

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anti-HCV is detectable 8–12 weeks after hepatitis C virus (HCV) infection [1]. As antibodies against HCV are not neutralizing, they are detected not only in chronic hepatitis C patients but also in the majority of recovered patients. Thus, anti-HCV positivity cannot clearly distinguish current, active infection from past infection [2], and positive anti-HCV results can indicate active HCV infection (acute or chronic), past, resolved HCV infection, or a false-positive anti-HCV result [34]. False positives may occur under conditions of myeloma, rheumatoid arthritis, liver cirrhosis, cancer, or autoimmune diseases (collagenous, autoimmune hepatitis) [56]. Anti-HCV testing by third-generation anti-HCV ELISA shows a high false-positive rate of 15–60% (mean 35%) in low-risk groups for HCV infection, such as blood donors and healthcare workers as well as the general population [7891011121314]. To overcome this issue, efforts have been made to reduce false-positive results by adjusting the signal-to-cutoff (S/CO) ratio [615161718] or by conducting additional tests, such as the nucleic acid amplification test (NAAT) or the recombinant immunoblot assay (RIBA) [192021]. In 2003, the US Centers for Disease Control and Prevention recommended a S/CO ratio for anti-HCV screening tests and a diagnostic algorithm that involves NAAT and RIBA [19]. In July 2013, an updated HCV testing algorithm involving sequential testing of anti-HCV screening-positive samples with HCV RNA using only the NAAT was published [20]. The most important change to the testing algorithm was the withdrawal of the US Food and Drug Administration approval of RIBA, a supplemental test for anti-HCV. Therefore, it became challenging to discriminate false-positive anti-HCV results from past, resolved HCV infection by the NAAT alone.
Past, resolved HCV infection and false-positive anti-HCV results are problematic in two aspects. First, when a patient tests positive for anti-HCV, especially during a medical checkup, clinicians will strive to determine false positivity not only through laboratory approaches but also by using imaging techniques, such as ultrasonography and computed tomography. As HCV requires continuous monitoring since reinfection can occur even after recovery [22], false positivity may have significant consequences for the patient in terms of time and cost. Second, patients with a false-positive anti-HCV result are incorrectly banned from donating blood. However, this is not an issue for past, resolved HCV infection patients. In retrospective studies [2324], there were no confirmed cases of infection from transfusion of blood that tested positive for anti-HCV, negative or indeterminate for RIBA, that is, false-positive anti-HCV.
Thus, accurate interpretation of anti-HCV-positive results and a clear distinction between past, resolved HCV infection and a false-positive result is needed. We performed both the NAAT and RIBA as confirmatory tests on samples that showed positive results of anti-HCV by two immunoassay (IA) systems. On the basis of the test results, we assessed the diagnostic performance of each IA based on the S/CO ratio, and explored an algorithm with optimal efficiency that assesses the anti-HCV results of one or two IAs.
METHODS
1. Study population
This retrospective study was performed between July 2013 and June 2016 at Seoul National University Bundang Hospital, Seongnam, Korea. We tested 126,919 patients and 44,556 individuals from those undergoing a medical checkup for anti-HCV using the ARCHITECT (Abbott Diagnostics, Wiesbaden, Germany) and Access (Bio-Rad, Marnes-la-Coquette, France) systems. All positive anti-HCV serum samples were tested on each assay repeatedly, and the NAAT and RIBA were performed as supplemental tests to confirm positive anti-HCV results. As of April 2014, the results were reported as positive when a S/CO ratio ≥5 in ARCHITECT and ≥3 in Access were achieved simultaneously, without any additional supplemental tests.
In total, 2,388 (1.39%) samples tested positive in the anti-HCV screening. We evaluated the 1,035 samples that remained after applying the following exclusion criteria: patients in the follow-up phase, no NAAT or RIBA results owing to lack of sample, and results with S/CO ratio of ≥5 in ARCHITECT and ≥3 in Access after April 2014. This study was approved by the Seoul National University Bundang Hospital institutional review board (B-1609/361-103). The need for written informed consent was waived.
