

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Quantitative assessments of the health status of a population are important for decision-making and priority-setting processes in the field of public health (1). The health status and major health problems have traditionally been identified using metrics including cause-specific mortality rates, life expectancies, and incidence and prevalence rates (1). This approach is becoming unwieldy, however, when monitoring and comparing a number of problems over time, or assessing the impact of specific health interventions, as is done in cost-effectiveness analyses (2). Furthermore, recent changes in demographic and epidemiologic factors are having a major impact on the health status of many populations. For example, non-communicable diseases (NCDs) and their often non-fatal but long-term impact on health has become a major concern, leading researchers to question whether the observed gains in life expectancy have been accompanied by improvements in health status (1345). Thus, methods to measure a population’s full health spectrum, including NCDs and injuries are required.
Burden of disease (BoD) analysis has helped meet this need (1). The Global Burden of Disease (GBD) study, launched by the World Bank and the World Health Organization (WHO) in 1991 (6-10), represents a major advance in the quantification of the impact of diseases, injuries, and risk factors and its results have increased our understanding of basic descriptive epidemiology of global population health (11). With the success of the GBD study, the BoD technique has become predominantly associated with the GBD approach and its methodology using disability-adjusted life year (DALY) is now widely accepted (1).
The first national BoD study in Korea using the DALY metric was presented in 2002 (12), and many diverse BoD studies have been conducted since (1314151617181920212223242526272829303132333435). The DALY concept, however, is primarily used academically and has not yet been actually utilized in the health policy arena. Therefore, in this article, we review the DALY metric and population-based Korean BoD (KBD) studies, with the intent of increasing the understanding of their value and their potential role in strengthening future assessments of the Korean population’s health status.
DALY AS A SUMMARY MEASURE OF POPULATION HEALTH
Summary measures of population health (SMPH) combine information on mortality with that on the vast array of non-fatal health outcomes so as to represent a population’s health as a single numerical index (336). Such summary measures have a range of potential applications, such as comparing the health of one population with that of another, monitoring changes in the health of a given population over time, identifying and quantifying health inequalities within a population, providing appropriate and balanced attention to the effects of non-fatal health outcomes on overall population health, prioritizing health service delivery and planning, informing research and development efforts, and analyzing the benefits of health interventions to enable cost-effectiveness analyses (337).
The wide range of summary measures developed in the past fall into two broad categories: health expectancies and health gaps (23). Both classes use time as an appropriate metric for measuring the impact of both mortality and non-fatal health outcomes (3). Health expectancies estimate the average time that a person could expect to live in a defined state of health and are useful for summarizing the average health attainment of a population and for communication to a general audience (38). Health gaps extend the notion of mortality gaps to include time lived in states other than ideal health, and are used to measure the difference between the actual health of a population and a defined ideal (311). While health expectancy measures do not naturally lend themselves to disaggregation by categorically defined causes, health gap measures permit categorical attribution of the fatal and non-fatal BoDs and injuries to an exhaustive and mutually exclusive set of disease and injury causes (239). Because one of the fundamental goals in choosing an SMPH for quantifying the GBD is to enable identification of the relative magnitude of different health problems, including diseases, injuries, and risk factors, a health gap measure was chosen for the GBD project and a new SMPH, the DALY, was developed (2394041). Driven by the influential GBD projects (3424344454647484950), the DALY has attracted the most attention among composite health gap measures and become the dominant SMPH (1).
Years of life lost (YLL), years lived with disability (YLD), and their sum, the DALY
The DALY, by aggregating information on mortality and morbidity into a single number in units of healthy life lost, provides a unique perspective that integrates fatal and non-fatal outcomes while still allowing each to be examined separately (51). One DALY is one lost year of healthy life (52). To allow aggregation and comparison of the burdens of different diseases and injuries, mortality is quantified as years of life lost (YLLs) by taking into account the age at which death occurs. YLL is computed by multiplying the number of deaths at each age by the standard life expectancy for that age (53). Morbidity is converted to years lived with disability (YLDs). YLD represents the lost years of full health. By means of disability weights, the degree of disability imposed by each condition on those who live with the disease is scaled from 0 (perfect health) to 1 (equivalent to death) (344552535455). YLD is computed by multiplying the number of incident cases by their expected mean duration and the disability weight of the disease (53). These metrics, like all other SMPHs, explicitly or implicitly include a series of social value choices that must be decided in the planning process — namely, reference life expectancy, disability weights, time discounting, and age weights (35657). Since the initial GBD study in 1990, these value choices have been extensively debated (342434445464748495057). In GBD 2010, a simpler version of DALYs was introduced (5758) by the Institute for Health Metrics and Evaluation (IHME). That study used prevalence YLD rather than incidence YLD, and dropped time discounting and age weights, thereby resulting in a YLD computation procedure in which the prevalence of a sequela is multiplied by its associated disability weight (57). While the YLL calculation inherently takes an incidence-based perspective, non-fatal health outcomes can be quantified using either incidence- or prevalence-based measures (53596061). This issue is discussed further later in this article.
