

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Early-stage (International Federation of Gynecology and Obstetrics [FIGO] stage IA–IIA) cervical cancer can be effectively treated either with primary radical surgery or pelvic radiation with 5-year survival rates of 80%–85% for stage IB and 50%–65% for stage IIA [1]. Although the survival outcomes appear comparable between the 2 modalities, surgery has an advantage of preservation of ovarian and vaginal function, which is especially important for young, reproductive age patients [12]. When surgical treatment is chosen, radical hysterectomy with pelvic lymphadenectomy is universally performed. However, the procedure is frequently associated with long-term adversities. Bladder dysfunction is one of the most common long-term complications after radical hysterectomy with incidence of 8%–80% [3]. The condition results mainly from disruption of pelvic autonomic nerves that course through posterior, lateral, and anterior paracervical/parametrial areas during radical resection of those areas, which is the important part of the procedure. For the first few days after radical hysterectomy, vesical function is diminished in all patients. In many patients, bladder dysfunction can persist for 6–12 months or even longer [34]. This has tremendous adverse impact on long-time quality of life.
Modification of the conventional technique of radical hysterectomy was first introduced by Japanese gynecologic surgeons in an attempt to diminish the damage to pelvic autonomic nerves during parametrial resection [56]. Favorable outcomes on recovery of vesical function, vaginal blood flow, and anorectal function associated with nerve preservation were documented in subsequent studies [789101112]. Nerve-sparing radical hysterectomy (NSRH) has been adopted at our institution for several years in an attempt to reduce operative damage to the pelvic autonomic nervous system [1314]. However, the recovery of bladder dysfunction has varied among the cases and also among the published studies. Some clinical and operative factors may have effects on the difference in recovery of bladder function following the procedure. Published data on predicting factors for recovery of vesical function after radical hysterectomy is lacking.
The aim of this study was to examine association between clinical/surgical predicting factors and recovery of voiding function following NSRH.
MATERIALS AND METHODS
In this retrospective cohort study, women with early-stage cervical cancer (FIGO stage IA1–IIA2) regardless of histologic type, who underwent type C1 radical hysterectomy according to Querleu-Morrow classification at Faculty of Medicine, Chiang Mai University, in the period between 2006 and 2016 were included. Type C1 radical hysterectomy, as performed in our institution, involved: 1) transection of rectovaginal and rectouterine ligaments (posterior/dorsal parametrium) at the rectum; 2) transection of vesicouterine and vesicovaginal ligaments (anterior/ventral parametrium) at the bladder; 3) transection of cardinal ligament (lateral parametrium) at the medial aspect of the internal iliac artery and vein; 4) complete mobilization and lateralization of the ureter; and 5) systematic identification and preservation of inferior hypogastric plexus and its vesical branch [1314]. Exclusion criteria were: death or refused treatment before hospital discharge, recurrent cervical cancer, postoperative transfer to intensive care unit, and intraoperative urinary tract injury that needed repair.
After approval by Faculty of Medicine, Research Ethic Committee, clinical (body mass index [BMI], medical illness, medication, and previous treatment), surgical (surgeons, types of radical hysterectomy, parametrial and vaginal resection length, lymphadenectomy), and pathological (histological cell type, largest tumor diameter, that were defined from final pathological report) data of all eligible cases were extracted from the previously collected radical hysterectomy database of Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, Faculty of Medicine, Chiang Mai University. In addition, data on postoperative voiding were collected from hospital charts.
Primary outcome was association between clinical/surgical/pathological predicting factors and inability to attain adequate voiding function on postoperative day 7 (POD7) following NSRH. At our institution, transurethral catheter is retained until POD7. Adequate voiding function was defined as uninterrupted urination with less than 100 mL of residuum, at least 2 times consecutively, without the need for further catheterization. In patients with inadequate voiding function, intermittent self-catheterization was employed until adequate voiding function is achieved. At the time of initial removal of the transurethral catheter on POD7, a urine sample was taken from each patient for urinalysis. Urinary tract infection was diagnosed if 10 or more leukocytes were identified in high-power field microscopic examination without contamination by epithelial cells and the presence of bacterial colonies of over 10,000 cfu/mL in culture.
