

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Child and adolescent psychiatry is a still-developing field, and in Korea is a salient public issue. Previous research investigating the prevalence of mental disorders among children and adolescents under 18 years old living in Seoul suggested that 25% of them contend with mental health problems, and that these are sufficiently severe in about 10% of this population to require treatment (1). Child psychiatry in western medicine (WM) meets a significant part of patients’ needs, while in Korea, psychiatric practices in Traditional Korean Medicine (TKM) also meet those needs. Korea has a unique dual medical system. Patients in Korea can access both WM and TKM, as needed. Furthermore, WM and TKM have different approaches to illnesses (2). The diagnostic framework and treatments of TKM are based on ancient texts, which emphasize that disharmony or imbalance of one’s internal energy (chi) causes illness. Thus, the goal of treatment in TKM is to re-balance vital energy. Treatment modalities of TKM include acupuncture, moxibustion, herbology, and cupping (34). In general, patients choose WM or TKM depending on their preferences and individual experiences. The relationship between WM and TKM is rife with ideological and economic conflict.
In WM, child and adolescent psychiatry is a subspecialty of general psychiatry focusing on the mental health of youths under 18. In 1980, Korea launched a child and adolescent psychiatry fellowship program. After this, the Korean Academy of Child and Adolescent Psychiatry was established in 1983 for the promotion of scholarly exchanges (5). General psychiatrists can now be board-certified in child and adolescent psychiatry through additional coursework fellowship and exams as of 1997, allowing for the systemic education and training of child and adolescent psychiatrists. The number of board-certified child and adolescent psychiatrists is 235 as of April 2015. In TKM, the Korean Society of Oriental Neuropsychiatry was established in 1970, followed by introduction of a specialty board system and establishment of the associated law in 1999-2000. The TKM psychiatry board certification exam has been given since 2003, and thus far, 159 practitioners of TKM who specialize in psychiatry have been certified (26). However, there is no branch of child and adolescent psychiatry in TKM, and so treatment in these cases is through TKM-based general psychiatrists or pediatricians.
In 2010, the Korean standard classification of diseases-Oriental medicine (KCDO) and the Korean standard classification of diseases (KCD) were integrated into a system called the KCD-6 (7). The KCD-6 has led to the objective comparison of WM and TKM, through analysis of Korean health insurance claims data. The aim of this study was to compare utilization of WM and TKM in mental disorders of children and adolescents. We analyzed the claim frequency of F-codes – the KCD-6 category “Mental and behavioral disorders” – among 0-18 year-old patients from 2010 to 2012.
MATERIALS AND METHODS
Data collection
We assembled nationwide, population-based claims data of the Health Insurance Review and Assessment Service (HIRA) of Korea between 2009 and 2012. NHIS is a Korean public insurance service that is compulsory for all residents of Korea. Thus, NHIS covers approximately 98% of the Korean population, and the claims data from HIRA represent about 90% of the total population in Korea (8). Healthcare service providers submit claims to HIRA for purposes of reimbursement. Specifically, we examined the data for F-codes (Mental and behavioral disorders, F00-F99). Data prior to 2009 was excluded to prevent misclassification or confusion related to the pre-KCD-6 separate classification systems (9).
Ultimately, we selected 431,799 subjects (ages 0-18 years) from the HIRA database.
Variables and statistical analysis
Rates of mental disorder diagnoses in WM or TKM are affected by confounding factors, including age, gender, health insurance type as a measure of socioeconomic status, and comorbidities of psychiatric disorders. We classified samples into three age groups, age 0–7, 7–12, and 13–18 years old. We counted psychiatric comorbidities by counting the additional F-codes inserted in an individual’s claim, in the range of 1 to 5.
We compared the Top 10 highest frequency F-codes in children and adolescents for both WM and TKM, then calculated the Top 5 highest frequency differences of F-codes by age.
We then used χ2 tests to analyze significant differences in the utilization of WM and TKM, according to claimants’ characteristics. All statistical tests were considered significant at P < 0.05, and were conducted using commercially available software (Enterprise Guide ver. 4.3, SAS Institute Inc., Cary, NC, USA).
Ethics statement
This study protocol was approved by the institutional review board (IRB) of the Inje University Sanggye Paik Hospital of Korea (IRB No. 2015-02-001). Claims data were provided and analyzed anonymously, and the research had no risk of identification of claimants in the sample, and the board waived the requirement of informed consent.
RESULTS
The total number of claimants with F-codes was 431,799 from 2010 to 2012. Of these, 161,935 claims were made in 2010, 138,232 claims in 2011, and 131,632 claims in 2012. Further, in that total, 356,907 (82.66%) utilized WM and 74,892 (17.34%) used TKM.
