

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
The cervical cancer incidence of 10.9 per 100,000 person-years was the second most common female cancer and the second leading cause of cancer deaths in women aged 15 to 44 years in Japan in 2012 [12]. Cervical intraepithelial neoplasia (CIN), usually graded CIN1 (mild), CIN2 (moderate), and CIN3 (severe) and also known as cervical dysplasia, is the potentially premalignant transformation and abnormal growth of squamous cells on the surface of the cervix [34]. The major cause of CIN is chronic infection of the cervix with the sexually transmitted human papillomavirus (HPV) [45]. World Health Organization (WHO) guidelines [6] adopted the pathological term squamous intraepithelial lesion (SIL), which has been a general term in cytology of The Bethesda System [7], for screening and treatment of precancerous lesions for cervical cancer prevention. Low squamous intraepithelial lesion (LSIL) is recognized as an infectious lesion by HPV whereas high squamous intraepithelial lesion (HSIL) is a neoplasia that may include CIN2 and CIN3 [4]. The Japanese Treatment Guideline [8] recommends that CIN1 and 2 be monitored together as a single category rather than treated because 70% of CIN1 spontaneously will regress within 1 year, 90% will regress within 2 years, and about 50% of CIN2 will regress within 2 years without treatment [91011]. On the other hand, CIN3 should be treated by excision or ablation with postoperative follow up for at least 2 to 5 years to observe for possible recurrence [1213]. The median time from CIN2/CIN3 to cancer has been estimated to be 23.5 years with 1.6% of lesions progressing to cancer within 10 years [12], whereas in an ethically controversial New Zealand study 31.3% of CIN3 lesions were observed to progress to cancer within 30 years [13].
The main aim of detecting CIN precancerous lesions via the clinical and laboratory pathways of cytology, histology and colposcopy is to treat and prevent them from developing into invasive cancer [1415]. There are 2 approaches to managing and treating CIN: continued observation (with cervical cytology, HPV testing, and colposcopy) and treatment with an excision or ablation by conization of the cervical transformation zone (an anatomic area that contains the transition from the squamous epithelium of the ectocervix to the glandular epithelium of the endocervix), or less commonly, hysterectomy [1617181920]. In some clinical contexts, “see-and-treat” protocols are used, in which evaluation and management are performed at the same visit. Decisions regarding management of CIN depend upon the risk of cervical cancer, risks associated with treatment, and the likelihood of compliance with a management plan. Continued observation is used in Japan for CIN1 and 2 lesions that are highly likely to regress. CIN3 lesions are associated with a high risk of developing cervical cancer, and these are typically treated with cervical excision or ablation. However, there is some chance that these lesions will regress and observation is preferred for some patients. This is particularly the case for women who plan future childbearing, since excisional procedures may result in future adverse obstetric outcomes [2122]. Treatment is generally performed based upon histologic results from colposcopically-directed biopsy [21232425]. In some cases, when colposcopy is not adequate and/or there are recurrent high-grade cytologic findings (atypical squamous cells, cannot rule out high-grade squamous intraepithelial lesion [ASC-H] or HSIL), an excisional procedure is performed by conization for the purpose of diagnosis and further treatment might not be required [1920]. In addition, treatment in “see-and-treat” protocols is provided based upon colposcopic appearance of a lesion without confirmation from a biopsy result [21]. The treatment policy for CIN may vary substantially between Japan and other countries such as USA [141521] thereby compromising stringent and meaningful statistical comparisons between different countries [26].
When cervical biopsy specimens are diagnosed histologically as CIN1 and 2, how should we treat or observe such lesions? In order to evaluate the clinical efficacy of the conservative treatment of CIN grades 1 and 2, we undertook a retrospective study of the clinical management of the pre- and postoperative diagnosis and treatment by conization of 13,215 cervical precancerous lesions in Japan in the years of 2009 and 2011.
