

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Epilepsy is a common neurologic disorder, with a reported prevalence ranging from 2.2 to 17.6 per 1,000.1 Until recently, epidemiologic reports on the prevalence of epilepsy in Korea were lacking. Previously the authors reported the prevalence of treated epilepsy based on the diagnostic codes for claims and the antiepileptic drugs (AEDs) prescribed, using the database from the National Health Insurance (NHI), public third party payment system.2 That study found that the overall prevalence was 2.41 per 1,000, which is very near to the bottom of the range of the rates found in other countries. However, because the diagnostic codes of the NHI database were generated for claims, it is crucial to validate the accuracy of these codes. Although the use of administrative health data for epidemiologic studies has been increasing, few studies have estimated the prevalence adjusted by diagnostic validity. The diagnostic validity may depend on demographic, institutional, or clinical variables, and applying validity that is specific for subgroups will allow more accurate estimation of prevalence.
In this study we aimed to estimate the age- and sex-specific prevalence of epilepsy with less bias, by using a nationwide database supplemented by extensive validation performed using a medical records survey of the representative sample.
METHODS
Study design
We conducted two surveys in parallel: 1) a Health Insurance Review and Assessment service (HIRA) database survey and 2) a medical records survey. Data on potential epilepsy patients were extracted from the main HIRA database based on our working criteria described below. We also performed a nationwide survey of medical records of patients sampled from representative health institutes. Using the results of the medical records survey, we assessed positive predictive value (PPV), the probability of the HIRA database patients having epilepsy, according to diagnostic codes, age group, and sex. Finally, we estimated the prevalence of treated epilepsy by projecting the PPV derived from the medical records survey involving the number of initially presumed epilepsy patients from the HIRA database after stratifying for covariates (Fig. 1).
This study was approved by the Institutional Review Board (IRB) of the lead institutes (approval number: AN10221-001) and all participating institutes with an IRB.
Data sources
The national health system of Republic of Korea is based on the NHI system, registration in which is mandatory for the entire population and for all medical facilities, and Medicaid (MA), which is provided through a social welfare fund for registrants who are unable to pay the NHI premiums. The population coverage has been greater than 98% since 2005.3 This is basically a fee-for-service system, and all medical expenditures including for medications, medical services, and revenue are submitted to HIRA as separate claims. HIRA is a governmental third-party agency that has assessed all claims based on diagnostic codes and medical records from NHI and MA since 2000, and from the Veterans Administration since 2008. Costs for virtually all diagnostic and therapeutic practices associated with epilepsy are covered by the system, and all related records are stored in the HIRA database. We excluded patients under 1 year of age because we found that it is often difficult to determine from reviews of medical records whether they have epilepsy or acute symptomatic seizures at this age.
Potential patient dataset using the HIRA database
Our working criterion for extracting potential patients with epilepsy from the HIRA database was a prescription for at least one AED according to the list of claims in 2009. The list of AEDs, based on those available in 2009 in Korea, included carbamazepine, clobazam, ethosuximide, gabapentin, lamotrigine, levetiracetam, oxcarbazepine, phenobarbital, phenytoin, pregabalin, primidone, topiramate, vigabatrin, valproate, and zonisamide. Clonazepam was excluded because it is rarely used as a monotherapy for epilepsy and is used more frequently in other conditions. Other AEDs, including primidone, felbamate, esclicarbazepine, lacosamide, and tiagabine, were not available in 2009.
Potential epilepsy patients were classified into two categories: those prescribed AEDs with and without diagnostic codes indicating epilepsy or seizure (Diagnosis-E), based on either the principal or additional diagnostic code for the claim. Diagnosis-E included G40* (epilepsy), G41* (status epilepticus), F803 (Landau-Kleffner syndrome), and R56 (convulsion) according to the 10th version of the International Classification of Diseases and Related Health Problems (ICD-10).
In total, 7,282,236 claims from patients prescribed AEDs during 2009 were retrieved. The claims were sorted by individual based on anonymous personal identifiers and hospital identifiers, in order to determine the actual number of patients for 2009 (Fig. 1).