Statistical analysis was performed by using Stata® program version 12 (StataCorp LP, College Station, TX, USA). Comparison of continuous clinical/surgical variables between patients with and without adequate voiding function on POD7 was performed by using Student's t-test. The χ2 test or Fisher's exact test, as appropriate, was used for an analysis of association of all categorical variables with inability to attain adequate voiding function on POD7. To minimize the probability of obtaining a significant result simply due to chance that resulted from simultaneous testing of multiple hypotheses, the p-value of <0.01 was employed to indicate statistical significance. Logistic regression model was applied in a multivariate analysis to determine the independent predicting factors for inability to attain adequate voiding function on POD7 following NSRH. The p-value of <0.05 was considered significant.
RESULTS
Of 755 patients, 383 (50.7%) resumed adequate voiding function on POD7 while 372 (49.3%) did not. Mean voiding volume per each voiding on POD7 were 281.4 mL in patients with adequate voiding function and 163.9 mL in patients with inadequate voiding (p<0.001). Postvoid residual (PVR) urine volume per each voiding on POD7 in patients with and without adequate voiding function were 48.2 mL and 296.0 mL, respectively (p<0.001). Mean age was comparable between the 2 groups, 46.5 years in patients with adequate voiding function on POD7 and 47.3 years in those without (p=0.25). Mean parity was 2.0 in patients with adequate voiding vs. 2.1 in those with inadequate voiding function (p=0.11).
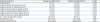
Table 1 compares operative data between patients with and those without adequate voiding function on POD7. Tumor size appeared larger in patients whose POD7 voiding function was inadequate. In addition, dimension of surgical resection represented by lengths of resected parametria and adjacent vagina were more extensive in patients with inadequate POD7 voiding function. However, number of resected pelvic lymph nodes, operative time, and blood loss were comparable between the 2 groups.
Table 1
Comparison of operative data between patients with and those without adequate voiding function on POD7
![]()
In univariate analysis (Table 2), factors significantly associated with inability to attain adequate voiding function on POD7 included tumor size larger than 4 cm (p<0.001), postoperative urinary tract infection (p=0.002), and grossly visible tumor (p=0.005). Also, the proportion of patients unable to resume adequate voiding function were significantly different among primary surgeons ranging from 21.4% to 72.4% (p<0.001). In addition, patients with prior conization had a higher chance of resuming adequate voiding function on POD7 (p=0.001). Compared to a cohort of 73 patients who had type B2 radical hysterectomy at our institution in the same period, significantly higher proportion of the patients in the present study were unable to resume adequate voiding on POD7 (49.3% vs. 16.4%, p<0.001).
Table 2
Association between clinico-pathological characteristics and inability to attain adequate voiding function

Data expressed as number of patients (%).
POD7, postoperative day 7; SIL, squamous intraepithelial lesion.
*Statistically significant.
![]()
In multivariate analysis that takes into account tumor size, tumor appearance (gross vs. microscopic), stage, preoperative chemotherapy, postoperative urinary tract infection, primary surgeon, prior conization, length of vaginal and parametrial resection, and parametrial margin, tumor size >4 cm, postoperative urinary tract infection, and primary surgeon were significantly associated with inability to attain adequate voiding function on POD7 (Table 3).

DISCUSSION
Approximately half of the patients in this study cohort resumed adequate voiding function on POD7. This can be compared favorably to our historical cohort data from January to August 2005, which was the period that NSRH was initially adopted at our institution [14]. In that small series comprising 22 patients that had NSRH, 36% of the patients had PVR urine volume of <100 mL and 27% had PVR of <50 mL at the initial removal of the catheter on POD7. Of note, on the fourteenth day after surgery, 82% and 77% of the patients in that series had the PVR of <100 mL and <50 mL, respectively. For the present study, factors significantly associated with inability to attain adequate voiding function on POD7 included tumor size >4 cm, postoperative urinary tract infection, and primary surgeon. This finding not only emphasizes the impact of disease extent that dictates surgical radicality, but also infection and technical variation on the resumption of adequate voiding function following NSRH.