MATERIALS AND METHODS
A nation-wide survey was undertaken in 2009 and 2011 to collect the results from 205 Japanese institutions of 14,185 consecutive cases of women who were managed for cervical precancers and treated by cervical conization (excision) with at least a 2-year follow up. The data in the Japan Society of Obstetrics and Gynecology (JSOG) nation-wide registry for cervical cancer (2009 and 2011) was collected and used to analyze the clinical efficacy of diagnosis and conservative treatment of CIN grades 1 and 2 for 13,215 Japanese patients who underwent treatment by conization. Their preoperative and postoperative histologic findings and clinical outcomes were evaluated using standard statistical procedures including clinical and demographic characteristics of the 13,215 patients.
The pretreatment diagnostic protocols for recommended conization involved cytology (LSIL or HSIL), colposcopy, biopsy, and CIN or invasive cancer histologic reporting [820]. Prediagnosis of CIN was based on biopsy results. Conization was used for ‘therapeutic’ and/or ‘diagnostic’ purposes. The ‘therapeutic’ use of conization defines the successful treatment of lesions by excision whereby the pathologic indicators of cytology, coloposcopy and histology all showed the same successful results. On the other hand, ‘diagnostic’ defines the use of conization to identify severe lesions whereby the prior results of cytology, coloposcopy and histology disagreed and that suspicious invasive cases required a correction in diagnosis for staging and treatment. We used the histologic results of CIN categories or the International Federation of Gynecology and Obstetrics (FIGO) staging of cervical carcinomas rather than the cytological results for assessing the pre- and posttreatment of cervical cancers. The FIGO staging of cervical carcinomas was IA, IA1, IA2, IB, IB1, and IB2 [27]. Adenocarcinoma in situ was reported as ‘AIS,’ whereas sarcomas and polyps were reported as ‘other.’ Surgical margins were reported as negative when margins of the biopsies were visibly free of penetrating tumor cells, and as positive when tumor cells were found in the margins. Additional treatment for those with surgical margin positive involved hysterectomy, repeat conization or radiation therapy. The average numbers of different groups and categories in the analyses were calculated as the mean and the standard deviation of the mean (SDM) using Statistical Package for Social Sciences 11.01 (SPSS Inc., Chicago, IL, USA). The p-values of equal to or less than 0.05 without corrections were considered to be statistically significant. The study was approved by the ethics committee of Tokai University (Institutional Review Board [IRB] registration number, 15R-095).
RESULTS
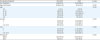
Pathological and clinical data was collected from 205 Japanese institutions of a total of 14,832 cases that were treated for cervical precancers by cervical conization in 2009 and 2011. Of the 14,832 women, 13,215 underwent conization after prediagnosis of CIN. Of these, 1,536 women were diagnosed with CIN1 and 2, and 1,1679 women were diagnosed with CIN3. Table 1 shows the clinical and demographic characteristics of the 13,215 women who were treated by cervical conization based on the diagnosis of CIN1, 2, and CIN3. In general, there was a significant difference between the characteristics of the patients who were diagnosed for CIN1 and 2 and those diagnosed with CIN3. There were a significantly greater number of women diagnosed with CIN3 (88.4%) than CIN1 and 2 (11.6%). However, the women with CIN1 and 2 on average were older with higher percentage of gravida, parity and menopause than the CIN3 patients. More than 70% of the cervical precancerous patients were in the age brackets between 31–40 and 41–50 years of age, but there were a small number (19) of cases of CIN3 who were less than 20 years of age (0.2%).
Table 1
Clinical and demographic characteristics of 13,215 patients who were treated by conization based on the preoperative diagnosis of CIN1 and 2, and CIN3
All of the 13,215 women who had been treated by cervical conization had the surgically removed tissue diagnosed by histology. Table 2 shows the results of the postoperative histological diagnosis. Surprisingly, 52.1% of the 1,536 lesions diagnosed preoperatively as CIN1 and 2 were diagnosed postoperatively as CIN3 (47%) or greater (IA1, IA2, IB1 or more, and AIS). Interestingly, the cases with CIN1 and 2 were treated by cervical conization either for therapeutic (78.5%) or diagnostic (21.5%) reasons because the lesions of these patients showed no evidence of natural regression or there was some evidence of special or unusual conditions during the preoperative diagnoses. On the other hand, 88.7% of the 10,670 lesions diagnosed preoperatively as CIN3 were found postoperatively to have been diagnosed histologically as CIN3 (82.2%) or greater (IA1, IA2, IB1 or more, and AIS). The incomplete excision of the cervical lesion by conization is reported as the positive surgical margin and this occurred significantly more (p<0.001) in the CIN3 preoperative cases (15.2%) than the CIN1 and 2 preoperative cases (10.5%). All of these 13,215 cases were observed postoperatively on average for about 30 months and recurrence of lesions was low for the preoperative cases of CIN1 and 2 at 3.9% and of CIN3 at 4.3%.