MEASURING KOREAN POPULATION HEALTH USING THE DALY METRIC
The various KBD DALY measurement studies (1314151617181920212223242526272829303132333435) can be narrowed down to two major works supported by the Ministry of Health and Welfare. The first, KBD 2002, was a 4-year research project and involved the collaboration of five institutions (Seoul National University, the Korea Institute for Health and Social Affairs, Kyung Hee University, Sungkyunkwan University, and Hanyang University). Using national population health data, this project demonstrated the applicability of DALYs for KBD analyses. The project provided a set of epidemiological estimates, YLLs, YLDs, and DALYs for 150 diseases and 3 risk factors for the reference year 2002. Key methodology and results were reported in 2007 (16). The second work, KBD 2012, is a recent 5-year project involving four collaborating institutions (Korea University, University of Ulsan, Ewha Womans University, and Kyung Hee University). Key findings from the first phase of the work have been published (29303132333435). The study covered 313 diseases and injuries for the reference year 2012, using improved methodology and an enhanced, higher-quality national database.
KBD 2002 vs. KBD 2012
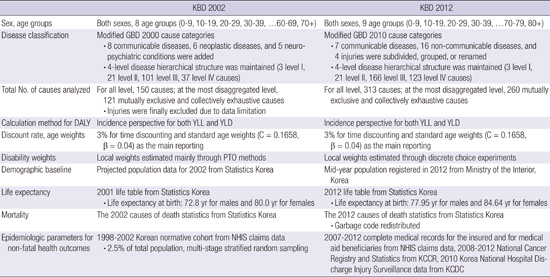
While the basic concept and approach of the two major studies — KBD 2002 and KBD 2012 — were consistent with the original GBD study (3), some modifications were made to adapt them to the Korean population. Table 1 summarizes the methods and data sources of each study. In KBD 2002, a Korean normative cohort was constructed to estimate the epidemiologic data. The cohort was a representative sample of 1,209,693 participants randomly selected from National Health Insurance Service (NHIS) claims data from 1998 to 2002, which covers about 2.5% of the total eligible Korean population. Stratified random sampling was conducted with proportional allocation by age group, sex, area of residence, and type of insurance. To compensate for the limitations of the medical utilization database, morbidity estimates were determined by reviewing medical records. The severity of each non-fatal health outcome was quantified by medical professionals using measurement methods including person trade-off, time trade-off, visual analogue scale, and standard gamble. Cause-specific mortality was estimated from Statistics Korea 2002 data.
Table 1
Summary of methods and data sources for KBD 2002 and KBD 2012

KBD = Korean Burden of Disease, GBD = Global Burden of Disease, DALY = disability-adjusted life year, YLL = years of life lost due to premature mortality, YLD = years lived with disability, PTO = Person Trade-off, NHIS = National Health Insurance Service, KCCR = Korea Central Cancer Registry, KCDC = Korea Centers for Disease Control and Prevention.
In KBD 2012, considerable effort was made to address the limitations of KBD 2002: the cause list was expanded to encompass 313 causes, the complete medical records for 2007–2012 were used instead of sample cohort data, and data from the Korea Central Cancer Registry and the Korea Centers for Disease Control and Prevention were added to improve the precision of cancer and injury estimates. Disability weights were estimated through discrete choice experiments. For cause-specific mortality, “garbage code” redistribution algorithms were used to improve accuracy of the problematic underlying causes of death in the data. Although we are fairly confident in the values estimated from these refined data and enhanced methodologies, there remain opportunities to enhance the precision of the underlying epidemiological data. One option is to combine treatment or prescription information with the main diagnostic codes in NHIS claims data analyses. An uncertainty level could also be provided based on sensitivity analysis of different extraction criteria. Additionally, consistent longitudinal epidemiologic studies and population-based surveys would support these results, providing supplementary information that could validate the epidemiological indicators or indicate how the NHIS claims data could be adjusted to reflect population estimates more precisely.
While these single-year works provide valuable comprehensive health status assessments and indicate the important contributors to a population’s BoD at a given time(Tables 2 and 3), they do not allow the study of changing epidemiologic patterns over time. To continue providing evidence to guide policy and practice priorities (62), such information should be produced and updated on a regular basis using consistent data and metrics. This would strengthen health assessments using the DALY metric in Korea and enhance their value for policy and program development (63).
Table 2
Top 10 specific causes of disability-adjusted life years (DALYs) in KBD 2002

YLLs, YLDs, and DALYs per 100,000 population. Sums may not add up to exact total due to rounding.
KBD = Korean Burden of Disease, ICD-10 = International Classification of Diseases 10th revision, DW = disability weight, YLL = years of life lost due to premature mortality, YLD = years lived with disability.
Table 3
Top 10 specific causes of disability-adjusted life years (DALYs) in KBD 2012
YLLs, YLDs, and DALYs per 100,000 population. Sums may not add up to exact total due to rounding.
