

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Epithelial ovarian cancer (EOC) is the gynecological malignancy with the highest mortality rate [1]. This may be attributed to the fact that EOC usually presents at an advanced disease stage [2]; the 5-year-survival rate for patients in stage III is reported to be 35% while in stage IV this is as low as 22% [3]. Adequate surgical cytoreduction is the most important independent factor affecting survival in EOC [45678]. Complete tumor removal should be the aim of any primary operative treatment of EOC.
The extent of intra-peritoneal tumor growth and its impact on the completeness of surgical cytoreduction and on survival has been thoroughly studied in colorectal and gastric cancers and accordingly a numerical score, peritoneal cancer index (PCI), was developed. It assesses the extent of intra-peritoneal disease at diagnosis through quantitatively combining the cancer implant size with the tumor distribution throughout 13 abdominopelvic regions, producing a maximum score of 39 [9]. The PCI has been found to be significant in terms of correlating patient disease-free survival (DFS) and overall survival (OS), respectively [91011]. The PCI was found to be a powerful stratification tool to the extent that the treatment of patients with advanced colorectal and gastric carcinomas is now tailored according to the PCI score [121314]. Patients with high PCI scores, above 17, should not be offered aggressive therapeutic measures because they do not provide any survival benefits to those patients [15].
EOC with extensive intra-peritoneal tumor growth represents a surgical challenge for the gynecological oncologist. The extent of cytoreductive surgery should be limited to standard procedures (hysterectomy, bilateral salpingo-oophorectomy, rectosigmoid resection, infragastric omentectomy, pelvic and aortic lymphadenectomy and, when applicable, appendectomy) omitting extensive radical surgical resections (multiple digestive tract resections, total abdominal peritoneum stripping, coeliac lymph node dissection, and abdominal organ resections for example splenectomy, partial gastrectomy, and liver resection) when a complete surgical cytoreduction is not attainable, as advocated by Vidal et al. [16].
It is however worth mentioning that the context of the use of PCI as a prognostic factor while dealing with colorectal and gastric cancers is different from EOC where the application of hyperthermic intraperitoneal chemotherapy (HIPEC), following complete cytoreduction including total abdominal peritoneum stripping, is an integral part of treating colorectal and gastric cancers [10111213] in contrary to the case in EOC where HIPEC is still an experimental procedure that should not be applied outside clinical trials [1718]. This difference in the management strategy may affect the significance of PCI to play a prognostic role in EOC.
This study aimed to examine the PCI score in advanced EOC, correlating it to completeness of surgical cytoreduction, to the clinical outcome of the disease and validating a cut-off value that might have an influence on prognosis in analogy to colorectal and gastric cancers.
MATERIALS AND METHODS
1. Ethical considerations
This was a prospective, observational cohort study that was conducted at El-Shatby Women's University Hospital, University of Alexandria, Egypt. The study was approved by the Ethics Committee, Faculty of Medicine, University of Alexandria (approval number: 160/2010). All of the patients who presented with symptoms that were consistent with advanced EOC and who were being prepared for primary explorative laparotomies between June 2010 and June 2014 provided signed, informed consent to participate in the study.
2. Patient population, assessments, and treatment
The study exclusively involved patients who had advanced EOC of the serous type. The final decision about whether a patient should be included in the study was based on the International Federation of Gynecology and Obstetrics (FIGO) stage and the final histopathology report. Only patients with primary serous EOC at FIGO stages IIIB or higher were included. Patients with FIGO stage IVB with extra-abdominal distant or liver parenchymal metastasis were excluded from the study. The study exclusively included patients with a performance status of 0–2, which was based on the Eastern Cooperative Oncology Group (ECOG) classification [19]. Patients who were assigned to receive neoadjuvant treatment were excluded from this study, as were those who were younger than 18 years or older than 75 years of age. Routine preoperative abdominal and pelvic computed tomography (CT) scans were obtained, and chest radiography was performed. A suspicion of lung metastasis led to the exclusion of the patient from the study, and when malignant pleural effusion was suspected, pleurocentesis was performed for staging purposes and to plan further treatment. After obtaining the final histopathology reports and the final stage was assigned, patients with serous EOC were recruited to the study. A flowchart diagram shows the recruitment procedure in Fig. 1.
