

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Nerve root compromise can be deemed as the direct cause of radicular pain even though the primary pathology is the intervertebral disc herniation. The disc herniation, being a mechanical lesion, tends to compromise the nerve root.1) In addition, the inflammatory response to the exposed nucleus pulposus also contributes to radicular pain.234) However, some disc herniations do not hinder the nerve root, especially if the herniation is focal and away from the root. Therefore, the amount of nerve root compromise caused by disc herniation may vary depending upon the location of herniation.
The nomenclature versions currently in practice for grading nerve root compromise include the grading systems of Pfirrmann et al.5) and van Rijn et al.6) These systems are well established, proved to be reliable, and periodically used by various authors. Due to its dichotomized nature, the van Rijn's system demonstrates higher reliability; 7) however, we preferred the Pfirrmann's grading for its itemized nature. The orthopaedic residents at our hospital were aware of this grading system. Even though they did not use it regularly, they were comfortable with the system as it was simple and facile. Hence, we decided to quantify the reliability of Pfirrmann's grading among orthopaedic residents at our institute.
METHODS
Fifty consecutive magnetic resonance imaging (MRI) studies that belonged to patients who initially presented with lumbar radiculopathy and were diagnosed to have a single level lumbar disc herniation were selected. We evaluated all the sagittal and axial cut MR images of the affected disc level to select one axial cut MR image that portrays maximal herniation in each patient. Therefore, 50 axial cut MR images were selected, which included images depicting concomitant ligamentum flavum thickening and/or facet hypertrophy. We excluded images portraying far lateral disc herniations, spondylolisthesis, infections and neoplasms at the chosen level.
Pfirrmann's grading is based on the evaluation of an axial cut MR image at the level of maximal disc herniation to grade the unilateral traversing nerve root compromise due to the herniating disc. Pfirrmann et al.5) graded the nerve root compromise into normal (grade 0), contact (grade 1), deviation (grade 2), and compression (grade 3). A calibrating session was held to brief the residents regarding this grading system using Pfirrmann's original work. A set of ten axial cut MR images other than the 50 selected images were chosen for discussion at the calibrating session.
Residents were clearly explained about the normal position of the nerve roots in an axial cut MR image. Concerns were raised about the nerve roots being nonvisible in certain MR images. In addition, there was also a concern about images portraying a broad-based disc herniation causing bilateral nerve root compromise where the contralateral nerve root cannot be used as a reference to differentiate contact (grade 1) or deviation (grade 2). In such circumstances, we instructed the residents to assume the position of the nerve root with their understanding about its normal location and the four described grades in the Pfirrmann's grading system.
Accordingly, each resident had to grade the 50 MR images for which, they were not put under any obligation regarding time, mainly to reduce instances of fatigue and to maintain the precision of their ratings. Once they were ready with their responses, they were asked to recheck under supervision. Their responses to each MR image as grade 0, 1, 2 and 3 were considered as categorical variables. Interrater reliability of the grading system was determined by calculating the Fleiss' kappa coefficient. The same MR images were shuffled and provided to one of the residents for reassessment after a month and the response was collected. This data was used to determine the intrarater reliability by calculating the Cohen's kappa coefficient.
Statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA) and Graph Pad Prism 5.0 (GraphPad Software Inc., San Diego, CA, USA). Reliability was assessed by calculating percentage agreement and also the kappa statistic. We interpreted the values of kappa as per the recommendation of Landis and Koch;8) according to them, a kappa value of 0–0.20 indicates slight agreement, 0.21–0.40 indicates fair agreement, 0.41–0.60 indicates moderate agreement, 0.61–0.80 indicates substantial agreement, 0.81 or higher indicates excellent agreement, and 1.00 indicates absolute agreement. Informed consent was obtained from all patients to use their MR images for research purposes without revealing identity and the study was performed abiding by all ethical considerations.
