1 and 1.2 %, respectively, P = 0.463).
Total versus partial fundoplication: symptom resolutions
The symptom resolution rates were showed in Table 3. The postoperative typical symptom resolution rate at the time of discharge was excellent (68.8%), good (25.0%), and fair (6.3%) in 16 patients who initially had typical symptoms. Therefore, the total symptom resolution rate was 93.8% (15 of 16) in partial fundoplication cases. However, the typical symptom resolution rate decreased to 81.3% (13 of 16) after 3 months.
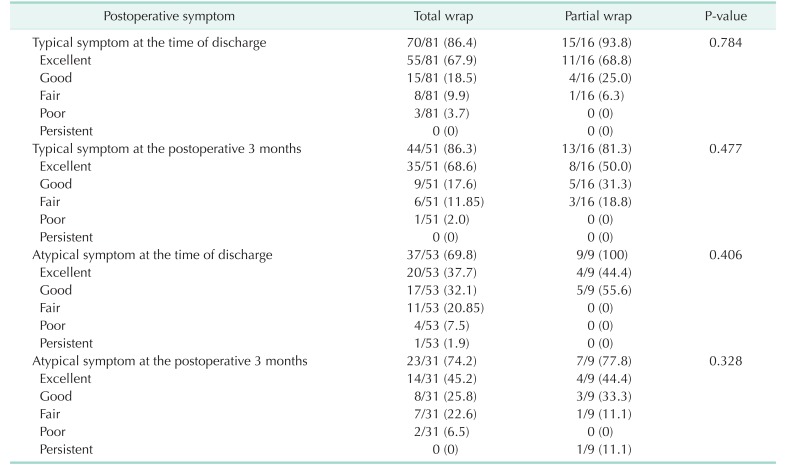
Table 3
Incidence of postoperative symptom resolution
The cases that initially showed no symptom was excluded from this comparison. Therefore, these values are expressed as the number of patients undergoing symptom resolution divided by the number of initially symptomatic patients. In this comparative analysis, ‘excellent’ or ‘good’ resolution was regarded as postoperative symptom resolution.
![]()
Nine patients (29.1% of partial fundoplication cases) had atypical symptoms at the time of initial diagnosis. All of these patients (100%) showed atypical symptom resolution at the time of discharge. Two of them showed atypical symptoms after 3 months. Therefore, the atypical symptom resolution rate decreased to 77.8% (7 of 9).
No significant difference was found between total and partial fundoplication in terms of the resolution rate of typical symptoms, either at the time of discharge or 3 months after the operation (P = 0.784 and P = 0.477, respectively). The resolution rate of atypical symptoms also did not differ between total and partial fundoplication cases at the time of discharge or 3 months postoperatively (P = 0.406 and P = 0.328, respectively).
Total versus partial fundoplication: postoperative adverse symptoms
In terms of postoperative adverse symptoms, total fundoplication was associated with higher rates of all 4 adverse symptoms at the time of discharge than partial fundoplication (dysphagia, 48.8% and 18.8%, respectively, P = 0.040; difficult belching, 47.7% and 12.5%, respectively, P = 0.006; gas bloating, 44.2% and 6.3%, respectively, P = 0.005; and flatulence, 31.4% and 9.4%, respectively, P = 0.087) (Fig. 1).
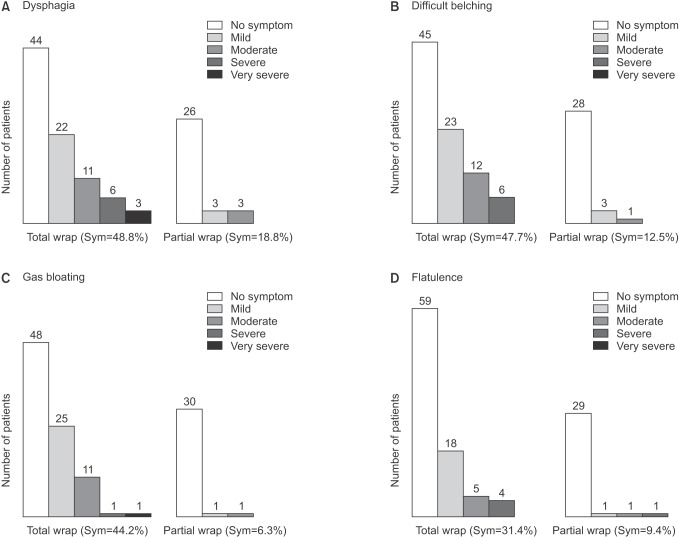 | Fig. 1Comparison of postoperative adverse symptoms at the time of discharge. (A) Dysphagia was more frequent after total fundoplication than partial (Incidence was 48.8% and 18.8%, respectively, P = 0.040). (B) Difficult belching was more frequent after total fundoplication than partial (Incidence was 47.7% and 12.5%, respectively, P = 0.006). (C) Gas bloating was more frequent after total fundoplication than partial (Incidence was 44.2% and 6.3%, respectively, P = 0.005). (D) Flatulence was more frequent after total fundoplication than partial (Incidence was 31.4% and 9.4%, respectively, P = 0.087). Sym, incidence of symptoms.
