

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Among the diseases causing acute neck pain, longus colli calcific tendinitis (LCCT; “retropharyngeal calcific tendinitis” or “prevertebral calcific tendinitis”) is a disease that should not be overlooked. LCCT is a disease in which calcium hydroxyapatite crystal deposits from in the superior oblique tendon fibers of the longus colli muscle, like calcific tendinitis of the shoulder and hip joints.12) The pathogenesis was first clarified by Ring et al.3) in 1994; an inflammatory reaction secondary to calcium deposition induces symptoms of LCCT such as severe neck pain, limited neck movement and odynophagia.4) Since it is a rare disease, only several case reports have been published,23567) and detailed analysis of the clinical features of the disease is still missing. In this regard, we analyzed clinical and imaging data of 10 patients with LCCT for better understanding of the features of the disease.
METHODS
Patients and Data Collection
This is a retrospective review of clinical records and radiographic findings. Between January 2015 and June 2017, 10 patients who were treated for LCCT at our spine center were enrolled. Clinical data included medical history, symptoms, duration of symptoms before treatment and treatment period. In addition, we reviewed the routes of patient visits and whether the patients had previously visited other hospitals. All patients were hospitalized and treated with medical treatment consisting of intravenous (IV) injection of methylprednisolone 125 mg twice and oral nonsteroidal anti-inflammatory drugs (NSAIDs) administration. All patients discharged after symptomatic improvement to the extent that daily life was possible. Laboratory data include C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and white blood cell count. All patients underwent cervical simple radiography and the retropharyngeal space was measured at C3 level on the lateral image. Computed tomography (CT) scans were used to confirm the presence and location of calcification and further characterize the appearance of calcific deposit. Magnetic resonance imaging (MRI) was performed to differentiate from other diseases such as retropharyngeal abscess. We conducted this study in compliance with the principles of the Declaration of Helsinki. The protocol of this study was reviewed and approved by the Institutional Review Board of Pohang Semyeong Christianity Hospital (IRB No. PSMCHIRB-17-05). Informed consent was waived.