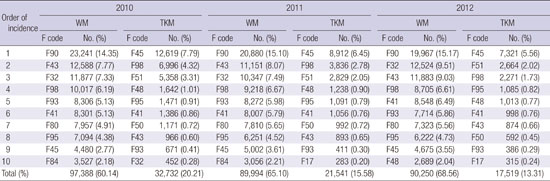
The claim frequency of F-codes declined yearly. In WM, there were 127,667 claims in 2010, 115,837 claims in 2011, and 113,403 claims in 2012. In TKM, there were 34,268 claims in 2010, 22,395 claims in 2011, and 18,229 claims in 2012. Because the claim frequency of TKM declined more rapidly than that of WM, the ratio of WM to TKM increased (Table 1).
Table 1
The incidence of mental disorders (F codes of ICD-10) by age and sex between 2010 and 2012

Of the total claimants, 58.76% (n = 253,720) were men. The male-to-female ratio was 1.63 in the 0–6 age group, 1.96 in the 7–12 age group, and 1.04 in the 13–18 age group. In WM, the overall male-to-female ratio was 1.50, and in TKM it was 1.12. In WM, the male-to-female ratios in the 0–6, 7–12, and 13–18 age groups were 1.83, 2.13, and 1.07 respectively. In TKM, the male-to-female ratios in the 0–6, 7–12, and 13–18 age groups were 1.24, 1.23, and 0.92, respectively (Fig. 1).
Fig. 1
The incidence of mental disorders (F codes of ICD-10) by sex between 2010 and 2012.
M, male; F, female; TKM, traditional Korean medicine; WM, western medicine.

From 2010 through 2012, the number of claims increased with age. There were 114,906 claims (26.61%) in the 0–6 age group, 134,539 claims (31.16%) in the 7–12 age group, and 182,354 claims (42.24%) in the 13–18 age group. In WM, the number of claims was 82,344 (23.07%) in the 0–6 age group, 115,665 (32.41%) in the 7–12 age group, and 115,665 (44.52%) in the 13–18 age group. WM was utilized most frequently in the 13–18 age group. In TKM, the number of claims was 32,562 (43.48%) in the 0–6 age group, 18,874 (25.20%) in the 7–12 age group, and 23,456 (31.32%) in the 13–18 age group. Utilization of TKM was most frequent in the 0–6 age group, followed by the 13–18 age group and the 7–12 age group (Fig. 2).
Fig. 2
The incidence of mental disorders (F codes of ICD-10) by age between 2010 and 2012.
TKM, traditional Korean medicine; WM, western medicine; yr, year-old.

Subjects were divided into two socioeconomic status groups by health insurance type. NHIS represents the higher status, while medical aid, which is supported by the government, represents the lower group. In WM and TKM, the total number of claims relying on the National Health Insurance Service (NHIS) was 331,154 (92.78%) and 73,282 (97.85%), respectively, and the number of claims relying on medical aid was 25,753 (7.22%) and 1,610 (2.15%), respectively (Table 2). The number of claims to medical aid by using TKM was relatively low.
Table 2
The incidence of mental disorders (F codes of ICD-10) by medical insurance type between 2010 and 2012

From 2010 to 2012, the highest frequency F-code claims in children and adolescents using WM were F90 (Hyperkinetic disorders) at 17.96%, and F43 (Reaction to severe stress and adjustment disorders) at 9.98%. The most frequent F-code claims in TKM were F45 (Somatoform disorders) at 38.52%, and F98 (Other behavioral and emotional disorders with onset usually occurring in childhood and adolescence) at 17.50%. The remainder of the highest 10 frequency claims, broken down by year and type of medicine utilized, are provided in Table 3. Note that there was little overlap in the high-frequency F-codes between WM and TKM.
Table 3
The incidence of the top 10 of F codes of ICD-10 between 2010 and 2012
ICD-10, International Classification of Disease and Health Problems 10th Edition; WM, western medicine; TKM, traditional Korean medicine; F code, Code for Mental and behavioural disorders in ICD-10; No., number; %, percentage of the total F-code claims in the year; F17, disorders due to use of tobacco; F32, depressive episode; F41, other anxiety disorders; F43, reaction to severe stress and adjustment disorders; F45, somatoform disorders; F48, other neurotic disorders; F50, eating disorders; F51, nonorganic sleep disorders; F80, specific developmental disorders of speech and language; F84, pervasive developmental disorders; F90, hyperkinetic disorders; F93, emotional disorders with onset specific to childhood; F95, Tic disorders; F98, other behavioral and emotional disorders with onset usually occurring in childhood and adolescence.
