

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Extra-abdominal desmoid tumors are rare benign lesions. They can, however, markedly grow and invade into the surrounding tissues. They may require multiple and debilitating surgical interventions for local control, resulting in significant surgery-related morbidity and occasionally even loss of the affected limb. Even though surgery has until recently remained the primary treatment modality for desmoid tumors, alternative attempts have been introduced because disfigurement and/or functional impairment resulting from a wide resection may be unacceptable.1) In addition, high recurrence rates even with a wide resection ranging from 30% to 40% have necessitated the development of alternative treatment modalities including chemotherapy,23) radiotherapy,456) antiestrogen agents,78) interferon,910) tyrosine kinase inhibitors,1112) colchicine,13) and nonsteroidal anti-inflammatory drugs (NSAIDs).11415)
Amongst the alternative treatment options, NSAIDs would be attractive considering its efficacy on desmoid tumors reported in the literature and its well-tolerated minimal adverse effects profile. The use of NSAIDs for this benign but aggressive lesion was based on a case report of regression of a sternal desmoid tumor during indomethacin treatment of pericarditis.15) Following on from that various NSAIDs or composites with tamoxifen,16) testolactone,17) warfarin and vitamin K17) have been tested in nonrandomized retrospective studies or presented as part of either case reports or series; the response to such treatment, described as either partial or complete response, ranged from 50% to 100%. Even though most reports of NSAIDs in desmoid tumors have shown promising results, controlled trial data are lacking and the clinical benefit of NSAID treatment remains unproven. The efficacy and mechanism of action have not been fully established, and many authors doubt that the result is solely attributable to the NSAID itself. Recently, some investigators have tried to elucidate the natural course of extra-abdominal desmoid tumors; they reported the ability of these tumors to stabilize or regress spontaneously and insisted that the wait-and-see policy is a valid management strategy.1819202122)
In this study, we retrospectively reviewed the outcomes of patients who had been treated with the NSAID meloxicam for extra-abdominal desmoid tumors and evaluated the correlation between the clinical outcome and clinicopathological variables including cyclooxygenase-2 (COX-2) expression in the tumor specimen as determined by immunohistochemistry. We hypothesized that COX-2 expression in the specimen would be directly related to the response to NSAID treatment, assuming that the treatment effect would be attributable to the COX-2 inhibitory action of NSAIDs. In addition, the clinical outcomes of this study were compared to previous literature reports of the wait-and-see strategy. This study was approved by the Institutional Review Board of Seoul National University Bundang Hospital (IRB No. B-1506-304-106).
METHODS
Extra-abdominal Desmoid Tumors in Our Hospital and Meloxicam Treatment
We retrospectively reviewed 27 patients who had been treated for extra-abdominal desmoid tumors by either surgery or meloxicam between September 2009 and September 2013. There were 11 men and 16 women with a mean age of 37.2 years (range, 16 to 66 years). Eight lesions were located in the upper extremities, seven were in the lower extremities, and 12 were in the trunk. The mean tumor diameter was 5.8 cm (range, 1.8 to 11.2 cm). Nineteen patients presented with a primary tumor and eight had a recurrent lesion. For the 19 primary cases, biopsy prior to treatment confirmed the diagnosis. All 27 patients underwent sigmoidoscopy to rule out familial adenomatous polyposis and none of them showed any evidence of polyposis. Meloxicam was prescribed for small lesions that would be resectable without functional impairment, with patients kept under close surveillance for potential growth. In addition, meloxicam was considered as the initial treatment in cases where surgery was not feasible without sacrificing vital neurovascular structures. A medical history of gastrointestinal illness or previous alternative systemic treatments for the lesion was a contraindication for the meloxicam trial.
Of 27 patients, 10 underwent surgery and 17 were given meloxicam as their initial treatment. Of 10 patients in the surgery group, four had recurrence. Three of them were then included in the meloxicam treatment group. Meloxicam was given to a total 20 patients: 17 for primary lesions; three for recurrent lesions following surgery performed in our hospital. Eight were male and 12 were female in the meloxicam group. Their mean age was 36.1 years (range, 16 to 64 years). Meloxicam was planned to be administered orally at a dose of 15 mg/day for 6 months. Cessation of medication was determined when (1) complications of NSAID developed, including gastrointestinal symptoms, cardiovascular problems, elevation of liver enzymes and face edema; (2) there was disease progression; or (3) the medication treatment course was complete. The mean duration of follow-up was 25.8 months (range, 3 to 64 months) for meloxicam treatment.