RESULTS
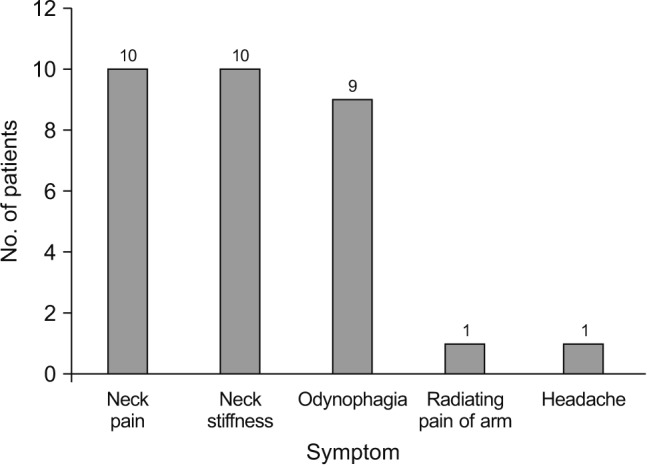
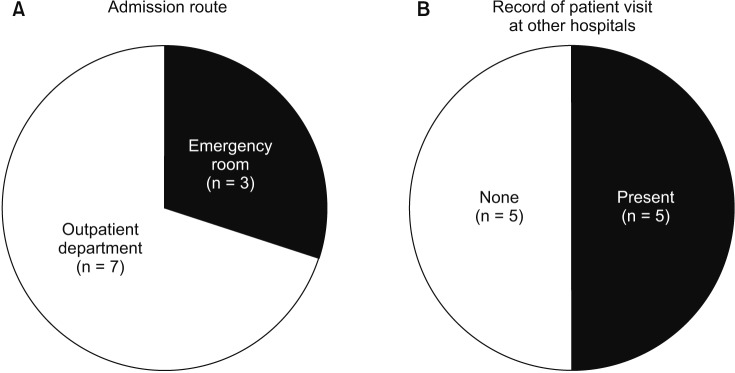
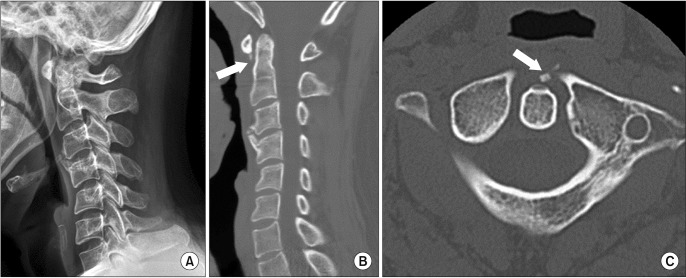
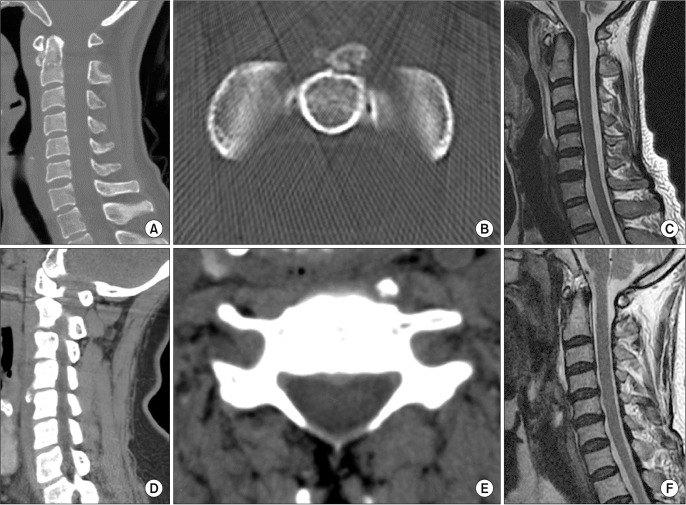
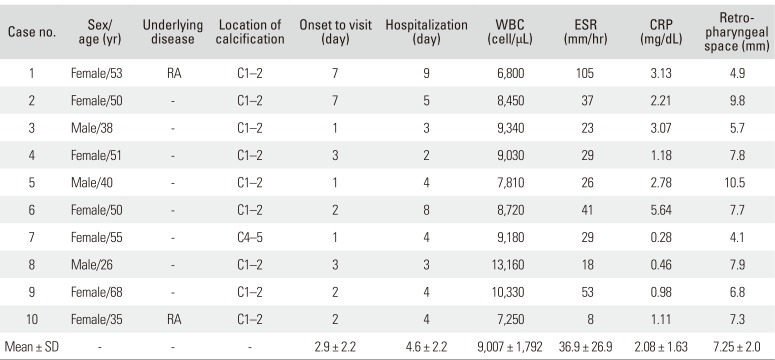
The mean age of the patients was 46.6 years (range, 26 to 68 years), and there were three males and seven females. Except for two cases of rheumatoid arthritis (RA), there was no other underlying disease and trauma history. All 10 patients complained of severe posterior neck pain and neck stiffness. Odynophagia was presented in nine patients. Other symptoms included one case of trapezial radiating pain and headache, each (Fig. 1). Fever was not associated present in all patients. The mean time from symptom onset to hospital visit was 2.9 days. The shortest period was 1 day and the longest period was 7 days. All of the patients visited the hospital in acute phase. The mean hospitalization period was 4.6 days. Of the 10 patients, three patients were admitted through the emergency room, and the rest were admitted through outpatient clinics (Fig. 2A). There were five patients in the medical records that had visited other hospitals (Fig. 2B). On the laboratory data, elevation of CRP was observed in nine cases, and the mean value was 2.08 mg/dL (reference range, < 0.30 mg/dL). ESR was elevated in eight patients and the mean value was 36.9 mm/hr (reference range, < 20 mm/hr). The patient with the highest ESR of 105 mm/hr was an RA patient, and the ESR level was usually above average in the patient. Leukocytosis was present in only two patients (13,160 and 10,330 cells/µL), and the remaining patients showed normal levels (reference range, < 10,000 cells/µL). In two cases, calcification was not found in simple radiography, but calcification was confirmed in 10 cases on CT images (Fig. 3). The calcification was located at the lower part of the C1 arch where the insertion site of the superior oblique tendon of the longus colli is located, except for one case where calcification occurred in the anterolateral aspect of the C4–5 disc space (Fig. 4). The mean value of the retropharyngeal space was 7.2 mm, ranging from 4 mm to 10.5 mm. There was no retropharyngeal abscess or infectious spondylitis on MRI, and prevertebral effusion was present in all cases (Fig. 4C and F). Clinical, laboratory and imaging data of the 10 patients are summarized in Table 1.
