

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Since cytological screening with the Papanicolaou (Pap) test was introduced, the incidence of cervical cancer has decreased markedly. However, this disease remains a sizeable health problem, accounting for an estimated 528,000 new cases and 266,000 deaths worldwide in 2012 [1]. In Korea, cervical cancer incidence has decreased continuously, largely due to the detection of precursor lesions using the Pap test [2]. Nevertheless, cervical cancer is still the most common gynecological cancer, and the age-standardized incidence was 9.5 per 100,000 persons in 2013 [3]. Accordingly, it remains a significant public health concern in Korea.
Currently, 2 population-based cervical cancer screening programs are operated by the Korean government. One is the National Health Insurance Service Cancer Screening Program (NHISCSP), which is offered to National Health Insurance Service (NHIS) beneficiaries in the upper 50% income stratum, and the other is the National Cancer Screening Program (NCSP), which is offered to NHIS beneficiaries in the lower 50% income stratum and Medical Aid Program (MAP) recipients. Both the NHISCSP and the NCSP provide complimentary biennial cervical cancer screening for all Korean women over the age of 30 years [4].
A report regarding the results of the Korean nationwide cervical cancer screening program in 2009 was published [5]. To achieve timely objectives in public health, it is important to monitor current trends. Thus, in this study, we sought to determine the results of the national cervical cancer screening program based on data for a recent 6-year period for NHISCSP and NCSP. Here, we report the participation rates and the rates of abnormal Pap smear results by age between 2009 and 2014.
MATERIALS AND METHODS
1. Study data and populations
We accessed the database system of the NHISCSP and NCSP for cervical cancer. Data for the 2 screening programs from January 1, 2009 to December 31, 2014, were obtained. All Korean women aged 30 years or over are instructed to be screened for cervical cancer via the NHISCSP or the NCSP biennially. Participation in the NHISCSP or the NCSP tests was ascertained based on cervical cancer screening results presented to the NHIS. The NHIS has gathered data in a standardized form to check screening activities in both programs.
2. Variables
The conventional Pap smear test was used for cervical cancer screening in both NHISCSP and NCSP [6]. In this study, the Pap test results were classified by the pathological findings with the 2001 Bethesda system in the following categories [7]: 1) negative for intraepithelial lesion or malignancy; 2) epithelial cell abnormalities, including atypical squamous cells of undetermined significance (ASC-US), atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion (ASC-H), low-grade squamous intraepithelial lesion (LSIL), high-grade squamous intraepithelial lesion (HSIL), squamous cell carcinoma, atypical glandular cells (AGCs), adenocarcinoma in situ (AIS), and adenocarcinoma; and 3) other, a category was designated for reporting normal or abnormal endometrial cells in women who are ≥40 years old. Organisms and other non-neoplastic findings are optional under the category “negative for intraepithelial lesion or malignancy.” Abnormal Pap test results were defined as those reported as ASC-H, LSIL, HSIL, squamous cell carcinoma, AIS, or adenocarcinoma [8]. Age was considered a categorical variable and was grouped as follows: 30–39, 40–49, 50–59, 60–69, and ≥70 years old.
3. Calculation of participation rate and abnormal rates in cervical cancer screening
The participation rate in cervical cancer screening was calculated by dividing the number of participants by the target population of both NHISCSP and NCSP for cervical cancer, and is denoted as a percentage with a 95% confidence interval (CI). Changes in the annual participation rates were calculated as the annual percentage change (APC) with a 95% CI. The rates of abnormal results in cervical cancer screening were calculated by dividing the number of abnormal Pap test results by the number of participants, with a 95% CI. The ratio of ASC-US to squamous intraepithelial lesion (SIL) (ASC-US:SIL ratio) was calculated by dividing the number of ASC-US cases by the number of all SIL cases (including LSIL and HSIL).
4. Statistical analysis
The Cochran-Armitage trend test is used in categorical data analysis to assess the association between a variable with 2 categories and a variable with k categories [9]. All analyses were performed using the SAS software (ver. 9.4; SAS Institute, Cary, NC, USA) and R (ver. 3.3.2; R Foundation, Vienna, Austria; http://cran.r-project.org/mirrors.html). p-values <0.05 were considered to indicate statistical significance.
RESULTS
1. Population and participation
Data were collected from January 2009 to December 2014. The target populations of the NHISCSP and NCSP for cervical cancer screening and the participation rates according to time are described in Table 1. The participation rates varied from 41.10% in 2009 to 51.52% in 2014, trending toward a gradual increase (APC, 4.126%; 95% CI=2.253–6.034; Fig. 1A).