Evaluation of Response to Meloxicam
Twenty patients who were treated with meloxicam were followed up with laboratory tests for hepatic and renal function every month. At each visit, they were clinically assessed with either magnetic resonance imaging or sonography performed every 3 to 6 months. The efficacy of meloxicam treatment was evaluated twofold. First, the tumors were classified according to Response Evaluation Criteria in Solid Tumors (RECIST) guidelines:23) tumor progression (PD) was defined as an increase of > 20% in the initial largest tumor diameter; complete response (CR), as disappearance of the lesion; partial response (PR), as a decrease of > 20% in the initial largest tumor diameter; and stable disease (SD), as a small change that does not meet any criteria. Second, the cumulative probability of dropping out from our conservative strategy during or after meloxicam treatment was estimated in a competing risk setting.24) Patients in whom the tumor had increased in size were considered to have a failure of the meloxicam treatment and dropout. Patients who had not completed the full course of meloxicam treatment were not considered dropouts if they showed no evidence of disease progression.
Correlation between Response to Meloxicam and Clinicopathological Variables
Twenty patients were divided into two groups according to clinical response to meloxicam treatment based on the RECIST criteria: nonprogressive group (CR, PR, and SD) vs. progressive group (PD). Correlations between clinical outcome and clinicopathological variables including sex, age, location of tumor, tumor size, presentation (primary vs. recurrent), and COX-2 expression, were assessed by the Fisher exact test. All reported p-values were two-tailed. All specimens were subjected to immunohistochemical study for COX-2 expression using biopsy samples by the conventional streptavidin-biotin complex technique on the formalin-fixed paraffin-embedded sections. A musculoskeletal pathologist without knowledge of the clinical information (HJP) was employed to evaluate the result of immunohistochemical staining.
Literature Review Reporting the Results of Wait-and-See Policy
A comprehensive review of the literature was performed by a search of PubMed using the terms, “extra-abdominal,” “desmoid tumors,” “aggressive fibromatosis,” “observation,” and “wait-and-see.” We excluded manuscripts that (1) included abdominal desmoid cases, (2) were from the same hospital with overlapping time periods, (3) and reported less than 10 cases; ultimately, data on 208 patients from five articles were available for review.1819202122) When articles from the same hospital with overlapping periods were noted, the most recent data was included.
Go to : 
RESULTS
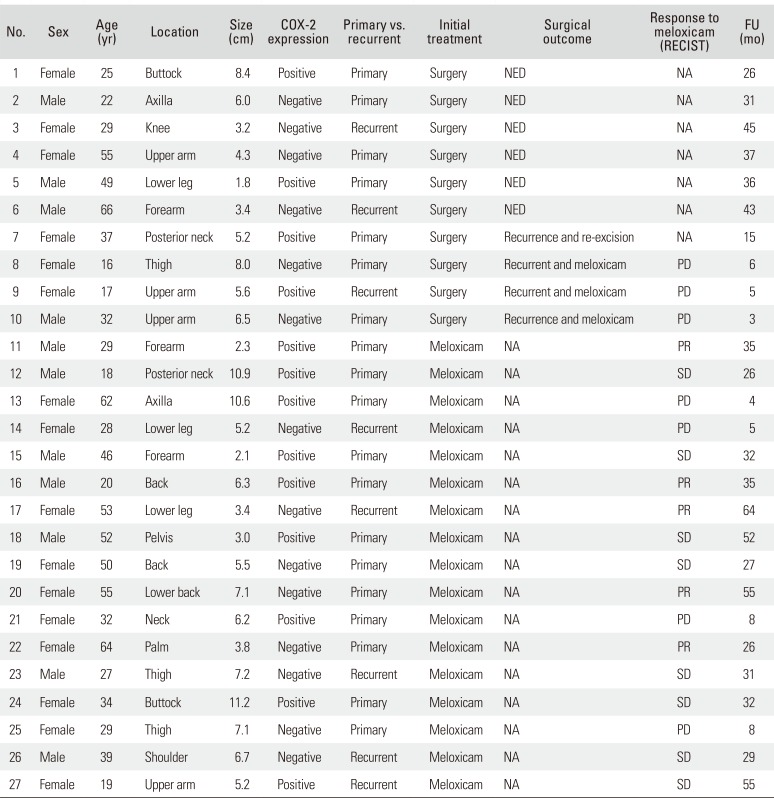
Characteristics of the 27 patients are summarized in Table 1, and allocation of the patients with treatment results are shown in Fig. 1.