2. Anti-HCV assays for HCV infection screening
For patient testing, we used the ARCHITECT anti-HCV chemiluminescent microparticle IA (CMIA) on an ARCHITECT i2000 analyzer. For testing of the medical checkup population, we used the Access HCV Ab PLUS chemiluminescent IA (CIA) on an Access 2 analyzer. The ARCHITECT CMIA employs recombinant antigens to c100-3 (NS4) (yeast-derived), a fusion protein of two noncontiguous coding regions of NS3, and a core produced in Escherichia coli and referred to as HCr43 (HCV Chiron 43) for antibody capture. The Access HCV Ab PLUS CIA includes paramagnetic particles coated with recombinant proteins (NS3/NS4) and capsid peptide suspended in Tris buffer. The S/CO ratio was recorded directly from the automated system. As per the manufacturer's guidelines, a test result was considered positive when the S/CO ratio was ≥1.
3. Supplemental testing of anti-HCV-positive samples
The NAAT for HCV RNA was performed using the Abbott RealTime HCV PCR (Abbott Diagnostics, Illinois, USA). The limit of detection of the RealTime HCV PCR assay was 30 IU/mL, with 0.2 mL used for sample preparation. RIBA was conducted using the HCV BLOT 3.0 Strip Immunoblot Assay (MP Diagnostics, Illkirch Cedex, France). The nitrocellulose strips contain four recombinant HCV proteins from both structural (core) and nonstructural (NS3, NS4, and NS5) viral antigen regions. For this assay, the intensity of the colored bands on a nitrocellulose strip is proportional to the amount of bound antibody and was graded as negative, ±, 1+, 2+, 3+, or 4+, according to the manufacturer's instructions. The positive results are either >1+ reactivity with at least 2 HCV antigens or 2+ reactivity to the core band only. An indeterminate result was defined as any single HCV band of 1+ or greater reactivity that did not meet the positive criteria. A negative result was defined as no bands of ≥1+. The tests were carried out according to the manufacturer's instructions.
4. Interpretation
Samples that tested positive for anti-HCV and for the NAAT were considered true positive, with present HCV infection. Negative NAAT with positive RIBA result indicated true positive and past, resolved HCV infection. Other results (negative or indeterminate RIBA results) were regarded as biological false-positive anti-HCV results [19].
5. Statistical analysis
We used the Wilcoxon signed rank test in SPSS ver. 22.0 (IBM Co., Armonk, NY, USA) to compare the results of a repeat test and of the IA. P values of <0.05 from two-sided tests were considered statistically significant. Sensitivity and positive predictive value (PPV) were presented as percentages. We used the Wilson score method [25] without continuity correction in Microsoft Excel 2010 software (Microsoft Corporation, Redmond, WA, USA) to calculate a 95% confidence interval (CI) for a proportion. We calculated the mean and standard deviation (SD) of anti-HCV S/CO values according to the NAAT and RIBA results.
RESULTS
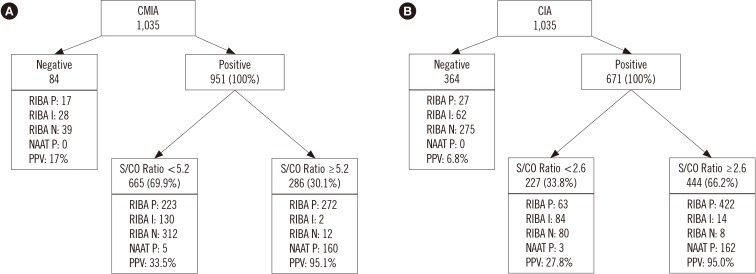
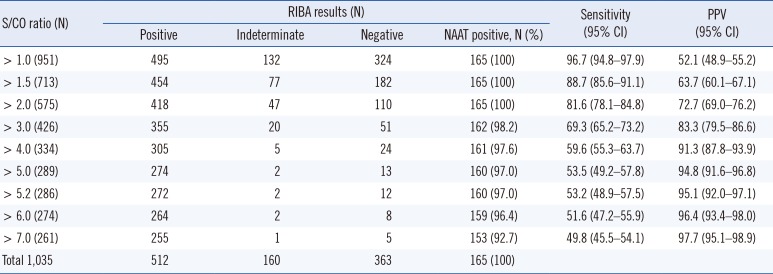
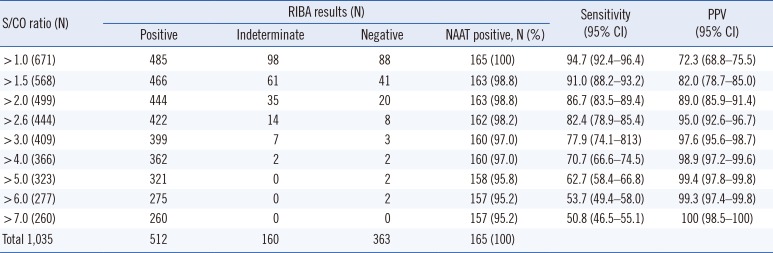
Among the 1,035 samples with positive anti-HCV, RIBA was positive in 512 (47.9%; 163 were NAAT positive), indeterminate in 160 (15.2%; none were NAAT positive), and negative in 363 (36.9%; two were NAAT positive) samples. The results of the two anti-HCV assays were discordant in 448 samples (41.9%); among these discordant samples, CMIA-positive and CIA-negative results were observed in 84 samples, and CIA-positive and CMIA-negative results were observed in 364 samples.
