

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The number of Koreans with cardiovascular disease is increasing because of rapid aging and sociocultural changes such as a Westernized diet. In particular, the number of patients with acute myocardial infarction (MI) has steadily increased by approximately 30% over the past five years. This has led to a gradual increase in the economic burden and total cost of medical care benefits for patients with this disease [1].
Platelets play an important role in maintaining normal hemostasis via various mechanisms. Malfunction of these mechanisms can result in the formation of pathologic thrombi and cause vascular occlusion, leading to cardiovascular disease and ischemic stroke [2]. Clopidogrel, one of the most commonly used anti-platelet agents in cardiovascular disease, irreversibly inhibits ADP binding to platelet purinergic receptor P2Y12 [3]. The use of clopidogrel with acetylsalicylic acid is considered a primary therapeutic option for managing patients with recent-onset acute coronary syndrome (ACS) [45].
However, several studies have reported variable responses to clopidogrel in patients with cardiovascular disease [678]. Despite appropriate medical treatment with clopidogrel, major adverse cardiac events (MACEs) occur in some patients. This inter-individual response variability is often referred to as clopidogrel resistance [9]. The incidence of MACEs is higher in patients with a lower response to clopidogrel than in patients with a normal or higher response to clopidogrel [10].
Several methods are used to measure platelet function, including ADP-induced light transmittance aggregometry, the VerifyNow P2Y12 assay, Plateletworks, Multiplate analyzer, and the VASP assay; each method measures platelet activity using different properties [1112]. The platelet function analyzer (PFA)-200 test (INNOVANCE PFA-200 System; Siemens Healthcare, Munich, Germany) is used to evaluate platelet P2Y12 receptor blockade in patients treated with a P2Y-receptor antagonist [13]. The PFA-200 test involves an easy automated process that requires a short time to obtain the test results. As it is a high-shear system using whole blood instead of platelet-rich plasma, it mimics the characteristics of physiological platelet function [14]. However, only a limited number of studies have used the PFA-200 P2Y test to measure the effects of clopidogrel. In particular, no study has examined the relationship between the PFA-200 P2Y results and MACEs.
We therefore analyzed the relationship between PFA-200 P2Y results and the occurrence of MACEs, including cardiac death, MI, restenosis, and ischemic stroke. We also investigated the use of PFA-200 P2Y results as a predictor for MACE risk in patients treated with clopidogrel.
METHODS
1. Study population and patient characteristics
Consecutive patients diagnosed as having ACS in Dong-A University Hospital, Busan, Korea, between August 2013 and June 2016 were prospectively recruited. The inclusion criterion for this study was a diagnosis of ACS, defined as ST elevation MI, non-ST elevation MI, and unstable angina. Patients with active bleeding, hemodynamic instability, or contraindications for antiplatelet agents were excluded. All 106 patients received percutaneous coronary intervention (PCI) using a loading dose of 300–600 mg clopidogrel. Patients who had not taken clopidogrel or aspirin were administered a loading dose of 600 mg clopidogrel and 300 mg aspirin. Patients who had taken 75 mg clopidogrel and 100 mg aspirin for longer than five days were administered a loading dose of 300 mg clopidogrel. For all patients, the loading dose was administered at least four hours prior to PCI, followed by a maintenance dose of 75 mg clopidogrel. We obtained data on baseline characteristics, including age, sex, body mass index (BMI), underlying diseases (diabetes mellitus [DM], hypertension, dyslipidemia, and chronic kidney disease [CKD]), medical history (previous cerebrovascular accidents, PCI, coronary artery bypass grafting, and MI), lifestyle (current alcohol consumption and current smoking status), and other administered drugs. Once platelet function tests were performed, the various MACEs that occurred during the follow-up period were investigated. Clinical data were obtained from medical records. This study was approved by the Institutional Review Board of Dong-A University Hospital. Informed consent was obtained from patients prior to the collection of blood samples.