DISCUSSION
Since LCCT was first reported by Hartley8) in 1964, fewer than 80 cases have been reported so far according to a recent review of literature.9) Although LCCT is known as a rare disease, it is not uncommon in clinical practice to encounter patients with LCCT.910) However, since there are not many reports yet, we analyzed patients' data to get a closer look at the clinical and imaging features of the disease. It is known that calcification occurs in the longus colli with the same mechanism as calcification occurring in the shoulder or hip. The known risk factors include repetitive trauma, recent injury, ischemia, inflammation and tissue necrosis.11) Ten patients included in this study had no recent trauma, and no specific clues were found about the cause of the disease. However, on the analysis of past medical history, there were two RA patients. Although there were no atlantoaxial instability or impaction on the images of the two RA patients, considering the high probability of instability of the upper cervical vertebrae in patients with RA,1213) there is a possibility that repetitive trauma or inflammation may have affected the occurrence of calcification in both patients. The number of patients included in this study is small, but considering that the prevalence of RA in Asians is 0.5% to 1.0%,14) it is noteworthy that two out of the 10 people included had RA. In most cases reported to date, the location of calcification was around C1 or C2.9) In this study, except for one case, calcification was located under C1 arch. There is no known evidence that calcification occurs particularly frequently in the superior oblique part of the longus colli muscle. Given that C1–2 is kinematically different from the lower cervical vertebrae, it may be conjecture that inflammation or ischemia may be more likely to occur due to repetitive trauma. All of the calcification sites were clearly identified by CT, and eight of 10 showed calcific deposit in simple radiography. As already reported in several reports, CT is a gold standard for imaging diagnosis of calcification.2) It is a less timeconsuming and relatively inexpensive tool that allows for quick and accurate diagnosis when LCCT is suspected. The osteophyte growing in the front of the vertebral body could be mistaken for calcification, but it could be distinguished from the osteophyte by confirming that the calcific deposit was located in the longus colli muscle on the CT axial view. In one patient of our study, calcification was rarely seen at the C4–5 level, but the clinical features were the same in the other nine patients. The mean time to visit after the onset of symptoms was 2.6 days, and three out of 10 patients visited the hospital through the emergency room. This indicates that LCCT is also characterized by sudden appearance of severe pain like calcific tendinitis of the supraspinatus or peritrochanteric tendon. Calcific tendinitis is known to cause symptoms when it reaches the resorptive phase, because the phagocytic activity of macrophages and multinuclear giant cells occurs during this phase that leads to resorption of the calcium accompanied by an associated inflammatory response.15) In this phase, exudates come out from the cells, and the pressure inside the tendon increases, causing severe pain and limitation of movement. In our study, all 10 patients complained of severe neck pain and stiffness, accompanied by odynophagia. Although there were nonspecific symptoms such as headache and radiating pain, the three symptoms mentioned above may be a symptom triad that is typical of LCCT. Clinically, when neck pain and odynophagia accompany, infectious disease such as retropharyngeal abscess should be distinguished. We found that hyperintensity effusion was broadly distributed in the prevertebral space on the T2-weighted image of MRI, and there was no wall enhancement suggesting prevertebral abscess. The retropharyngeal swelling occurred with effusion, and the mean value measured by simple lateral radiography was 7.2 mm, well above the normal value of less than 4 mm. Laboratory data also showed mild elevations due to inflammatory response, showing differences from infectious disease. Symptoms of LCCT are sudden and very severe, but it is known that symptoms respond well to conservative treatment in 1 to 2 weeks. Our results showed an average of 4.6 days to symptomatic resolution. Since LCCT is an inflammatory disease, most cases are treated with NSAID or short-term steroid treatment.3611) Although there is no definite treatment manual, the symptoms of the initial phase are extreme, so in our experience the short-term use of IV steroids seemed to help with symptom relief. Among the results of this study, it is noteworthy that half of the patients had records that they had previously visited other clinics. Since LCCT is not a well-known disease to the physician and there are not many reported cases, it would be difficult to put LCCT into the differential diagnosis. In one study, the prevalence of LCCT was reported to be 0.5 per 100,000, but the authors also reported that the actual prevalence rate maybe higher considering misdiagnosis rate and the nature of the disease that heals naturally.9) And almost all authors who reported LCCT presumed that the disease was more likely be present than expected.234) Therefore, it is important for the physicians to be aware of the disease and differentiate it when there are similar symptoms. In this study, we analyzed 10 patients to further elucidate the clinical and imaging features of LCCT. However, the number of cases was still small to generalize the characteristics of LCCT. Further studies should follow a larger number of patients to better understand the characteristics of LCCT. For now, this study is meaningful in that it demonstrated the importance of recognizing the characteristics of LCCT.
On the basis of the outcomes in the current study, we have found that LCCT has characteristic clinical features of severe neck pain, neck stiffness and odynophagia. It also has an imaging characteristic that calcic deposit appears mainly in the superior oblique portion of the longus colli muscle with prevertebral effusion. Conservative treatment with short-term IV steroid injection and NSAID administration dramatically relieved symptoms. Understanding the characteristics of this disease can prevent unnecessary testing and misdiagnosis.
 XML Download
XML Download