When broken down by age group, F90, the most frequent claim code in WM, was commonly found in the 7–12 age group. Codes F43, F32 (Depressive episode), and F41 (Other anxiety disorders) were frequently noted in the 13–18 age group. Finally, code F98 was commonly cited in the 0–6 age group. Code F45, the most frequent claim code in TKM, and F48 (Other neurotic disorders), the 4th-ranked code, were most common in the 13–18 age group. F98 and F51 (Nonorganic sleep disorders), the 2nd- and 3rd-ranked codes, respectively, were most frequent in the 0–6 age group. F95 (Tic disorders), the 5th-ranked code, was common in the 7–12 age group (Table 4).
Table 4
The incidence of the top 5 of F codes of ICD-10 by age between 2010 and 2012

ICD-10, International Classification of Disease and Health Problems 10th Edition; WM, western medicine; TKM, traditional Korean medicine; F32, depressive episode; F41, other anxiety disorders; F43, reaction to severe stress and adjustment disorders; F45, somatoform disorders; F48, other neurotic disorders; F51, nonorganic sleep disorders; F90, hyperkinetic disorders; F95, tic disorders; F98, other behavioral and emotional disorders with onset usually occurring in childhood and adolescence.
As seen in Table 5, almost half the claims (47.29%) using WM had only one F-code, and the number with more than one code dropped sharply, with only 1.87% having 5 codes. The same trend was seen using TKM, in which 70.25% of claims had one code, but only 0.71% had 5 codes. The prevalence of a single disorder without comorbidities was high in both WM and TKM, and particularly in TKM. Overall utilization of TKM was relatively low in patients who had comorbidities.
Table 5
The incidence of mental disorders (F codes of ICD-10) by the number of comorbidity between 2010 and 2012
DISCUSSION
We compared the demographic characteristics and frequency of diagnosis of patients who utilized WM and TKM for child and adolescent psychiatry. We identified trends in the utilization of WM and TKM child and adolescent psychiatric care by examining 3 years of HIRA data.
One of the strengths of this study is the analysis of data on the nationwide population in Korea. To our knowledge, this is the first study to compare WM and TKM in child and adolescent psychiatry using nationwide data. The large sample size provided high statistical power. The comparative study of WM and TKM has been rare, because WM and TKM have different approaches and diagnoses. Having no standardization, it is difficult to compare WM and TKM objectively. This type of comparison has been enabled by using the KCD-6 integrated diagnostic classification system.
Claims for child and adolescent psychiatry in both medicinal systems declined yearly, contrary to the expectation that claims would increase with the increasing need for mental healthcare of children and adolescents. It is, however, consistent with previous studies which noted that Koreans are reluctant to visit psychiatrists. Patients and their families have negative attitudes to psychiatry because they perceive mental illness as a stigma (1011). They are concerned that a medical record of a mental disorder may interfere with their careers. Thus, they tend to hide mental problems and dismiss them as personal problems instead of seeking appropriate treatment (12).
Some patients pay in full, and in these cases psychiatrists do not make claims to HIRA. Patients also choose therapies such as cognitive behavioral therapy (CBT), play therapy, or learning therapy, rather than pharmacotherapy which requires an F-code record. Furthermore, government support is inclined towards these therapies and non-medical institutions. These reasons could shed light on the decline of F-code claims (1314).
Several hypotheses may explain the higher rate of decline of F code claims in TKM. First, our other data indicate that children and adolescents needing psychiatric care visit WM psychiatrists psychological counseling centers primarily. Second, TKM practitioners prescribe Hanyak, herbal medicine, which is not covered by health insurance. In addition, practitioners in TKM do not need to claim F-codes. According to a previous study, but inconsistent with our data, psychotherapy in TKM increased annually. This suggests that the actual utilization of TKM could be increasing (15). Frequently, TKM practitioners advertise to potential patients that they can treat their mental illnesses without psychiatric medical records.
In WM, F-code claims increased by age. This finding is inconsistent with previous studies (1617). Adolescents in Korea experience pressure to compete with each other for higher academic achievement, which causes additional pressure to study. Problems at school such as school violence and bullying also affect adolescents’ mental health. Indeed, the rate of suicide in adolescents (10–19 year olds) has increased gradually from 3.8% in 2000 to 5.2% in 2010 (18). School-age children’s mental health has become a public issue, and now includes intervention efforts by families, teachers, and friends necessary to manage (or at least self-monitor) their mental health. These trends could explain the increased F-code claims in this age group (1920).
In TKM, claims in 0–6 age group were the most frequent. Most likely, the parents of younger children may have a more negative attitude toward psychiatrists in WM, or to psychiatric medication. Further, when children experience mental distress or trauma, they tend to display externalized symptoms such as change in appetite, sleep, toilet habits and somatic symptoms (21) which may not be recognized as mental health issues. Thus, parents take their younger children to TKM practitioners first, for hanyak or acupuncture.