Medical records survey and validation of diagnostic codes for epilepsy
We collected clinical information on epilepsy patients by surveying the medical records for the validation of diagnostic codes. The survey consisted of two steps: 1) data abstraction by certified health record administrators and 2) subsequent verification by epileptologists. The health record administrators were trained to review medical records and extract data related to epilepsy. All cases were scrutinized and assessed by a board of epileptologists based on detailed clinical information abstracted by the health record administrators. Diagnoses were categorized as follows based on the 1993 International League Against Epilepsy guidelines: epilepsy, single seizure, uncertain whether epilepsy or seizure, nonepileptic, and undetermined.4 This survey method demonstrated a high validity in a preliminary study, with a sensitivity of 90% and a specificity of 97%, and kappa statistics for interrater and testretest reliabilities of 0.907 and 0.975, respectively.5
Multistage cluster sampling was performed in three geographic regions (the capital, midland, and southeast areas) categorized based on approximately even distributions of institutes and population. Based on a pilot survey of three hospitals, the sample size was estimated at 2,000 for patients prescribed AEDs with Diagnosis-E, and 4,000 for those prescribed without Diagnosis-E. Finally, we surveyed 6,774 patients from 43 institutes distributed throughout the country, comprising 4 tertiary referral hospitals, 29 general hospitals, 8 hospitals, and 2 private clinics.
Estimation of prevalence
The PPV for epilepsy was calculated as the number of patients with true epilepsy divided by the total number of patients prescribed AEDs, for age, sex, and diagnostic categories.
The total number of the cases was estimated as
NDi is the number of patients prescribed AEDs with Diagnosis-E according to the HIRA claims data, NMi is the number of patients prescribed AEDs without Diagnosis-E according to the HIRA claims data, PDi is the PPV for patients prescribed AEDs with Diagnosis-E, PMi is the PPV for patients prescribed AEDs without Diagnosis-E, Di is the number of patients prescribed AEDs with Diagnosis-E, Mi is the number of patients prescribed AEDs without Diagnosis-E, EDi is the number of cases deemed to be true epilepsy among Di, and EMi is the number of cases deemed to be true epilepsy among Mi, based on the medical records survey.
We applied the PPV derived from the medical records survey to groups of subjects extracted from the HIRA database according to specific strata. We used the age- and sex-specific national population estimated for 2009 from the Korean national statistical office as the denominator when calculating the prevalence.6
RESULTS
Validity of diagnostic codes
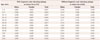
Among the total of 50,290,771 beneficiaries, 1,119,360 patients (2.2%) were prescribed AEDs during 2009, of which 155,307 (13.9%) had Diagnosis-E and 964,053 (86.1%) did not have Diagnosis-E. The PPV for epilepsy was 0.460–0.978 (overall 0.810) for the group with Diagnosis-E and 0.021–s0.324 (overall 0.066) for the group without Diagnosis-E. The ranges indicate the variations with age and sex: the PPV tended to decrease with age in both groups, with consistently lower values in females over 30 years of age based on the medical records survey (Table 1).
The number of patients prescribed AEDs with Diagnosis-E but deemed not to have epilepsy was estimated at 28,712 nationwide. The false-positive cases were determined to be acute symptomatic seizures, single seizure, or uncertain whether epilepsy or seizure (41.9%); therapeutic trial for possible seizures (7.07%); prophylactic use (18.2%); misassignment of the diagnostic codes for pain (23.7%); other purpose (4.29%); or due to an unknown cause (4.80%).
The number of patients prescribed AEDs without Diagnosis-E but determined as having epilepsy was estimated at 60,902 nationwide. The false-negative cases had diagnostic codes suggesting central nervous system pathology potentially related to epilepsy (53.6%); psychiatric illness (5%); paroxysmal disorders requiring differentiation from epilepsy, such as syncope, dystonia, cramps, and headache (5%); and those unrelated to epilepsy (36.4%).
Prevalence
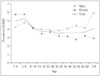
The estimated number of epilepsy patients treated with AEDs was 187,497 [95% confidence interval (CI)=185,512–188,697]. The overall prevalence was 3.84 per 1,000 (95% CI=3.81–3.87). The prevalence was higher in males (4.20 per 1,000; 95% CI=4.17–4.23) than in females (3.47 per 1,000; 95% CI=3.44–3.51) for all age groups except patients aged 1–9 years (males: 4.57 per 1,000; females: 5.78 per 1,000). The prevalence was relatively constant across age groups, with a tendency to be higher in patients younger than 15 years and in the elderly (Fig. 2) (Supplementary Table 1 in the online-only Data Supplement).
