

 PDF
PDF ePub
ePub Citation
Citation Print
Print


A 58-year-old Asian male presented to the emergency department with sudden unsteadiness starting on the previous day, accompanied by non-spinning type of dizziness and vomiting. The patient had no prior history of a stroke or cardiovascular disease except for type 2 diabetes mellitus. He had been smoking tobacco for 15 pack-years. His initial vital signs and cardiac examination were unremarkable. The neurological examination revealed left-sided limb ataxia, using the heel to shin and finger to nose tests, and gait ataxia. A brain magnetic resonance imaging (MRI) revealed multiple acute cerebellar infarct lesions in the posterior inferior cerebellar artery territories (Fig. 1). The laboratory findings were unremarkable. The electrocardiography exhibited normal sinus rhythm. Two-dimensional transthoracic echocardiography showed a normal heart configuration. To evaluate a potential cardiac source of the embolism, transesophageal echocardiography (TEE) was performed. No definite thrombus or intracardiac shunt was identified, but the left atrial appendage (LAA) was not shown on the TEE (Fig. 2A, B). To exclude any thrombotic occlusion of the LAA or ectopic appendages, contrast-enhanced multidetector computed tomography was performed and confirmed a diagnosis of the absence of the LAA (Fig. 2C, D). The congenital absence of the LAA is a quite rare cardiac anomaly, and only a few cases have been reported in the literature.123 The clinical significance of the anomaly was not elucidated. Most of the reported cases of the congenital absence of the LAA were diagnosed during an evaluation of a possible thrombus in the left atrium or LAA for rhythm control of atrial fibrillation. No patients had a history of embolic events among those cases. Although the congenital absence of the LAA was considered as an incidental finding, the present case highlights that various etiologies can evoke stroke events and defining stroke mechanisms is important for effective stroke prevention, in the era of LAA intervention.
Figures and Tables
FIG. 1
T2-weighted (A, B), diffusion (C) and apparent diffusion coefficient (D) brain magnetic resonance imaging of the patient reveals acute infarctions in both cerebellums associated with the posteroinferior cellebellar artery (left dominant).
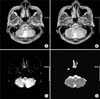
FIG. 2
Multiple transesophageal echocardiography image views at the midesophageal level (A, B). It was impossible to visualize the left atrial appendage in its typical location. Contrast-enhanced multidetector computed tomography with axial (C) and 3 dimensional volume-rendering (D) images. The left atrial appendage was not visualized. In contrast, the great cardiac vein and left circumflex coronary artery were clearly observed along with the atrioventricular groove. LA: left atrium, LV: left ventricle, LPV: left pulmonary vein, GCV: great cardiac vein, LCx: left circumflex coronary artery.

References
1. Collier P, Cavalcante JL, Phelan D, Thavendiranathan P, Dahiya A, Grant A, et al. Congenital absence of the left atrial appendage. Circ Cardiovasc Imaging. 2012; 5:549–550.

2. Zhang ZJ, Dong JZ, Ma CS. Congenital absence of the left atrial appendage: a rare anatomical variation with clinical significance. Acta Cardiol. 2013; 68:325–327.
3. Song IG, Kim SH, Oh YS, Rho TH. Underdevelopment of left atrial appendage. Korean Circ J. 2017; 47:141–143.
 XML Download
XML Download