Table 2
Postoperative histological diagnosis after conization of CIN lesions from 13,215 patients
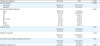
Table 3 shows the clinical and demographic characteristics of 1,536 women diagnosed preoperatively with CIN1–2 and who were treated by cervical conization for therapeutic or diagnostic reasons. The differences between the therapeutic and diagnostic groups were statistically significant (p<0.05) for the number in each group, average age, age distribution, postcone histological diagnosis (invasive disease 2.8% in therapeutic cases and 6.1% in diagnostic cases), the need for additional treatment, and the number of months of postoperative observation. Overall, however, there were only marginal differences between the characteristics of the 2 groups in regard to the age brackets (31 to 50 years of age), and rates of recurrence. In general, the women chosen for diagnostic conization were older, had more invasive lesions (6.1%) and more required additional treatment (10%) than the patients chosen for therapeutic conization. In addition, the positive surgical margins were fewer in the diagnostic conization group (7.6%) than in the therapeutic conization group (11.3%). Of the 1536 women with the preconization diagnosis of CIN1 and 2, including those selected for conization for therapeutic and diagnostic reasons, 41 (2.7%) were diagnosed postoperatively with invasive disease (IA1, IA2, IB1 or more) and 21 were found with cervical adenocarcinoma in situ (AIS) (Table 2).
Table 3
Clinical and demographic characteristics of 1,536 patients diagnosed preoperatively with CIN

Table 4 shows the additional treatment regime for 41 patients who were diagnosed with invasive disease after histological examination of their cervical tissue that was removed by the conization procedure. Of the 41 women with invasive disease, 14 patients were treated successfully by the initial conization with no evidence of recurrence after about 30 months of postoperative observation and they required no further treatment. One of the 15 untreated patients was lost during follow up and the success of her postoperative outcome is not known. Twenty-six of the patients with invasive disease received additional treatment; 2 were reconed, 23 had hysterectomies, and one was treated by radiation. A total of 1,535 women with the preconization diagnosis of CIN1 and 2 survived their diagnostic and therapeutic cervical conization treatment after approximately 30 months of follow up, and one of the 1,536 women with the preconization diagnosis of CIN1 and 2 did not participate in the follow up.