2. Platelet function test
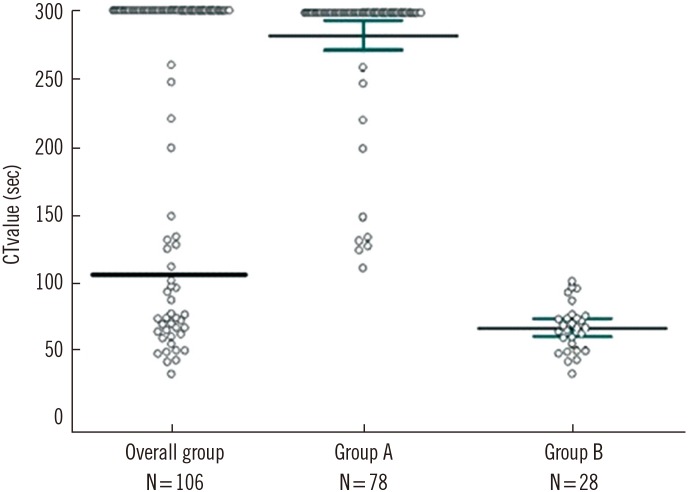
Blood samples were obtained at least four hrs after the administration of a loading dose of 300–600 mg clopidogrel. Blood sampling was carried out using 21-gauge needles and vacuum tubes containing 3.2% sodium citrate. The collection tubes were properly mixed by gently inverting them three or four times, and 800 µL of each blood sample was pipetted into the opening of the test cartridge. Platelet response to clopidogrel was evaluated using the PFA-200 P2Y test, performed within two hrs of blood sampling. The test measured the closure time (CT; second): the time required for the generated platelet plug to completely occlude the central aperture. The maximum measurable CT value was 300 seconds. The cut-off value was determined as 106 seconds, according to the manufacturer's instructions [15]. Patients were divided into Group A (N=78; CT value>106 seconds) and Group B (N=28; CT value ≤106 seconds).
3. Statistical analysis
Statistical analysis was performed using MedCalc for Windows, version 12.7.0.0 (MedCalc Software, Mariakerke, Belgium). P<0.05 was considered statistically significant. Normally distributed data were expressed as mean±standard deviation or number with percentage. The χ2 test and Fisher's exact test were used to compare baseline characteristics between the two groups. For normally distributed continuous variables, the independent t-test was used. The starting point of time-to-event analysis was the date of PCI with a loading dose of clopidogrel. The end point was the date of MACE occurrence, termination of follow-up, or discontinuation of clopidogrel. The remaining patients were designated as event-free. Time-to-event outcomes were analyzed using the Kaplan-Meier method, and relative risk for Group B was estimated with confidence interval (CI). Predictors of MACEs (including CT values) were determined using Cox proportional hazards regression analysis and logistic regression analysis. Cox proportional hazards regression analysis was conducted using the following variables: PFA-200 P2Y results, BMI, underlying diseases, medical history, and lifestyle. Variables were included in the multivariate analysis, if their univariate analysis P was <0.20. The analyses were based on the assumption that the hazard ratios for variables were proportional over time.
RESULTS
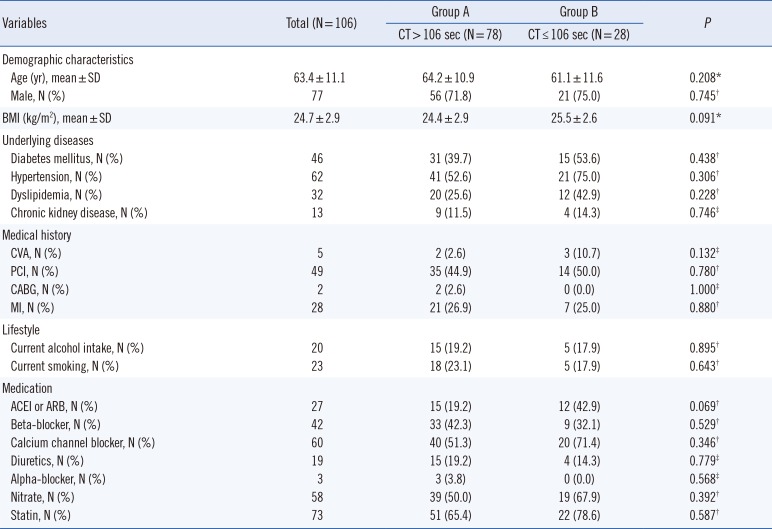
Baseline characteristics did not significantly differ between the two groups (Table 1). In Group A, the CT values of 68 patients were over the measurable upper limit of 300 seconds, while that of the other 10 patients were within the measurable range (171.5±55.3 seconds). The mean CT value of Group B was 68.9±17.5 seconds (Fig. 1).