We determined the optimal values for the S/CO ratios of CMIA and CIA results that simultaneously satisfied PPV ≥95% and false-positive rate <5% to be 5.2 and 2.6, respectively (Tables 1 and 2; Fig. 1).
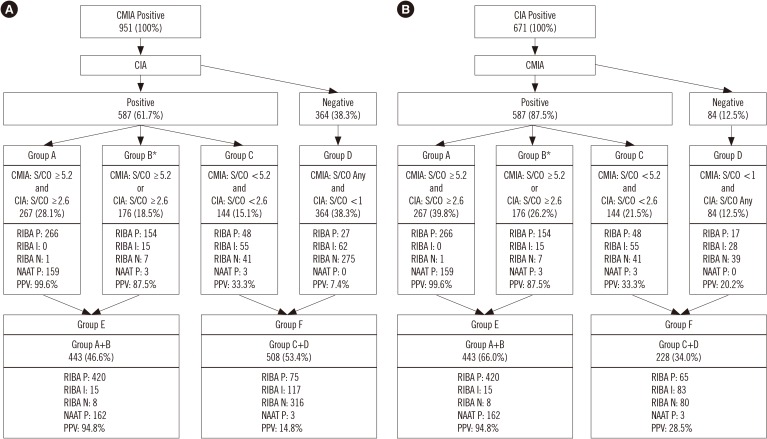
On the basis of these results, we established an algorithm for screening anti-HCV with two different IAs and categorized the results in groups A to F by the optimal S/CO ratio for each IA (Fig. 2). In total, 267 samples met the criteria for the S/CO ratio concurrently in each IA, with a PPV of 99.6% (1 false-positive anti-HCV), whereas 443 samples met only one criterion for the S/CO ratio, with a PPV of 94.8% (23 false-positive anti-HCV). Sequencing before and after the two IAs did not affect the results of groups A, B, and E. However, depending on the performance of each IA, a different number of samples should have been tested with a supplemental test (group F).
DISCUSSION
We investigated two models for detecting anti-HCV positivity. The first model uses only one IA for anti-HCV testing. In this case, the results are reported simply in reference to the S/CO with 95% PPV: a higher value is reported as positive and a lower value as weak positive. Weak positives should be tested for false positivity through an additional supplemental test. S/CO values with 95% PPV were 5.2 for CMIA and 2.6 for CIA. Thus, the CMIA has a higher false-positive rate and a two-fold greater S/CO value than CIA. Previous studies have also reported high false-positive rates for anti-HCV tests using the ARCHITECT system [152627]. The second model uses two different IAs for anti-HCV testing, which allows for mutual complementation with a cross-check comparison between test results. If the first IA shows a positive anti-HCV result, then the second IA may be used to re-examine and report the results by each S/CO ratio.