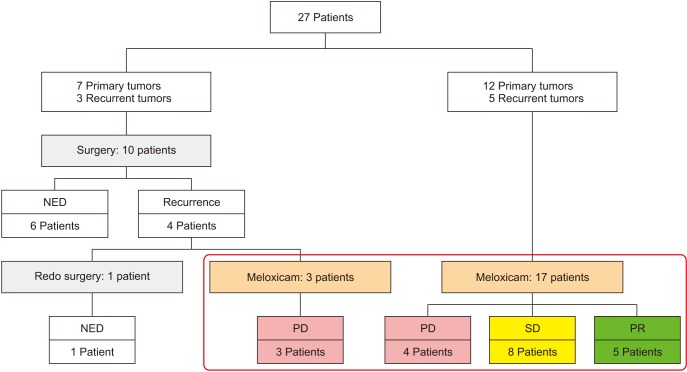 | Fig. 1Allocation of patients and treatment results according to Response Evaluation Criteria in Solid Tumors criteria. NED: no evidence of disease, PD: progressive disease, SD: stable disease, PR: partial response.
|
Table 1
Patient Characteristics
![]()
Surgical Treatment
All surgeries aimed to obtain a wide margin. Of the ten patients who underwent surgery as initial treatment, six had no recurrence until the latest follow-up at a mean of 36.3 months (range, 26 to 45 months) after surgery. Four patients had recurrence at a mean follow-up of 8 months (range, 6 to 15 months). For the recurred lesions, one patient underwent re-excision and had no further recurrence. The remaining three patients were given meloxicam.
Clinical Outcomes of Meloxicam Treatment and Correlation with Clinicopathological Variables
Meloxicam was given to 20 patients in our series. Seventeen patients were given it as an initial treatment and three were for recurrent disease following surgery. Sixteen patients completed the full planned course of meloxicam, whilst four patients ceased due to progression of disease during the course of treatment. No patient abandoned meloxicam due to adverse effects of the medication.
Of the 20 patients evaluated, according to the RECIST criteria, there were five patients with PR (25.0%) (Fig. 2), eight with SD (40.0%), and seven with PD (35.0%). No patient showed complete remission of disease at the last follow-up. Thirteen of the 20 patients (65.0%) had a status of SD or better. Six of seven patients with PD underwent surgical management. The lesion of the remaining one patient (patient no. 21) was deemed inoperable because of proximity to the brachial plexus, the axillary vessels, the lung, and cervical spines. The patient was recommended systemic chemotherapy but was lost to follow up.
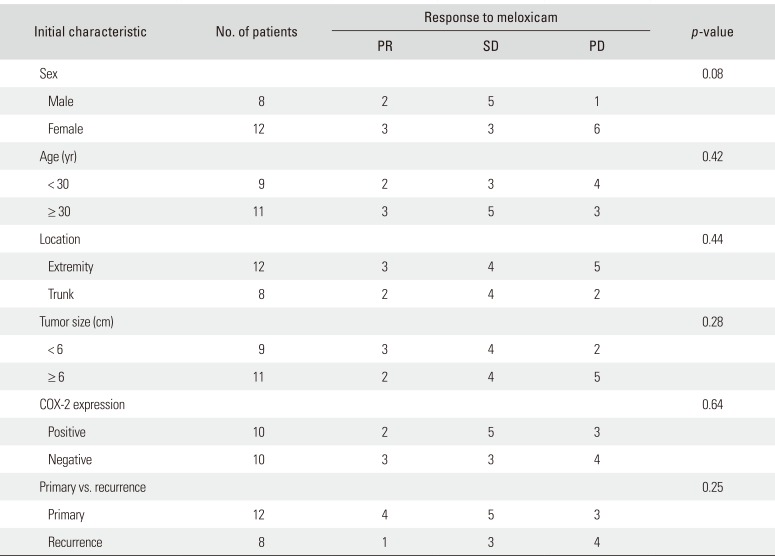
With regards to clinical variables including sex, age, location of tumor, tumor size, and presentation (primary vs. recurrent) before meloxicam treatment, none showed a statistically significant correlation with clinical outcomes (Table 2). As for COX-2 expression, immunohistochemistry demonstrated positive staining in 10 patients (50%). COX-2 expression was not a significant prognostic factor for response to meloxicam by the Fisher exact test. Of the 10 patients with positive staining for COX-2, seven had nonprogressive disease, while six out of 10 patients did in the negative staining group (Fig. 3).