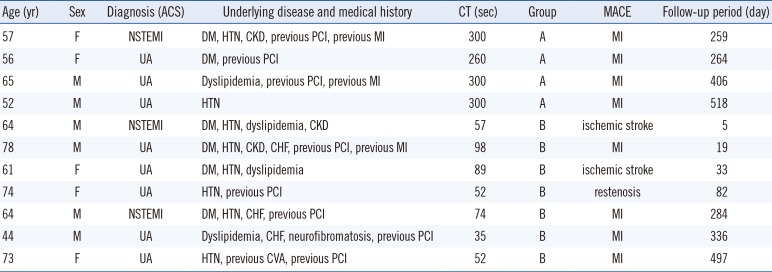
During this study, MACEs occurred in 11 (four Group A and seven Group B) patients (Table 2). The remaining patients were event-free at the time of analysis. The median follow-up period of the 106 patients was 493 days (range: five days to three years). The MACE incidence rate was higher in Group B (25.0%) than in Group A (5.1%; P=0.009). During the follow-up period, two patients were transferred to other hospitals and another two patients expired from other causes (non-small cell lung cancer and biliary sepsis). A total of 16 patients discontinued clopidogrel treatment. Mild bleeding occurred in seven patients of Group A, while there were no bleeding complications in Group B. These seven patients complained of episodic easy bruising or brief localized bleeding. Their mean CT value was 300 seconds (Table 2).
Time-to-event analysis using the Kaplan-Meier method showed a difference between the two groups (P<0.001). The estimated relative risk for Group B was 6.65 (95% CI: 1.55–28.48). The Kaplan-Meier cumulative event-free curves for the two groups are shown in Fig. 2.
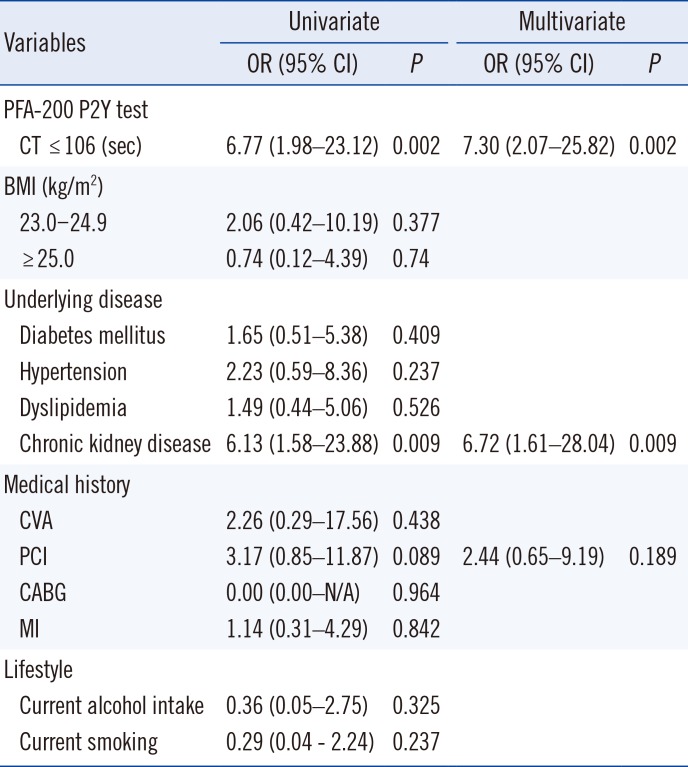
The analysis showed that the significant covariates were CT value and presence of CKD. In the multivariate regression analysis, other factors had relatively low odd ratios. Results of the Cox proportional hazards regression analysis using the enter method are summarized in Table 3.