Go to : 
RESULTS
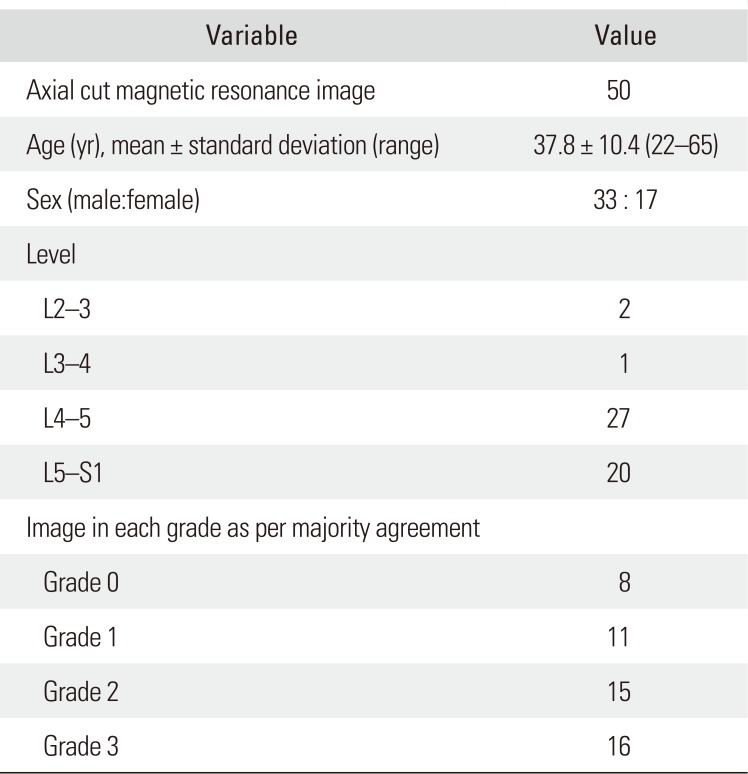
Consecutive MRI studies of different patients (n = 50; male, 33; female, 17; age, 37.8 ± 10.4 years) were selected. The selected images were predominantly the axial cuts of the affected L4–5 and L5–S1 disc levels depicting maximal herniation; apart from which, there was only one L3–4 and two L2–3 disc levels chosen (Table 1). Images were distributed to five orthopaedic residents and their grading for each image was received within a week. The grade on which the majority of the residents had agreement for a particular image was considered as the actual grade. In this way, our selected images included all four grades of nerve root compromise as described in the Pfirrmann's grading system (Fig. 1).
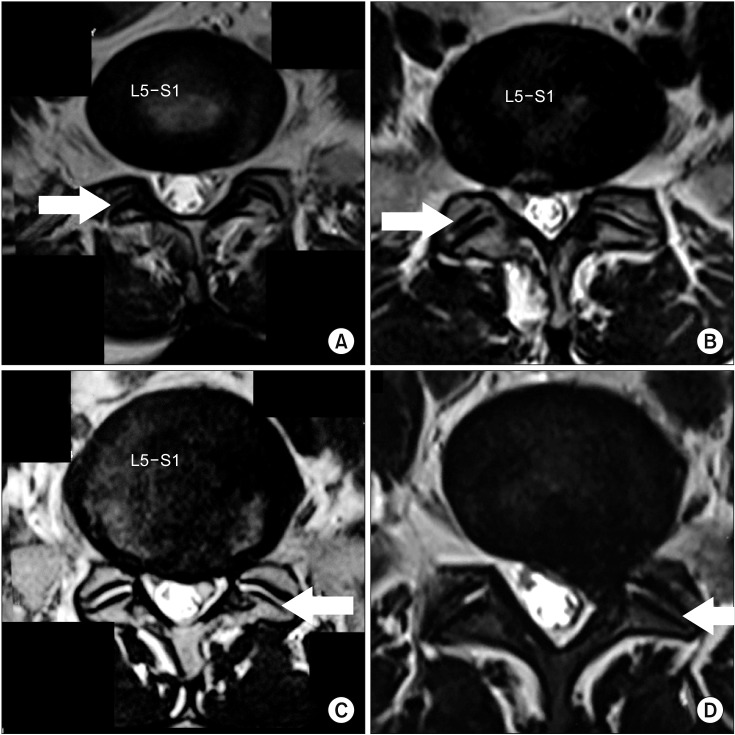 | Fig. 1Axial cut magnetic resonance images at the affected lumbar disc levels of different patients (arrows indicate the side which was graded). (A) Grade 0 (normal), when there is no contact of disc material with the nerve root. (B) Grade 1 (contact), when there is contact of disc material with the nerve root. (C) Grade 2 (deviation), when there is deviation of the nerve root dorsally. (D) Grade 3 (compression), when the nerve root is compressed between the spinal canal wall and the herniated disc.
|
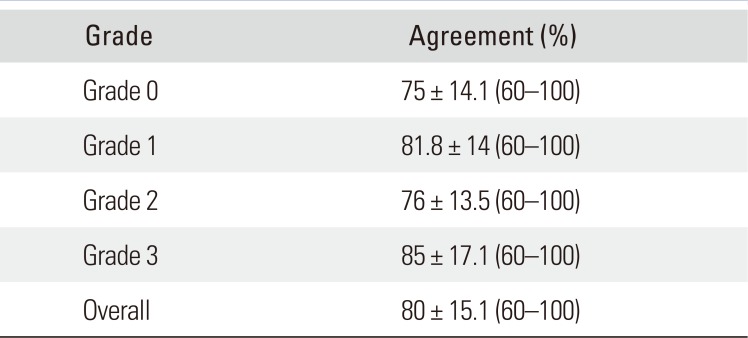
The percentage of agreement for a grade that was given by the majority to each image was calculated. This data was used to calculate the overall percentage of agreement (80% ± 15.1%) and grade-wise percentage of agreement (Table 2). Only for 14 of the selected images, 100% agreement was obtained: eight belonged to grade 3, two belonged to grade 2, three belonged to grade 1, and one belonged to grade 0. Among the remaining images, 22 had 80 % agreement and 14 had 60% agreement.