The different male-to-female ratios in WM age groups may be related to the different F-codes most frequently found in each group. For example, in the 0–12 age group, F90 and F98 were frequently claimed codes. F90 is the code for Attention Deficit/Hyperactivity Disorder (ADHD), which is significantly more common in boys than girls (up to 9:1). F98 includes diagnoses like enuresis, which is about 1.5 times more prevalent in boys, and encopresis, which is three to six times more likely to occur in boys than girls (3).
In contrast, the frequently diagnosed F43, F32, and F41 in the 13–18 age group in WM are equally prevalent, or more prevalent in females. These codes include conditions such as acute stress disorder, PTSD and adjustment disorder. They also include trauma-related disorders, which are more prevalent in females (3). There is no significant sex difference in the prevalence of adjustment disorder or in major depressive disorder in school-age boys and girls (22). However, in adolescents, major depressive disorder is two to three times more prevalent in females than males (3). Together, these conditions probably cause the male-to-female ratio to be more balanced in the older age group. Although the data on the 13–18 age group in WM suggests a higher utilization rate for females, our results suggest the ratio was about equal. This result suggests that female adolescents may not visit clinics despite the need for treatment.
There was less of a difference by sex in TKM than in WM. The disorders within codes F98 and F51 are mostly gender-neutral, though sleepwalking in persistent parasomnias is more prevalent in males than females (23). This prevalence may explain the lower gender difference in TKM overall, but the higher utilization ratio of males restricted to the 0–6 age group.
The F45 code related to somatoform disorders was overwhelmingly frequent compared to the other codes. Because research of somatic symptom disorders in children has been limited, its prevalence in children is unclear. One report showed an equal prevalence in prepubertal males and females, though the female incidence increases after puberty, while the male incidence falls at this time (24). Therefore, the minimal gender differences in TKM and slightly increased female ratio in the 13–18 age group might be associated with somatoform disorders.
As medical aid supports lower income and socially disadvantaged groups, the insurance type reflects patient’s socioeconomic status. Medical aid patients are free or almost free of cost-sharing, but because many TKM procedures and treatments are not covered, they would be required to pay in full. Thus, low income/medical aid patients may prefer WM over the costs associated with TKM.
This large scale study demonstrated that F45 claims are much more frequent in TKM. This result is consistent with previous studies that somatization patients account for a high percentage of utilization of TKM neuropsychiatry services (252627). Furthermore, in WM, F90 (Hyperkinetic disorders) were common, a result also supported by previous studies (13).
In WM, F43 and F32 codes followed F90 in rank order. Patients in WM who visit psychiatrists tend to have emotional problems caused by psychological distress. In TKM, however, behavioral problems in codes F98 and F51 ranked high. This result suggests that internalized psychological problems are treated more often with WM, and externalized physical/behavioral problems are treated more often with TKM. These trends suggest that patients perceive psychiatry in WM as treating mental problems through psychotherapy or medicine, while psychiatric medicine and psychiatry in TKM treat abnormal behavior and somatic symptoms whose cause is unknown.
There are less comorbidities in TKM than in WM. This result suggests that there are more patients who have multifaceted problems and a complex pathology in WM. Alternatively, practitioners of psychiatry in TKM may lack the training to properly assess comorbidities.
The major limitation of this study is that patient attitudes toward either WM or TKM could be affected by many factors, including patients’ residential location, first episode or recurrence. Other variables such as hospitalization and medication use reflecting severe mental disorders also remain to be investigated in further studies. It would also be helpful to compare the time courses of utilization of both WM and TKM, to determine the direction of patient flow between WM and TKM.
TKM interprets and manages mental problems of children and adolescents according to their own theory and mechanism, and diagnose based on the ICD-10. Practitioners of TKM who specialize in psychiatry tend to refer to the DSM-5 and report F-codes. However, there are very few of these certified practitioners, so diagnosis based on the DSM-5 may not be accurate or complete. Because of the different approaches and diagnostic flow between WM and TKM, it is difficult to see F-code claims as matching identically. Therefore, child and adolescent psychiatry in TKM should develop a more specialized training system and further evidence-based research to improve its mental health diagnostics.
A significant number of patients who have ADHD use WM, which also frequently receives cases of psychological problems such as depression and anxiety. On the other hand, patients who visit TKM are more commonly seen for physical health-related problems such as somatoform disorder, sleep disorder, and eating disorder.
WM and TKM need to complement each other to maximize the treatment benefits for mental disorders, and minimize the medical expense of patients. Psychiatrists in WM should inform the public that somatic symptoms could be caused by psychiatric problems, and thus relieve patients’ somatic concerns. As well, practitioners in TKM should be acquainted with formal diagnostic systems such as the DSM-5 to better correlate their code reports with those of WM.
 XML Download
XML Download