Parametrial (paracervical) resection is an essential and most complicated part of the radical hysterectomy procedure that determines both oncological adequacy and potential morbidities especially those related to pelvic autonomic nerve damage [1516]. The pelvic autonomic nerves originate at superior hypogastric plexus located over the surface of sacral promontory. The plexus, which contains sympathetic nerve fibers responsible for bladder compliance (detrusor muscle relaxation) and urinary continence (urinary sphincter contraction) give rise to bilateral pelvic hypogastric nerves, which course parallel and dorsomedial to the ureters. The hypogastric nerves are joined laterally by pelvic splanchnic nerves to form inferior hypogastric plexus. The pelvic splanchnic nerves originate from sacral nerve roots S2–S4 and carry parasympathetic innervation responsible for bladder emptying (detrusor muscle contraction, urinary sphincter relaxation), rectal function, and vaginal lubrication. The inferior hypogastric plexus provides branches to innervate rectum, vagina, and bladder. Its distal vesical branch is located in the deep layer of vesicouterine/vesicovaginal ligament, which is a part of anterior parametrium, and also forms a flat meshed band on the lateral wall of the upper third of the vagina [3]. The common sites of pelvic nerve injury during radical hysterectomy include proximal inferior hypogastric plexus at the time of rectovaginal/rectouterine and cardinal ligaments (posterolateral parametrium) resection and distal inferior hypogastric plexus at the time of vesicouterine/vesicovaginal ligament (anterior parametrium) and vagina resection [131517]. For type C1 radical hysterectomy, while anatomical landmarks for resection are rather fixed for posterior parametrium (rectum), lateral parametrium (medial aspect of internal iliac vessels), and anterior parametrium (bladder) regardless of tumor size, the extent of vaginal cuff resection is adapted to the dimension of the cervical tumor in relation to the vagina [18]. Therefore, larger tumors would mandate more extensive resection of the vaginal cuff and adjacent vesicovaginal ligament (paracolpium) resulting in higher risk of damage to the vesical branch of the inferior hypogastric plexus even though the nerve-preserving procedure is attempted. The significantly larger dimension of the resected vagina and parametria in the patients with inadequate voiding function found in this study supports this concept (Table 1). In the report by Zullo et al. [3] that examined long-term bladder function in patients who had Piver class 4 radical hysterectomy, the extent of vaginal resection, not the lateral parametrial resection, was significantly associated with bladder storage and voiding dysfunctions. In Possover et al. [7] study, it was suggested that in order to ensure preservation of the parasympathetic nerve fibers in the rectovaginal and vesicovaginal ligaments, the length of vaginal cuff resection should not be more than one-third of the vagina.
Over the past decades, laparoscopic approach for NSRH has been adopted in many institutions with the advantage of clearer visualization of structures including the pelvic autonomic nerve branches in comparison to the conventional open approach [1920]. However, the difference in the recovery of voiding function between patients who had laparoscopic procedure and those with laparotomy could not be demonstrated in our study. Therefore, it is unlikely that the better visualization obtained by employing laparoscopy would translate to additional benefit in avoiding injury to the pelvic autonomic nerves. It would further suggest that visualization is not the limiting factor that affects the effectiveness of the nerve-sparing procedure.
It is important to note that significantly higher proportion of the patient who had type C1 radical hysterectomy were unable to resume adequate voiding on POD7 compared to women who underwent type B2 radical hysterectomy in our institution. This finding emphasizes the inherent limitation of the nerve-sparing procedure. In this respect, neoadjuvant chemotherapy to reduce tumor dimension before radical surgery in patients with large tumor could provide an opportunity to perform type B2 instead of type C radical hysterectomy in those who are chemo-sensitive resulting in less damage to the pelvic nerves.