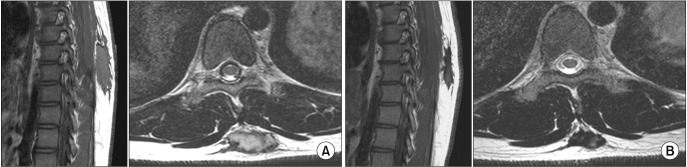
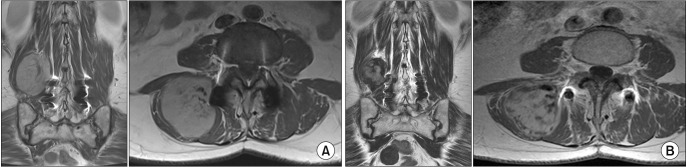 | Fig. 3A patient (no. 20) with desmoid tumor in the right paraspinal muscles (A) showed tumor shrinkage in follow-up magnetic resonance imaging (B). Immunohistochemistry of the specimen demonstrated negative cyclooxygenase-2 staining.
|
Table 2
Correlation between Clinicopathological Variables and Clinical Outcomes
![]()
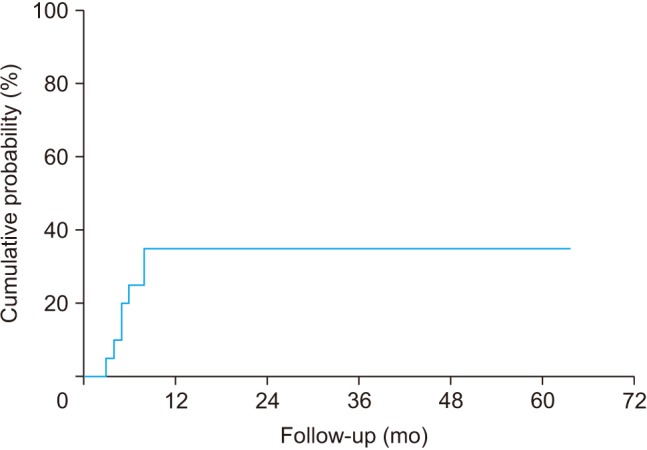
The cumulative probability of dropping out from our nonoperative strategy using meloxicam was 35.0% at 1 year, which remained unchanged at 5 years (Fig. 4). When stratified according to COX-2 expression, the probabilities were 30.0% at 1 and 5 years in the COX-2 positive group and 40.0 % at 1 and 5 years in the COX-2 negative group. There was no significant difference between the groups. All drop-outs occurred within 1 year of follow-up.
Literature Review Reporting the Results of Wait-and-See Policy
Five studies have reported various rates of spontaneous interruption of tumor growth ranging from 65.1% to 96.1% (Table 3).1819202122) Of the 208 subjects from the five articles, 17 (8.2%) showed spontaneous regression of tumor, 150 (72.1%) were stabilized, and 41 (19.7%) demonstrated progression of disease. A study of a series of 55 patients by Briand et al.19) showed that the cumulative probability of dropping out from the wait-and-see policy was only 5.7% at 1 year and 9.6% at 5 years.
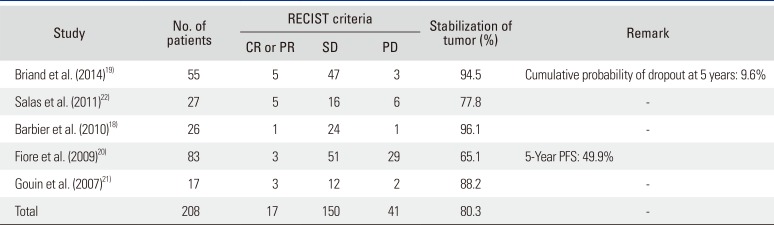
Table 3
Review of Literatures Reporting Results of Wait-and-See Strategy for Desmoid Tumors
| Study | No. of patients | RECIST criteria | Stabilization of tumor (%) | Remark | ||
|---|---|---|---|---|---|---|
| CR or PR | SD | PD | ||||
| Briand et al. (2014)19) | 55 | 5 | 47 | 3 | 94.5 | Cumulative probability of dropout at 5 years: 9.6% |
| Salas et al. (2011)22) | 27 | 5 | 16 | 6 | 77.8 | - |
| Barbier et al. (2010)18) | 26 | 1 | 24 | 1 | 96.1 | - |
| Fiore et al. (2009)20) | 83 | 3 | 51 | 29 | 65.1 | 5-Year PFS: 49.9% |
| Gouin et al. (2007)21) | 17 | 3 | 12 | 2 | 88.2 | - |
| Total | 208 | 17 | 150 | 41 | 80.3 | - |
![]()
Go to :
DISCUSSION
A desmoid tumor is a nonmalignant and seldom-fatal, but locally invasive disease. Surgery has been considered the standard treatment even with high recurrence rates ranging from 30% to 40%; because desmoid tumors can extend into muscular fibers, it is difficult to obtain a “clear margin.”25) As an alternative, some authors have reported the usage and efficacy of NSAIDs in the treatment of desmoid tumors. In this study, we assessed the outcome of meloxicam treatment for extra-abdominal desmoid tumors and the correlation with clinicopathological variables including COX-2 expression in tumor specimens.