|
After 3 months, adverse outcome rates did not improve, and between-group differences showed similar trends (dysphagia, 42.6% and 3.1%, respectively, P = 0.004; difficult belching, 31.5% and 3.1%, respectively, P = 0.020; gas bloating, 48.1% and 12.5%, respectively, P = 0.009; and flatulence, 46.3% and 12.5%, respectively, P = 0.020) (Fig. 2).
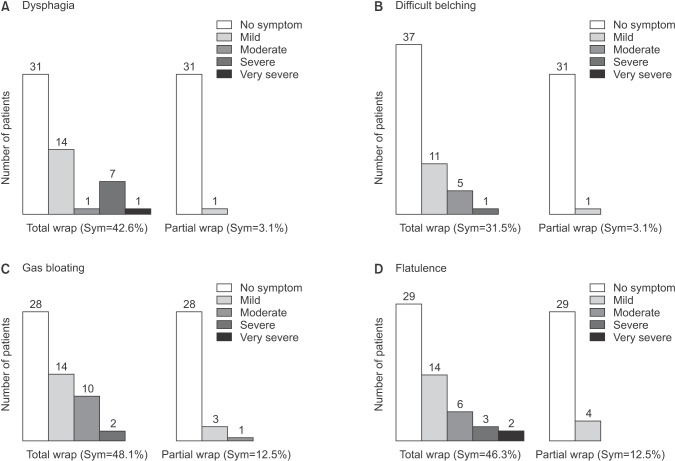 | Fig. 2Comparison of postoperative adverse symptoms at the postoperative 3 months. (A) Dysphagia was more frequent after total fundoplication than partial (Incidence was 42.6% and 3.1%, respectively, P = 0.004). (B) Difficult belching was more frequent after total fundoplication than partial (Incidence was 31.5% and 3.1%, respectively, P = 0.020). (C) Gas bloating was more frequent after total fundoplication than partial (Incidence was 48.1% and 12.5%, respectively, P = 0.009). (D) Flatulence was more frequent after total fundoplication than partial (Incidence was 46.3% and 12.5%, respectively, P = 0.020). Sym, incidence of symptoms.
|
Go to :
DISCUSSION
Recently, as the use of upper gastrointestinal endoscopic examination has increased rapidly in Korea, the detection of benign pathologic conditions related to the gastroesophageal junction has consequently increased. Furthermore, minimally invasive approaches such as laparoscopic wedge resection have become the standard approach for benign gastroesophageal junctional tumors, and functional problems including gastroesophageal reflux due to destruction of anatomical reflux barriers in junctional areas are now a matter of concern [13].
Esophageal achalasia, an esophageal motility disorder involving the smooth muscle layer of the esophagus and the lower esophageal sphincter (LES) [14], should be treated surgically with laparoscopic Heller's myotomy in patients for whom medical management or endoscopic pneumatic dilatation is ineffective [1516]. Myotomy involves a lengthwise cut along the esophagus, starting above the LES and extending down slightly into the stomach. After this procedure, a partial fundoplication or “wrap” is generally added to prevent excessive reflux, which can cause serious damage to the esophagus over time. The most commonly recommended fundoplication with Heller's myotomy is Dor's fundoplication, which consists of a 180° to 200° anterior wrap around the esophagus. It provides substantially better results than Nissen fundoplication, which is associated with a higher incidence of dysphagia [17].