DISCUSSION
We evaluated response to clopidogrel, using the PFA-200 test. Many clinical factors could lead to a suboptimal response to clopidogrel. Baseline platelet reactivity can increase under specific conditions such as ACS, high BMI, and DM, in particular, type 1 DM [16171819]. Individual differences in clopidogrel uptake rate and the degree of conversion into active metabolites can cause response variability to clopidogrel [20]. Drug interactions are also important factors to consider. A number of studies have reported that clopidogrel-induced anti-platelet effects are hindered by lipid-soluble statins, which depend on CYP3A4-mediated metabolism [2122]. Other studies, however, have indicated that lipid-soluble statins do not negatively correlate with the anti-platelet effects of clopidogrel [23].
Response variability to clopidogrel is clinically significant. Its underlying mechanisms have not yet been fully elucidated [9], but are likely to be multifactorial. Hence, it is necessary to investigate whether patient baseline characteristics could have affected the present results. We found no statistically significant differences between the two groups for all baseline characteristics.
We demonstrate that a CT value <106 seconds was a strong predictor of MACE occurrence. Furthermore, CT value was a stronger predictor of MACE occurrence than other factors such as BMI, underlying diseases (DM, hypertension, dyslipidemia, and CKD), medical history (previous cerebrovascular accidents, PCI, coronary artery bypass grafting, and MI), and lifestyle (current alcohol intake and current smoking). Among the latter factors, only CKD was associated with a higher risk of MACEs. CKD had a 6.13- and 6.72-fold adjusted MACE occurrence risk in our univariate and multivariate analyses, respectively, consistent with previous studies [24]. Reduced glomerular filtration rate is also associated with increased coagulability, arterial stiffness, and abnormal levels of apolipoprotein, homocysteine, and fibrinogen [252627]. These mechanisms might influence the increased risk of MACEs.
We demonstrated that MACE incidence is increased in patients with a relatively low response to clopidogrel, compared with patients with a normal or high response to clopidogrel, because of platelet P2Y12 receptor blockade. Thus, PFA-200 P2Y results could be used as a predictive marker of MACE risk in patients treated with clopidogrel. In addition, patients with a relatively high response to clopidogrel might have a higher incidence of bleeding, although the number of patients with bleeding was not significant in our study.
The present study has some methodological limitations. The first is the small number of subjects, all of whom were recruited from a single hospital; this could have introduced selection bias. Further studies with larger populations are needed to confirm our findings. In addition, although the term “MACE” has been used to evaluate short- and long-term outcomes in many previous studies, it has no standard definition [28]. The various components of MACEs should be evaluated in more comprehensive studies with larger samples.
We also did not compare genetic background between the two groups. Various genetic polymorphisms influence the degree of drug-induced platelet inhibition [2930]. Polymorphisms of the CYP2C19 gene, especially CYP2C19*2, could cause low active clopidogrel metabolite levels and might be associated with a low response to clopidogrel [3132]. Several studies have reported a correlation between polymorphisms of the CYP2C19 gene and risk of MACEs in patients treated with clopidogrel [333435]. Future studies should also evaluate genetic background.
The PFA-200 test was not performed during the follow-up period; thus, it is also necessary to determine whether the degree of platelet P2Y12 receptor blockade is maintained at a similar level over time. In addition, the PFA-200 P2Y results have a measurable upper limit of 300 seconds; the results of 68 patients exceeded the measurable upper limit. Because of this analyzer limitation, it is difficult to proportionally correlate test results and clinical outcomes, including MACEs and bleeding tendencies.
Thus, although the PFA-200 test could be used to predict therapeutic response at the start of anti-platelet therapy with clopidogrel, because of the above limitations, the results of a single platelet function test might not justify treatment modification. More studies are needed to provide appropriate strategies for anti-platelet therapy for patients.

 XML Download
XML Download