Table 1
Pap smear results by timeline from the NHISCSP and the NCSP for cervical cancer (2009–2014)
Values are presented as number (%) or median (95% CI).
AGC, atypical glandular cell; AIS, adenocarcinoma in situ; ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; CI, confidence interval; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; NCSP, National Cancer Screening Program; NHISCSP, National Health Insurance Service Cancer Screening Program; Pap, Papanicolaou; SIL, squamous intraepithelial lesion.
*The presence of organisms such as Trichomonas vaginalis or fungal organisms consistent with Candida species will be included as a comment in this category. Components that are optionally listed in the category include atrophy, radiation, and inflammation; †The rates of abnormal results in cervical cancer screening were calculated by dividing the number of abnormal Pap test results by the number of participants, with a 95% CI; ‡The ratio of ASC-US to SIL (ASC-US:SIL ratio) was calculated by dividing the number of ASC-US cases by the number of all SIL cases (including LSIL and HSIL).
Fig. 1
(A) Participation rates by timeline from the NHISCSP and the NCSP for cervical cancer during study period (2009–2014). (B) Participation rates by age from the NHISCSP and the NCSP for cervical cancer during study period (2009–2014).
NCSP, National Cancer Screening Program; NHISCSP, National Health Insurance Service Cancer Screening Program.

Fig. 1B shows the age-based participation rates in the NHISCSP and the NCSP from 2009 to 2014. In both 2009 and 2010, women 50–59 years of age had the highest participation rate (range, 50.2%–52.6%), followed by women 60–69 years of age (48.5%–51.6%). From 2011 to 2014, women 60–69 years of age had the highest participation rate (50.5%–61.3%), followed by those 50–59 years of age (50.7%–59.6%). From 2009 to 2014, women ≥70 years of age had the lowest participation rate (21.7%–31.9%), followed by those 30–39 years of age (27.7%–44.9%). Detailed results from the Pap smear tests performed each year are presented in Supplementary Tables 1,2,3,4,5,6.
The participation rates between 2012 and 2014 were determined according to health insurance type. The results are shown in Supplementary Table 7. The participation rates of National Health Insurance (NHI) beneficiaries (range, 48.58%–52.50%) were higher than those of MAP recipients (29.63%–33.17%).
2. Pap smear results
The rates of abnormal Pap smear results were calculated from 2009 to 2014 (Table 1). Detailed annual results from Pap smear tests with respect to patient age are presented in Supplementary Tables 1,2,3,4,5,6.
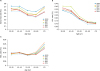
During the study period, the rates of abnormal Pap smear results tended to decrease from the age group 30–39 years to the age group 60–69 years but increased again in women ≥70 years of age (Fig. 2A). The latter group also had the most rapid increase in the rate of abnormal results. Each year, the rate of LSIL decreased with increasing age (p<0.001, Cochran-Armitage trend test; Fig. 2B), whereas the rates of HSIL/ASC-H and squamous cell carcinoma increased (p<0.001, Cochran-Armitage trend test; Fig. 2C).
Fig. 2
(A) The rates of abnormal Pap smear results according to age during study period (2009–2014). (B) The rates of LSIL on the Pap smear according to age and timeline. (C) The rates of HSIL or ASC-H on the Pap smear according to age and timeline.
ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; Pap, Papanicolaou.
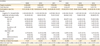
The rate of abnormal results decreased, from 0.65% in 2009 to 0.52% in 2014 (p<0.001, Cochran-Armitage trend test; Fig. 3A). A decreasing tendency was determined for the rates of abnormal Pap smear tests in all age groups, except in women 30–39 years of age (p=0.131, Cochran-Armitage trend test; Fig. 3B). Beginning in 2012, the rate of abnormal results in the youngest age group (30–39 years) was higher than that in any other age group. The rate of HSIL/ASC-H was 0.41% in 2009 and decreased thereafter (p<0.001, Cochran-Armitage trend test; Fig. 3A). The rate of HSIL/ASC-H showed a decreasing pattern for all age groups (p<0.050 for all age groups, Cochran-Armitage trend test; Fig. 3C), whereas the rate of LSIL did not (p>0.050 for all age groups, Cochran-Armitage trend test; Fig. 3D). Notably, the rate of ASC-US increased, from 0.98% in 2009 to 1.89% in 2014 (p<0.001, Cochran-Armitage trend test). This trend was observed among all age groups (p<0.050 for all age groups, Cochran-Armitage trend test; Fig. 3E). Moreover, the ASC-US:SIL ratio increased over time, from 2.71 in 2009 to 4.91 in 2014 (Fig. 3F).