Giant hiatal hernia is a type III combined sliding and paraesophageal hernia that is accompanied by dysphagia, regurgitation, epigastric pain, and intermittent mucosal bleeding [18]. Surgical treatment is recommend for paraesophageal hiatal hernia that manifests with significant obstructive and reflux symptoms [1920]. This treatment involves 3 basic principles. The first is complete reduction of the hiatal hernia with sac excision and tension free crural repair, the second is appropriate use of esophageal lengthening procedures, and the third is an antireflux procedure for GERD management [1821]. Most recent reports of paraesophageal hiatal hernia repair describe fundoplication as a step in the repair process, and this procedure is thought to aid in preventing postoperative gastroesophageal reflux and recurrence [2223]. There is no consensus regarding the type and degree of fundoplication needed after hiatal hernia repair to prevent reflux. However, one Korean study suggests partial fundoplication as a suitable substitute for total fundoplication, especially when esophageal motility is not mandatory [24].
In the present nationwide survey, we found that partial fundoplication was additionally performed when other pathologic conditions related to the gastroesophageal junctional area were present, such as gastroesophageal junctional tumor (12 cases), achalasia (10 cases), and giant hiatal hernia (7 cases). Simultaneous operations performed in these 29 cases might be why partial fundoplication had a longer operation time than total fundoplication in our results. Therefore, one limitation of the present survey is that the actual operation times of partial fundoplication could not be acquired.
Various types of partial fundoplication have been attempted thus far, but the 2 types typically used are anterior (Dor) and posterior (Toupet) partial fundoplication. The type of fundoplication generally depends on the surgeon's preference or the primary operation. For example, Dor fundoplication is preferred after myotomy or excision of gastroesophageal junction tumors, but Nissen or Toupet fundoplication is usually adopted after giant paraesophageal hiatal hernia repair. Actually, Dor fundoplication is appropriate procedure for protecting the myotomy operation field or preventing postoperative GERD after tumor excision; its antireflux effect has not yet been widely accepted. On the other hand, Toupet fundoplication is not inferior to Nissen procedure in terms of anti-reflux effect. In our survey, anterior Dor fundoplication was the most commonly performed procedure (19 patients; 61.3%), and it was mostly performed after myotomy for achalasia (8 cases) or resection of gastroesophageal junction tumors (11 cases).
Diet after foregut surgery usually depends on the aggressiveness and invasiveness of the operative procedure and the presence of organ resection and anastomosis. The original antireflux surgical procedure has no invasive component, and a regular diet can be started 1 or 2 days after the operation. However, since cases of partial fundoplication in the present study were associated with other surgical procedures, the start of a liquid or soft diet was delayed and the hospital stay was extended.
More than half of patients in the present study had no preoperative reflux symptoms because the other conditions they had, including gastroesophageal junction tumors and achalasia, were not associated with any anatomical pathologic abnormality of the LES that could give rise to gastroesophageal reflux symptoms. Generally, patients with giant hiatal hernia had reflux or obstructive symptoms and showed excellent and good postoperative symptom resolution after hernia repair and partial fundoplication in our survey. In a previous KARS survey of total fundoplication cases, the complete typical symptom resolution rate was about 86.3% [25]. Among cases of partial fundoplication in the present study, about 90% of patients with reflux symptoms showed complete resolution postoperatively.
The most remarkable findings in this study were the disappearance of adverse symptoms after partial fundoplication for antireflux procedures. A tight gastric wrap in total fundoplication can induce typical adverse symptoms, including dysphasia, difficult belching, gas bloating, and flatulence. A partial anterior or posterior wrap may reduce tightness along the entire circumference of the gastric fold around the gastroesophageal junction. In patients who underwent total fundoplication, the incidence rates of postoperative adverse outcomes, including mild, moderate, severe, and very severe cases, were 30%–50% in the early postoperative period (Fig. 1). The present survey found that they were below 20% after partial fundoplication.
Several randomized controlled trials have compared symptom resolution and postoperative adverse outcomes between total and partial fundoplication for GERD [2627282930]. In most reports, the operative time, perioperative complications, postoperative satisfaction, recurrence, and rates of medication or reoperation due to recurrence did not significantly differ between the 2 methods, although many surgeons are concerned that partial fundoplication does not result in a life-long standing solid wrap. However, the rates of adverse results, including dysphagia, gas-bloat syndrome, inability to belch, and reoperation due to severe dysphasia, were significantly higher after laparoscopic total fundoplication than partial fundoplication. Therefore, laparoscopic partial fundoplication may be a better surgical approach for GERD because it has a lower rate of postoperative adverse results and equal efficacy compared to laparoscopic total fundoplication.
Go to :
 XML Download
XML Download