Fig. 1
Flowchart diagram of the recruitment procedure in this study.
ECOG, Eastern Cooperative Oncology Group; EOC, epithelial ovarian cancer; FIGO, International Federation of Gynecology and Obstetrics; PCI, peritoneal cancer index.

All patients underwent the standard institutional therapy for ovarian cancer, namely primary surgical cytoreduction, which involved explorative laparotomy, abdominal hysterectomy with bilateral salpingo-oophorectomy omentectomy, peritoneal sampling and eventually stripping if needed, systematic pelvic and para-aortic lymphadenectomy and bowel resection, as recommended by the German Workgroup for Gynecological Oncology (AGO) [20]. Lymphadenectomy and bowel resections were exclusively reserved for patients in whom a complete surgical cytoreduction seemed attainable. The PCI was obtained and registered intraoperatively (Fig. 2). Complete surgical cytoreduction is defined as complete removal of all tumor tissue without any macroscopic residues and is assigned R0. Optimal cytoreduction is defined as incomplete removal of all tumor tissues leaving microscopic or macroscopic tumor residues that are smaller than 1 cm in maximal diameter and assigned R1, while suboptimal cytoreduction is defined as leaving tumor residues larger than 1 cm in maximal diameter and assigned R2. This is based on the final histopathology report. Finding microscopic tumor residues at the resection edge was assigned as R1. Postoperatively, all patients received 6 chemotherapy cycles that comprised a combination of paclitaxel (175 mg/m2 body surface area) and carboplatin (area under the curve [AUC]=5/6), both of which were administered intravenously every 3 weeks as standard adjuvant therapy as recommended by the AGO [20]. The treatment was considered complete after the chemotherapy had finished. A CT scan was performed at completion of chemotherapy in all patients. All patients were followed up for 24 months after chemotherapy completion. The follow-up was in the form of quarterly visits, in which general and gynecological clinical examinations, a transvaginal to detect local recurrences in the pelvis and an abdominal ultrasound to monitor ascites were performed. At clinical suspicion or suggestive symptoms, a CT scan was performed, and compared to the final CT findings at completion of chemotherapy, in order to confirm or exclude a recurrence. This was performed according to recommendations by leading bodies [20]. Patients lost to follow-up were excluded from the statistical analysis. The survival data were registered.

3. Statistical analyses
The data were tabulated using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) and analyzed using IBM® SPSS® for Windows, version 21.0 (IBM Corporation, Armonk, NY, USA). The normality of the data was tested using the one-sample Kolmogorov-Smirnov test. The χ2 test was used to test the associations between categorical variables. Different cut-off points were tested by receiver operator characteristic (ROC) curves to determine the most meaningful cut-off point. Significant variables entered into Logistic regression model using the Forward Wald statistical technique to predict the most significant determinants and to control for possible interactions and confounding effects. The Kaplan-Meier test was used for the survival analysis, and the statistical significance of the differences between the curves was assessed using the log-rank test. For all of the statistical tests, the threshold of significance was set at 5%, and differences were considered significant if the probability of error was less than 5% (p<0.05).