In many studies, NSAIDs exhibited anticancer activities in a variety of malignancies including colorectal, breast, prostate and pancreatic cancers.26) With regards to desmoid tumors, the usage of various NSAIDs has been reported since regression of a sternal desmoid tumor was noted with in indomethacin treatment of pericarditis.15) However, the efficacy of NSAIDs for desmoid tumors has largely been demonstrated only in patients with intra-abdominal disease when used in combination with cytotoxic or antihormonal agents until a recent study by Nishida et al.1) They reported excellent outcome of sole meloxicam administration in patients with extra-abdominal desmoid tumors with 95% of them achieving SD or better. The authors, therefore, recommended meloxicam as the initial treatment for patients with extra-abdominal desmoid tumors. In a study using celecoxib in combination with tamoxifen for 16 patients with extra-abdominal desmoid tumors, six had growth stabilization, one had a 50% reduction in the size of the tumor, there was one complete regression, and eight progressed.27) Of the patients who had resectable disease, surgery was avoided in 30%.
Anticancer activity by NSAIDs is assumed to be associated with the COX-dependent pathway. COX-2 has been demonstrated to play an important role in the growth of desmoid tumors: pharmacological blockade of the COX pathway resulted in the decrease of cell proliferation in the in vitro desmoid cell cultures.28) We hypothesized that COX-2 expression in tumor specimen would lead to a good response to NSAID treatment, expecting that the suppressive effect on tumor growth would be attributable to the COX-2 inhibitory action of NSAIDs. However, in the present study, we failed to demonstrate a statistically significant correlation between the COX-2 expression and clinical response to meloxicam. Of the 10 patients showing positive staining for COX-2, seven had a nonprogressive disease; six of 10 patients did in the negative staining group. This result could be interpreted as one of three situations: (1) the number of cases in this study might be not enough to show statistical significance; (2) the mechanism of action of meloxicam in the treatment of desmoid tumors might be by a pathway(s) other than COX inhibition; or (3) the clinical outcome might have little to do with NSAID treatment. Recently, some investigators have proposed a wait-and-see policy for the initial management of extra-abdominal desmoid tumors, based on their observation of spontaneous stabilization or regression of this disease. Briand et al.19) noted 85% of patients showed spontaneous arrest of tumor growth over the course of their study and the cumulative probability of dropping out from the wait-and-see policy was only 5.7% at 1 year and 9.6% at 10 years. Their study suggests that desmoid tumors have the ability to stabilize spontaneously in the vast majority of patients. Bonvalot et al.29) compared the outcomes according to treatment modalities. They reported that growth arrest concerned two of three of nonoperatively treated patients and suggested that patients may be managed with a wait-and-see policy because growth arrest is common in desmoid tumors. In the present study, 13 of 20 patients (65.0%) had a nonprogressive tumor with the meloxicam treatment. By indirect comparison using data from literatures, our results using meloxicam seemed to have no advantage over a wait-andsee strategy. To our knowledge, no single study reporting the efficacy of NSAIDs on desmoid tumors has performed comparative analysis with a control group. All of them are case reports or series. Without a control group, it is difficult to assess the treatment effect of NSAIDs. In addition, case reports and series are susceptible to post hoc fallacy that states “since event X was followed by event Y, event Y must have been caused by event X.” Studies on NSAID treatment for desmoid tumors may be guilty of this. In the present study, meloxicam intake may have prevented two of three patients from undergoing an operation, although we cannot conjecture what percentage of patients visited clinicians during an involuting phase and in how many patients' meloxicam actually regressed desmoid tumors. In order to prove the sole contribution of NSAID management, a large comparative study with a wait-and-see group will be necessary.
In this study, we were not able to determine that the use of a COX-2 inhibitor has an additional influence on the natural course of desmoid tumors. Nevertheless, the results of the present study suggest that conservative treatment could be a primary treatment option for this perplexing disease. Recently, National Comprehensive Cancer Network guidelines have included observation as an option for the selected patients with resectable tumors.30) Many authors retreat from their initial aggressive approach and begin instituting a conservative strategy as the primary treatment modality. Further studies on prognostic markers are mandatory to predict the efficacy of conservative treatments. In addition, studies involving long-term follow-up of initial good responders to conservative treatment are warranted.
Go to :
 XML Download
XML Download