The updated Querleu-Morrow classification of radical hysterectomy employs distinct anatomical landmarks to classify the procedures into type A to D [18]. The difference in the dimensions of the resected vagina and parametria between the study groups, both had type C1 radical hysterectomy, demonstrated in Table 1 reminded us that in practice, certain degree of variation in term of radicality exists within each classified type of radical hysterectomy.
Apart from operative damage to the pelvic autonomic nerves, it has been suggested that hematoma, infection, perivesical edema, and scar formation are also contributing factors for postoperative bladder dysfunction [31521]. The findings of postoperative urinary tract infection as an independent risk factor for inadequate voiding function in our study supports this idea. It implies that careful attention to prevention, early diagnosis, and treatment of urinary tract infection during preoperative, perioperative, and postoperative periods is important in promoting early resumption of bladder function following NSRH. In patients without preexisting urinary tract infection, method and duration of postoperative bladder drainage can influence the risk of postoperative urinary tract infection. In a retrospective cohort study that compared transurethral catheterization and suprapubic catheterization for postoperative bladder drainage in 212 early-stage cervical cancer patients who underwent radical abdominal hysterectomy, suprapubic catheterization was associated with lower proportion of patients with urinary tract infection (6% vs. 27%) and earlier trial of voiding (2.7 vs. 4.4 days) [22].
The impact of individual surgeons on operative morbidity has been documented in some studies. Coven et al. [23] examined the influence of primary surgeon on operative morbidity of 405 stage IB cervical cancer patients who had radical hysterectomy and pelvic lymphadenectomy by 8 surgeons. In multivariate analysis, primary surgeon was an independent predicting factor for blood loss, blood transfusion, operative duration, postoperative hospital stay, and bladder dysfunction at 3 months postoperatively. In recent meta-analyses assessing the effects of NSRH in comparison to conventional radical hysterectomy on bladder function, there exists a clinically significant heterogeneity among the included studies on time to recovery of bladder function [1224]. These data are in agreement with our finding and imply that the impact of individual surgeon on postoperative recovery of bladder function, though rarely quantified, is significant and should always be taken into account.
In a retrospective study comprising 85 early-stage cervical cancer patients who had radical surgery, Cibula et al. [25] found in multivariate analysis that type D radical hysterectomy and low BMI were significantly associated with longer interval to spontaneous voiding recovery while radical trachelectomy (in comparison with radical hysterectomy) was related to faster resumption of voiding function. Their finding with regard to the impact of extent of parametrial resection on recovery of voiding function is consistent with our finding. However, the significant role of BMI documented in that study was not examined in our study. They reasoned that women with lower BMI tend to have more radical parametrial resection and greater loss of bladder supporting tissue.
This is a large single institutional study with uniform technique of radical hysterectomy. The nerve-sparing philosophy had been well-recognized and adopted by all surgeons involved. However, certain limitations exist. Due to the retrospective nature, data on the exact time when adequate voiding function was achieved in patients who had not resumed adequate voiding on POD7 were not available as most of the patients were discharged from the hospital after POD7 and were seen in the clinic again 6 weeks postoperatively. In those cases, the patients were instructed to monitor voiding at home and to discontinue postvoid intermittent self-catheterization when adequate voiding function is obtained. Furthermore, urodynamic study was not performed for detailed assessment of type and pathophysiology of voiding dysfunction. Nevertheless, the spontaneous voiding volume and postvoid residuum criteria employed in this study to determine voiding function should serve its purpose well in identifying patients with clinically significant voiding dysfunction.
In conclusion, extent of disease represented by tumor size, urinary tract infection as well as individual surgeon's technique independently predict resumption of adequate voiding function on POD7 following NSRH.
 XML Download
XML Download