Fig. 3
(A) Proportion of the abnormal Pap smear results according to timeline. (B) The rates of abnormal Pap smear results according to age and timeline. (C) The rates of HSIL or ASC-H on the Pap smear according to age and timeline. (D) The rates of LSIL on the Pap smear according to age and timeline. (E) The rates of ASC-US on the Pap smear according to age and timeline. (F) The ASC-US to SIL ratios according to age and timeline.
ASC-H, atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; SIL, squamous intraepithelial lesion; Pap, Papanicolaou.

DISCUSSION
Here, we reported the results of the nationwide organized cervical cancer screening programs operated by NHIS in Korea. In this study, the rates of participation and of abnormal results from 2009 and 2014 were analyzed according to age and time. There have been several informative studies reporting the results of the Korean population-based cervical cancer screening program [510]. However, the latest one is based on data for 2009 [5]. Moreover, the published studies included only NCSP data [510]. In contrast, the present study included data from both NHISCSP and NCSP, which together cover almost all Korean women over the age of 30 years. Thus, this study will serve as a representative analysis for a nationwide cervical cancer screening program, reflecting the latest changes and general characteristics of the Korean population.
In the present study, the participation rate in the NHISCSP or NCSP for cervical cancer rose from 41.10% in 2009 to 51.52% in 2014, trending toward a gradual increase. In 2002, the participation rate in the NCSP for cervical cancer screening was only 15.4% [4]. The Korean National Cancer Screening Survey (KNCSS) reported that the overall screening rate associated with both the organized and opportunistic cancer screening programs was 67% in 2013 [11]. This value is comparable to those in Western countries that implemented a national cervical cancer screening program earlier. According to a Europe-wide survey on the status of cervical cancer screening in 2015, 20 countries offered a population-based screening program, and the participation rates were 70% or higher in most countries (England, Denmark, Ireland, Iceland, Finland, Wales, Sweden, Italy, Slovenia, and Scotland) [1213]. In the US, the National Health Interview Survey found that the cervical cancer screening rate was 80.8% in 2013 [14]. In Korea, the cervical cancer incidence has decreased over the last decade, from 18.6 per 100,000 women in 1999 to 8.5 per 100,000 women in 2012 [2]. This is attributable primarily to the increased cervical cancer screening rate. Multiple population-based cohort studies have demonstrated that cervical cancer screening with the Pap smear lowers cervical cancer incidence because it allows detection and treatment of precursor states [1516]. Moreover, it leads to improved cure rates for invasive cervical cancer by early detection [1718]. A nationwide health-related survey in Korea reported that failure to participate in cervical cancer screening programs was associated with low income, low education, unemployment, health insurance type, older age, disability, and smoking [19]. Consistent with those findings, in the present study, the participation rates of NHI beneficiaries were higher than those of MAP recipients. Thus, to facilitate participation in cervical cancer screening programs, special attention should be paid to these populations.
There has been controversy as to whether cervical cancer screening is advantageous to the elderly population [20]. The American Cancer Society has recommended that women older than 65 years can stop cervical cancer screening if they have had 3 or more consecutive negative Pap tests [21]. However, a recent systematic review, which was the basis of the guidelines of the Canadian Task Force on Preventive Health Care, does not recommend an upper age limit [22]. A recent population-based case-control study using Surveillance, Epidemiology, and End Results (SEER)-Medicare data found that screening was protective against cervical cancer in women aged 65–74 (odds ratio [OR]=0.24; 95% CI=0.13–0.37) and 75–84 years (OR=0.44; 95% CI=0.34–0.55) [23]. These data are consistent with other studies that showed a protective effect of Pap test screening in preventing cervical cancer in women >65 years old [172425]. Indeed, one study documented benefits for women >80 years old [25]. A review of the USA 2013 cancer statistics reveals that the risk of cervical cancer doubles for women ≥70 years compared with women aged 40–69 years [26]. This raises a concern that a group of older women who are at high risk for cervical cancer are not getting screened. In this context, NHISCSP and NCSP in Korea do include women older than 65 years due to the substantial cervical cancer incidence in this population [27]. Nevertheless, from 2009 to 2014, the participation rate was lowest among women ≥70 years of age, as also demonstrated by the KNCSS data. Moreover, in the present study, the rate of abnormal test results in this age group was not negligible, although it may be that the composition of the elderly group reflects the tendency of more symptomatic women to participate in screening programs. Elderly women tend to believe that menopause frees them from gynecological diseases, so they do not to undergo a Pap test unless they have symptoms or signs [28]. Thus, more selective and active intervention for elderly women, such as increasing visiting check-ups by the community outreach service and providing mobile clinics for gynecological exams, may be beneficial to facilitate participation in cervical cancer screening [19].