RESULTS
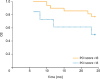
We recruited 96 patients who had EOC of the serous type at FIGO stages IIIB–IVA during the study period. The mean age of the recruited patients±standard deviation (SD) were 52.15±8.98 years, and the median age of the patient cohort was 57 years. Table 1 shows the patient characteristics with respect to tumor grade, FIGO stage, and the extent of surgical cytoreduction. The PCI score had a mean and SD of 11.66±2.25. At the end of the 24-month follow-up period, we registered 29 cancer-related deaths (30.2%). There were 29 cases of disease recurrence or persistence (30.2%) and 38 patients (39.6%) remained disease-free, with a median disease-free interval of 11 months (range 0–24 months). The median OS interval was 21.2 months. A ROC curve plotted the PCI score regarding OS to detect the cut-off value predicting better survival outcome (Fig. 3). A cut-off value of 13 was calculated, above which worse survival is expected (AUC=0.641; 95% confidence interval [CI]=0.517–0.765; sensitivity and specificity 80.6%, 45.0%; respectively; p=0.050). Table 2 shows the correlation of the calculated cut-off level of the PCI score to different clinical and histological parameters in our cohort. Figs. 4 and 5 show the Kaplan-Meier curves taking a PCI score of 13 as a cut-off level for DFS and OS, respectively. The median disease-free interval for patients with PCI ≤13 was 16.3 months (95% CI=14.1–18.4), while for patients with PCI >13 this was 5.6 months (95% CI=2.8–8.3); p≤0.001. The median OS for patients with PCI ≤13 was 22.2 months (95% CI=21.2–23.1) while for patients with PCI >13 was 17.9 months (95% CI=14.9–20.8; p=0.004).
Table 1
Characteristics of the patient cohort

Fig. 3
ROC curve for the PCI score in this cohort regarding OS.
ROC, receiver operator characteristic; OS, overall survival; PCI, peritoneal cancer index.
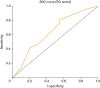
Table 2
Testing the calculated cut-off level of the PCI score regarding different patient parameters in this cohort

Values are presented as number (%).
CI, confidence interval; FIGO, International Federation of Gynecology and Obstetrics; PCI, peritoneal cancer index; OR, odds ratio.
*Each extent means as follow: R0, complete surgical cytoreduction; R1, optimal surgical cytoreduction; R2, suboptimal surgical cytoreduction.
Fig. 4
Kaplan-Meier curve of 2-year DFS for patients with a PCI score ≤13 and those with a score >13 (p≤0.001).
DFS, disease-free survival; PCI, peritoneal cancer index.
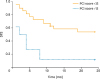
Fig. 5
Kaplan-Meier curve of 2-year OS for patients with a PCI score ≤13 and those with a score >13 (p=0.004).
OS, overall survival; PCI, peritoneal cancer index.
A univariate logistic regression analysis of the factors associated with recurrence in this cohort showed that a PCI score above 13 (odds ratio [OR]=9.104; 95% CI=2.502–33.132; p≤0.001), suboptimal surgical cytoreduction (OR=16.361; 95% CI=4.501–59.470; p≤0.001), and advanced FIGO stage, namely FIGO IIIC and IVA (OR=5.750; 95% CI=2.287–14.456; p≤0.001), had statistically significant impacts on the probability of recurrence. A multivariate analysis determined that, of the factors that had a significant impact on recurrence in the univariate analysis, suboptimal surgical cytoreduction was the only independent predictive factor for recurrence in this cohort (OR=7.548; 95% CI=1.473–38.675; p=0.015).
A univariate logistic regression analysis of the factors that can possibly be associated with death in this cohort, namely PCI score >13, suboptimal surgical cytoreduction, FIGO stage and tumor grading showed that suboptimal surgical cytoreduction (hazard ratio [HR]=2.24; 95% CI=1.23–4.09; p=0.005), and PCI score >13 (HR=2.18; 95% CI=1.22–3.89; p=0.012) were the factors that had a statistically significant impact on OS. A multivariate analysis determined that only suboptimal surgical cytoreduction (HR=2.33; 95% CI=0.616–8.795; p=0.005), but not PCI score >13 (HR=1.289; 95% CI=0.329–5.046; p=0.716), was an independent predictive factor of survival.