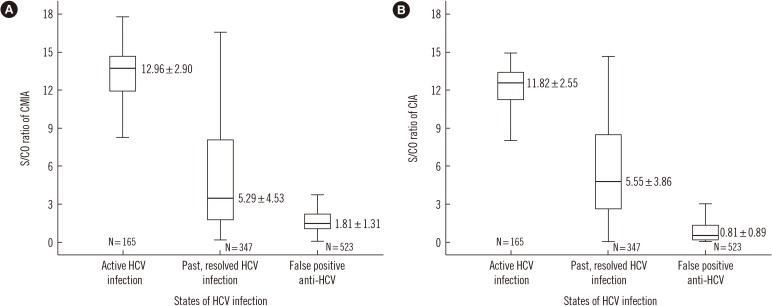
The two models delineated above did not use a repeat test or a supplemental test such as HCV NAAT. Most manufacturers recommend retesting with a duplicate if the anti-HCV test shows a positive result. Some studies report cases of a repeat test contributing to the final evaluation [16]. However, in the present study, of the 1,035 samples that were reflex-tested before applying the exclusion rule in CMIA, nine cases of discrepancy were identified under the S/CO 1 criterion, all of which were negative for HCV NAAT and RIBA. Therefore, repeat tests did not affect the results. In case of CIA, a total of 172 samples were repeatedly tested, but none of the samples showed different results. Although the repeat test may be used to identify errors resulting from the mix-up of samples as well as sampling and handling errors [28], our study showed that repeat tests are not necessary. This is because the biological false reaction still showed a result within the range of tolerable bias (data not shown), even after a repeat test with the same IA. In previous studies, a higher anti-HCV S/CO ratio indicated current infection and positive NAAT results [2129]. This study also showed that the NAAT-positive samples had average S/CO values >2-fold higher than those of negative samples (Table 3 and Fig. 3).
To determine HCV infection in the case of low S/CO ratio, for which determination is difficult, we reviewed the medical records of 43 patients with indeterminate RIBA results. There were eight (18.6%) true HCV-infected patients (resolved), and the rest were eight cancer patients, nine medical checkup patients, and 18 patients with other illnesses. S/CO ratios <2 were observed in 30 (70%) patients, and no patients were positive for the NAAT, which is in accordance with a previous report [5]. For patients with past, resolved HCV infection, the S/CO ratio declined from >10 to 1–2 over time. One patient showed a marked decline in the S/CO ratio to <2 within only two years. A high S/CO ratio with a negative NAAT may be regarded as a resolved infection [30]. However, in the patients with spontaneous recovery after infection without subjective symptoms (15–45%) [4], it is difficult to distinguish false-positive results from low S/CO ratio solely on the basis of their medical history, as they overlap with the false-positive results at low S/CO ratios. Therefore, supplemental tests can assist the clinician in decision-making, which may be crucial. However, since the only currently available laboratory test is the NAAT, which is not highly indicative, S/CO ratio analysis is the most important component. The anti-HCV S/CO ratio and HCV infection are related, with a higher S/CO ratio representing true infection. However, no correlation could be ascertained between a true HCV infection and low S/CO ratio. Furthermore, anti-HCV results have many false-positive factors. It is difficult to differentiate false-positive from positive anti-HCV results using the S/CO ratio alone. Some biochemical tests (e.g., alanine aminotransferase, albumin, cholesterol) are helpful in diagnosing HCV infection but are only distinctive in acute HCV infection (data not shown). In some studies, however, there was no difficulty in diagnosing HCV infection despite the permanent discontinuation of RIBA [30]. Our study demonstrated that positive results would not seem to be conclusive of HCV infection without supplemental RIBA testing.
A limitation of our study was the potential selection bias. Our study population was divided into two groups. One group consisted of hospital patients who were tested by CMIA, and the other group comprised subjects who underwent medical checkup by CIA. Because the performances of the two IA are different, the detection rate of anti-HCV-positive samples may be different in the two groups. However, we tried to analyze as many anti-HCV-positive samples as possible, and the detected anti-HCV-positive samples were independently analyzed by CMIA and CIA.
In conclusion, it is not yet possible to conclusively determine HCV infection (active or resolved) through NAAT or by adjusting the S/CO ratio. Furthermore, it is challenging to propose a standard S/CO ratio, because the performance of each IA in terms of S/CO ratio varies across manufacturers [151718,
21]. However, this study is significant because it sought to elucidate the role of the S/CO ratio by referring to the NAAT, RIBA, and medical records to determine as many true positives as possible from anti-HCV-positive results using one or two IAs.

 XML Download
XML Download