Table 4
Treatment of 41 patients diagnosed after conization with invasive disease

DISCUSSION
This survey showed that almost 50% of patients who were initially diagnosed with CIN1 and 2 actually contained CIN3 or invasive cancer in their cervical tissue. Since approximately two thirds of the CIN1 lesion is expected to regress naturally [10111218], these lesions are usually monitored by repeat cytology and occasionally by colposcopy over a 5-year period or longer, and not treated by excision or ablation methods such as conization [141921]. On the other hand, CIN2 and 3 have a higher risk of progression to cervical cancer if left untreated [1213], and therefore, these lesions are treated by conization [172325] or followed closely by colposcopy, biopsy and histology [1819202124]. In addition, CIN3 is often missed or misdiagnosed as CIN1 or 2 by the initial inspection or screening procedure using cytology and colposcopy [27] because of low sensitivity and specificity, poor technique, incorrect biopsy site or the presence of multiple lesions with different grades of CIN [212428]. In our study, the Japanese patients with CIN1 and/or 2 underwent conization mostly because the attending colposcopists considered that these low-grade lesions showed unnatural persistence or that there was some evidence of special or unusual conditions (possible adenocarcinomas, hidden squamo-columnar junction, multiple foci, and lesion size and location) during the preoperative diagnoses by cytology, colposcopy and occasional histology. Those patients contained CIN1–2 (45.0%), CIN3 (47%), or invasive cancer (2.7%) in their cervical tissue that was excised by conization. This result means that attending colposcopists were able to sort patients with higher lesions as expected during continued observation. In this regard, our results are similar to those previously reported by Ueda et al. [29] who found that 44.1% of their 660 Japanese patients diagnosed preoperatively with CIN1 and 2 had a higher severity of lesions (CIN3 and invasive cancer) when the tissue was excised by conization and diagnosed histologically. They concluded that the discrepancy between the preoperative and the postoperative biopsy results often occurred when the squamous-columnar junction was not clearly visible. In addition, Ueda et al. [29] reported that invasive cancer was detected in 151 (7.2%) of 2,107 cases in the biopsy after conization and that the invasive disease was statistically higher in preoperative CIN3 than in CIN1 or 2 cases. We obtained similar but slightly lower results in that in our study the invasive cancer was detected in 700 (5.3%) of 13,215 cases in the biopsy after conization and that the invasive disease was statistically higher in preoperative CIN3 (5.6%) than in CIN1 or 2 (2.9%) cases. The recurrence rate of 4% for cervical lesions or discovery of invasive carcinoma after conization was lower or within the same range in our study as in previous reports [2325293031].
The initial diagnosis of cervical precancerous lesions in the 2009 and 2011 study was reliant on cytology and histological biopsies after the visualization of cervical surface changes by colposcopy. The screening protocol was cytology (LSIL or HSIL), colposcopy, biopsy and histological reporting of CIN1 and 2 or CIN3 and then reexamination by colposcopy and treatment by conization. Treatment was recommended in the case of CIN1 and 2 if there was no natural regression of the lesion or special conditions were observed. In this regard, there is a different management and consensus between the USA and Japan whereby the continued observation of CIN2 and CIN3 with sequential cytology and colposcopy is less acceptable in the USA, except in pregnant and young women [6142122]. There are also clear differences between Japan and the USA in the management and treatment of cervical cancer patients [2033]. In Japan, the primary goal of continuous cervical cancer screening by cytology, colposcopy and histology is to detect CIN in order to detect and prevent early invasive cancer. Our study suggests that this goal was achieved successfully in 2009 and 2011 largely by the JSOG education strategy and their screening, management and treatment protocols [8].
From our analysis of the outcomes and treatments of the cases initially diagnosed with CIN1 and 2 in the 2009 and 2011 registered groups we conclude that these patients achieved satisfactory clinical outcomes and that there does not seem to be a need for any immediate change to the clinical approach in the diagnosis and treatment of precancerous lesions of the cervix. In addition, there are new recommendations for using ‘the continued observation principle’ based on HPV typing of CIN1 and 2 as described in the Guideline for Gynecologic Practice in Japan 2017 and revised by JSOG [6832]. Since the HPV typing test for CIN1 and 2 patients is covered by health insurance in Japan, most physicians are expected to use this additional test in the future. Similarly, the use of an HPV test, cytology and colposcopy as a triage to diagnosis cervical precancers has been recommended by other national and international organizations [141518212232]. In this regard, the results of our study of the diagnosis and treatment of women with cervical precancerous lesions in 2009 and 2011 sets an important benchmark for future studies whereby the diagnosis and treatment modes have changed more towards the perspective of an HPV genital infection rather than that of a non-viral dysplasia. Nevertheless, from our analyses of the large-scale observational study of conization, we conclude that cervical lesions should be observed and diagnosed carefully with cytology, colposcopy, HPV genotyping, and histology of cone biopsy, which is now the standard practice throughout Japan. In addition, all future pathological (cytological and histological) reports of HSIL should be reported as HSIL/CIN2 or HSIL/CIN3 in the hope that pathological diagnosis of LSIL and HSIL will be established more clearly and related better to the clinical behavior and HPV typing of precancerous lesions of the uterine cervix.
 XML Download
XML Download