DISCUSSION
Predictors of survival in EOC have not changed much in the last few decades despite expanding knowledge about the disease. A complete surgical cytoreduction with removal of all macroscopic detectable tumor tissue remains the most important independent risk factor predicting survival. PCI was thought to be a possible predictor of survival, in analogy to gastric and colorectal cancers. In a recent report on a retrospective cohort, Gasimli and co-workers [21] concluded that PCI is not adequate as an independent predictor of survival, although their data found a significant impact on DFS in the multivariate analysis. In another recent report, PCI was concluded to be a reliable predictor of the completeness of surgical cytoreduction. Its ability to predict survival was not, however, reported in this study [22].
Complete surgical cytoreduction may not be attainable in advanced EOC cases. A possible option for such patients may be neoadjuvant chemotherapy followed by interval debulking, which was proved non-inferior to primary debulking surgery in randomized controlled trials [2324]. Moreover, a work group from Leuven University suggested selection criteria according to which neoadjuvant chemotherapy and interval debulking are offered to the patients. These criteria are poor general condition of the patient, tumors larger than 2 cm around the superior mesenteric artery or behind porta hepatis, multiple liver metastasis or extra abdominal metastasis, extensive serosal invasion of the intestine necessitating a resection of more than 1.5 m of bowel length and patients who cannot receive a complete surgical cytoreduction under reasonable conditions (more than 1 bowel resection, operative time more than 4 hours) [25].
In analogy to colorectal and gastric cancer and based on the findings that chemotherapeutic agents administered intraperitoneally at high temperatures have more cytotoxic effect [2627], some authors reported a role for HIPEC combined with complete surgical cytoreduction after extensive surgical procedures in providing patients with primary and recurrent EOC an improvement in overall and in DFS in comparison with the standard of care namely primary surgical cytoreduction followed by adjuvant systemic chemotherapy [28293031]. The available data regards this therapeutic modality is heterogenous and cannot offer solid ground to consider HIPEC as a standard treatment option for EOC patients [1732].
This is the first report to date to prospectively study the significance of PCI as a predictor of survival. Although a cut-off value of 13 was calculated, above which the prognosis is significantly worse and the completeness of surgical cytoreduction is less likely (the calculated PCI cut-off for complete surgical cytoreduction is 12 in this cohort), the PCI score did not seem to be a clear independent predictor of survival in EOC, in contrast to data from gastric and colorectal cancer. The completeness of surgical cytoreduction remains the most important independent predictor of survival in EOC, even if a high PCI score is inversely proportional to the completeness of surgical cytoreduction. This remains a significant effect of high PCI score on the possibility of the completeness of surgical cytoreduction, but does not qualify the PCI score as a predictor of survival. The PCI score remains, however, a practical clinical tool with applications that should be further assessed in future studies.
The PCI score may help predicting complete surgical cytoreduction as seen in in published data [22], these needs, however, to be further assessed in larger prospective studies. Possible drawbacks of this study are the fact that 34.4% of the patients were FIGO stage IIIB and that in 64.6% of the patients a complete surgical cytoreduction was possible. Moreover, the maximum PCI score in our cohort was only 19, whereas the absolute maximum PCI score is 39. This could raise claims that this cohort included patients with EOC that was not very advanced, representing a selection bias. This bias is due to the inclusion of patients with FIGO stage IIIB that is postoperatively assigned that have been probably intraoperatively assigned as FIGO stage II leading to recruiting cases that are not advanced enough leading to a low PCI score in this cohort. The PCI score was determined intraoperatively while the FIGO stage was assigned postoperatively.
We conclude from this study that the PCI score is a reliable tool helping to assess the extent of disease intraoperatively in advanced serous EOC patients. PCI score may also help predict complete surgical cytoreduction, however, a PCI cut-off score that has prognostic significance could not be extrapolated from this cohort. The findings of this study should be further validated in prospective studies including a larger cohort of patients with longer follow-up periods.
 XML Download
XML Download