KBD = Korean Burden of Disease, ICD-10 = International Classification of Diseases 10th revision, DW = disability weight, YLL = years of life lost due to premature mortality, YLD = years lived with disability.
KBD vs. GBD
While the GBD study provided an overall picture of global health, it depended on sparse and often inconsistent data (54), and it used the same disability weights for everyone in a given health state and the same ideal life expectancy for all regions of the world. Thus, the data are not likely to be equally descriptive for all nations. We conducted the KBD, on the other hand, as a national study. We adopted the GBD concepts but used Korean data sources that reflect the Korean health status and disease states. The current KBD methodology is described elsewhere (29303132333435). We used life expectancy tables produced by Statistics Korea, derived local disability weights, and applied time discounting and standard age weights to incidence-based YLLs and YLDs. We extracted basic epidemiologic parameters mainly from the claims data of NHIS, the national insurer that covers about 97% of the population and is presumed to have complete medical records for both the insured and medical aid beneficiaries (64). Even with its limitations, NHIS represents the overall population trends in health care needs. Because the data and methods used by the KBD and GBD differed, their results are not directly comparable.
Incidence-based DALYs vs. Prevalence-based DALYs
In the GBD 1990 and subsequent WHO updates, DALYs were computed from incidence-based YLDs to ensure consistency with the inherently incidence-based YLL calculations (5759). Therefore, the sum of the two components (i.e., DALYs) estimates the future stream of healthy years that will be lost as a result of the current-year incidences of specific conditions (11). If both fatal and non-fatal outcomes are analyzed using prevalence, a health gap could be measured based on the prevalence of non-fatal health outcomes and of deceased individuals who would have lost years of life in the reference time period (3). However, the self-described prevalence-based studies actually compute incidence-based YLLs and prevalence-based YLDs and then simply combine the two components. This inconsistency calls into question the utility of the resulting DALYs, which could best be described as the years of future life lost to premature deaths in the reference year plus the amount of disability experienced in the reference year (61). This was considered an acceptable method in IHME’s GBD 2010 (5761), and the methods and estimates from that study contributed to the recent updates of the WHO’s Global Health Estimates for mortality, causes of death, and disease burden (559). In terms of YLDs, incidence-based estimates describe health loss resulting from newly diagnosed cases in the reference year, and thus reflect more recent epidemiological trends. Prevalence-based estimates, on the other hand, describe current health losses arising from incident or prevalent cases in the reference time period. Taking advantages of both methods as appropriate, the ongoing KBD project has decided to calculate both incidence- and prevalence-based YLDs and will perform comparative analyses in the 2017 follow-up study.
FUTURE DIRECTIONS
Our recent finding that non-fatal outcomes play a more important role than deaths in the nation’s disease burden (2930) highlights the usefulness of DALYs for describing the overall health status of a population (1345). Furthermore, NCD prevalence is expected to increase over the next decades (65) and concurrently, effective interventions and advances in medical technology are expected to allow those with NCDs to live longer in relatively good health. Thus, assessing the magnitude of a nation’s disease burden, rather than calculating the number of deaths, prevalence, or incidence cases, would be a more helpful approach when devising strategies to control population health. Our suggested priorities for future BoD studies in Korea are the following.
Extending the range of DALY analysis
In BoD studies, the burden can be readily disaggregated by cause at the level of diseases and risk factors, and it can be estimated for any population subgroup (66). Linking the burden with risk factors can yield insight into how best to investigate avoidable disease. Several factor- or cause-specific analyses have been conducted, but population-level, comprehensive, and comparative assessments of the disease burden attributable to specific risk factors have not been performed in Korea. The KBD project expects to assess 29 common Korean risk factors in public health. Identifying risk factors and the contribution of those factors to the burden is important, but methods to reduce risk factors at the individual- and population-levels should be studied simultaneously (67). Our KBD project team is also developing a cost-effectiveness analysis model using the CHOosing Interventions that are Cost-Effective (WHO-CHOICE) method (68). Information on intervention effectiveness is expected to provide a useful evidence base for setting priorities to maximize population health with limited resources (68). In addition, regional and socioeconomic analyses can lead to targeted health planning and allow monitoring of inequalities in the distribution of health care services. More broadly, the usefulness of DALYs should be evaluated further as we develop more practical health statistics to meet the nation’s specific health planning needs.
Improving estimate precision
The accuracy of DALYs depends primarily on the accuracy of the underlying epidemiologic data (526970). The KBD project is working to address the study’s limitations and methodological problems to improve this accuracy (29). We hope to refine the methods and improve the validity of the DALY estimates so we can more precisely measure Korean population health (66).
Producing comparative and consistent evidence
While GBD paints the big picture and compares diseases, injuries, and risk factors in different world populations (57), KBD quantifies the national burden of disease in Korea. The KBD study would be more meaningful if it could track changes that occur over time so that patterns, progress, and new challenges could be identified. Estimates for a wide range of health problems should be produced and updated regularly and consistently (295457). This broad body of evidence will strengthen the KBD analysis, which will help guide future health policy, interventions, and research.
 XML Download
XML Download