Beginning in 2012, the rate of abnormal results was highest in the youngest age group (30–39 years). This finding is probably the result of the high rate of women in this age group undergoing screening for the first time, however, screening participation in this group was the second lowest (range, 27.7%–44.9%) during the study period. Moreover, no tendency toward decreasing rates of abnormal results during the study period was observed in this group, unlike the other age groups. This might reflect the recent trend of early sexual initiation. In Korea, cervical cancer incidence has been increasing in younger age groups [2930]. Additionally, increasing mortality rates have been observed in these groups. This may be a result of more cases with advanced-stage disease at diagnosis and consequent poor survival [29]. Early sexual initiation is likely to cause early exposure to human papillomavirus (HPV) infection [31]. Women infected with high-risk HPV at an earlier age may progress to high-grade cervical intraepithelial neoplasia in their early 30s [32]. Thus, women in their 30s should participate in a cervical cancer screening program. Nonetheless, the widespread concept that cervical cancer is not a disease of younger women may hamper participation by younger women in screening programs [8]. In the younger age group, a combination of early detection by screening programs, public awareness of risk factors, promotion campaigns targeting this group, and HPV vaccination will play key roles in preventing cervical cancer in Korea.
In the present study, significant increasing trends were observed for rates of ASC-US in all age groups from 2009 onward. Moreover, the ASC-US:SIL ratio increased, from 2.71 in 2009 to 4.91 in 2014. We cannot explain this increase in the ASC-US:SIL ratio during the study period, but several factors, such as slide preparation methods [33], location-guided screening provided by liquid-based cytology [34], and over-interpretation of borderline-normal cells due to awareness of medicolegal litigation [35], may have influenced the ASC-US:SIL ratio. Because ASC-US primarily conveys diagnostic uncertainty, the rate of ASC-US is monitored by numerous laboratories for quality control to minimize its overdiagnosis. Considering the dissimilar frequency of cervical dysplasia in diverse populations, the ASC-US:SIL ratio has been used as a preferred indicator. The rate of ASC-US should represent ≤5% of reports, and the ASC-US:SIL ratio should not be higher than 2:1–3:1 in general screening practice [33]. In this regard, our results indicate that efforts to ensure quality control in ASC-US reporting should be stressed. One such effort is measuring the ASC-US:SIL ratio for individual cytopathologists, with periodic confidential feedback [36]. Nascimento and Cibas [33] reported that cytopathologists whose ASC-US:SIL ratio exceeded the upper benchmark tended to reduce the ratio as a consequence of confidential feedback. Further evaluation appears warranted.
The current study has several limitations. First, clinicodemographic variables that may influence cervical cancer screening participation (education, health insurance type, marital status, disability, jobs, region, and smoking) were not addressed. Second, the rates of abnormal Pap smears were not adjusted for the rates of hysterectomy because these data were unavailable for the study period. This issue has been observed in other reports on nationwide cervical cancer screening program [837]. However, as the overall rates of hysterectomy were negligible (174 of 100,000 females) [38], this limitation would seem to have minimal influence on our findings. Third, subsequent biopsy results after abnormal Pap smear tests were not available in the present study. Thus, we did not evaluate the detection rate of precancerous lesions or the diagnostic accuracy of the screening programs. Although we calculated the ASC-US:SIL ratio, this parameter is a measure of quality assurance, not a measure of a diagnostic accuracy. Indeed, overall performance cannot be evaluated by the ASC-US:SIL ratio, but only by histological correlation, such as with biopsy results.
In conclusion, several epidemiological features of the Korean nationwide cervical cancer screening programs were identified using the NHISCSP and NCSP databases. Differences were found in the rates of participation and abnormal test results according to both patient age and health insurance type. In addition, these rates changed over time. Although the participation rates increased after 2009, further efforts are needed to improve participation in cervical cancer screening programs, especially for MAP recipients, women over 70 years of age, and those 30–39 years of age, among whom the rates of abnormal test results were highest. Additionally, quality control measures for cervical cancer screening programs should be highly and consistently maintained. It is expected that our results will be beneficial in future research and in the development of healthcare policies to prevent cervical cancer in Korea.
 XML Download
XML Download