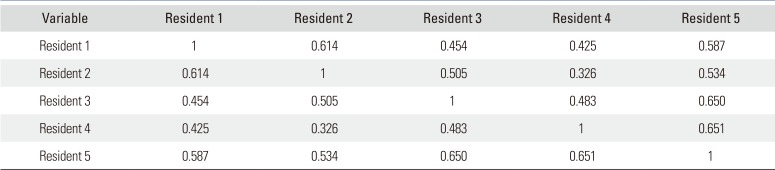
In order to precisely analyse the reliability of this grading system, we calculated the Cohen's kappa between all pairs of residents. This data was used to form the interrater kappa matrix (Table 3). However, the statistical measure for assessing the reliability of agreement between multiple raters is the Fleiss' kappa. We inferred a Fleiss' kappa value of 0.521, which signifies moderate reliability according to the interpretation of kappa by Landis and Koch (Table 4).8) Even though our kappa coefficient is lower and does not replicate Pfirrmann's original work, the reliability still remains moderate as inferred by Pfirrmann et al.5)

Intrarater reliability was calculated using the reassessment data of one of the residents. The chosen resident was consistent with his previous rating for 39 of the images; hence, there was 78% agreement. We calculated the Cohen's kappa between the chosen resident's previous and latest rating; it was found to be 0.696, which signifies substantial agreement according to the interpretation of kappa by Landis and Koch.8) Therefore, we inferred a moderate interrater and substantial intrarater reliability for the Pfirrmann's MR image-based grading of lumbar nerve root compromise.
Go to :
DISCUSSION
Lumbar radiculopathy is the predominant presentation of disc-induced nerve root compromise. A bulging or herniating disc can remain asymptomatic;910) however, radicular pain may develop if there is any hindrance to the nerve root.11) Hindrance to the nerve root happens when there is violation of the nerve root area by the displaced disc. The nerve root can either have a mere contact with the disc material or be pushed aside or compressed. This is the baseline of Pfirrmann's MR image-based grading of nerve root compromise. In addition, understanding the normal location of the traversing nerve roots in an axial cut lumbar disc level MR image is a prerequisite to use this grading system; however, far lateral disc herniations affecting the exiting root are not considered.
Despite not regularly used, Pfirrmann's grading is periodically utilized.121314) The system incorporates four grades: grade 0 is considered as normal even though there can be a focal disc herniation that does not hinder the nerve root; grade 1 (contact) is when the nerve root is in visible contact with the bulging or herniating disc material but remains in its normal location; grade 2 (deviation) is where the nerve root is displaced dorsally; and grade 3 (compression) is when the nerve root is compressed between the disc material and the wall of the spinal canal. Detailed descriptions of the grades are available in Pfirrmann et al.'s original work.5)
It is necessary that the nerve roots be clearly visible in the axial cut MR image; however, it may not be possible all the time. This was discussed in our calibrating session as the residents raised this issue looking at some of the axial cut MR images in which the nerve roots were not clearly visible. Another query that was raised by the residents during the calibrating session was about broad-based disc herniations where there could be bilateral nerve root compromise. The nerve root on one side cannot be taken as a reference to differentiate grade 1 (contact) or grade 2 (deviation) on the other side. In both situations, residents were instructed to assume the location of the nerve root. This assumption is only subjective and could have biased our results.
Once responses were received, reliability was calculated using percentage statistics and kappa statistic. After proposal of this grading system by Pfirrmann et al.5) in 2004, its reliability was rechecked by Lurie et al.15) in 2008. Pfirrmann et al. reported an interobserver kappa of 0.62–0.67; however, Lurie et al. inferred a comparatively low interobserver kappa of only 0.47. Even so, both kappa values can be interpreted as moderate reliability as per the kappa interpretation of Landis and Koch.8) Similarly, our interobserver Fleiss' kappa value was 0.521 signifying moderate reliability. In addition to interrater reliability, we calculated the intrarater reliability for one of the residents and inferred substantial agreement. This proves that the grading remains consistent.
It should be known that the raters who gave their responses were junior orthopaedic residents and not specialists in this field. Their individual understanding of this grading system may vary. Apart from this, spinal canal stenosis due to hypertrophied facets or a thickened ligamentum flavum could have mislead the assumption of the probable location of a compromised nerve root whenever it was not visible. These factors could have influenced our results; however, if appropriate rules are framed to interpret such MR images, the reliability of this grading system will grow higher and adopting it in day-to-day practice will become feasible.
In conclusion, 50 axial cut MR images at the affected lumbar disc levels were chosen and given to five orthopaedic residents for grading according to the Pfirrmann's MR image-based grading of lumbar nerve root compromise. Responses were received in the form of categorical variables and reliability analysis was done. We inferred moderate interrater and substantial intrarater reliability for this grading system. Moreover, our residents took only a short time to learn and reproduce this grading system as ratings that proved to be reliable and consistent. Therefore, our results prove that the Pfirrmann's MR image-based grading of lumbar nerve root compromise is a valid measure of the radiological severity of nerve root compromise due to the herniated intervertebral disc.
Go to :
 XML Download
XML Download