The prevalence of treated epilepsy with Diagnosis-E was 2.59 per 1,000 (males: 2.94 per 1,000; females: 2.32 per 1,000), and the prevalence of those without Diagnosis-E was 1.25 per 1,000 (males: 1.26 per 1,000; females: 1.23 per 1,000). Age- and sex-specific prevalence patterns differed between groups with and without Diagnosis-E. A plot of the prevalence against age had an inverted U-shape peaking at adolescence for patients with Diagnosis-E, and an upright U-shape for the group without Diagnosis-E (Fig. 3).
DISCUSSION
This study determined the nationwide prevalence of treated epilepsy across all ages except infants utilizing a nationwide database and validated by a medical records survey. Only a few studies have estimated the prevalence of epilepsy for the entire population of a country, for which various data sources can be used. A door-to-door survey is a traditional gold standard, but it is not practical in a large population. Although a populationlevel self-report survey has less selection bias and is less demanding than a door-to-door survey, its diagnostic accuracy is uncertain. A records-based survey is advantageous over a direct population survey in that it avoids recall bias, although selection bias may be an issue. In countries with universal health care systems, the utilization of administrative health databases is useful for nationwide epidemiologic studies with a relatively low selection bias.789
The main concerns when using administrative health data for epilepsy epidemiology studies are the correct identification of epilepsy cases and the determination of their validity. Diagnostic codes are commonly used as tracers for epilepsy810 and are often combined with AED prescriptions.7911 The validity of ICD codes for epilepsy or seizure in administrative health data has reported to be associated with PPV values of 0.347–1.00 and negative predictive values (NPVs) of 0.895–0.997.1213 The overall PPV and NPV of ICD codes for epilepsy or seizure in the HIRA database were 0.810 and 0.934, which are comparable to those of other studies, although we included only patients who had been prescribed AEDs. Case-defining algorithms that also take into account the duration of AED use, electroencephalogram, hospitalization, or emergency-room visits, and/or the number of billings could increase the validity, but there is a trade-off between the false-positive and false-negative rates.131415 The validity of the diagnostic codes has been assessed by a medical records review in several studies,1012141516 by reports from general practitioners in an Italian study,13 and by a community-based survey in a Taiwanese study.9 We traced epilepsy patients based on AED prescriptions, and assessed their PPV based on a review of medical records. The PPV decreased with age and was lower among female patients with or without Diagnosis-E, which may be due to the use of AEDs for nonepileptic purposes being more common in these populations. It is remarkable that 6.61% of the patients prescribed AEDs without Diagnosis-E were deemed to have epilepsy. Although the rate of false-negative diagnoses was relatively low, this group of patients constituted 32.6% of all treated epilepsy patients and was more than twice the number of false-positive diagnoses. Many studies of epilepsy prevalence using administrative databases,8101117 including our previous study,2 did not consider patients prescribed AEDs without Diagnosis-E as potential epilepsy patients, which may have resulted in the prevalence being underestimated.
The overall prevalence in this study is within the range reported for other East Asian countries (2.9 per 1,000 and 5.9 per 1,000).91819 We found a male predominance, which is also consistent with most of the previous studies conducted in Asia, Europe, and North America.18920 The prevalence increased with age in males, whereas it remained constant in females; this may be explained by a greater incidence of trauma and stroke—which are the leading causes of epilepsy—in males.21
The prevalence varied with age as a gentle U-shaped curve, with the prevalence being higher in children and the elderly. This pattern may reflect the remission of a considerable proportion of childhood epilepsies at adolescence22 and the increase in various brain pathologies with age. The prevalence was highest among young patients with Diagnosis-E, whereas the prevalence was U-shaped in patients without Diagnosis-E, which suggests that Diagnosis-E was assigned less frequently to elderly and pediatric patients with epilepsy. This is perhaps because symptomatic epilepsy is more common in these populations, particularly in elderly individuals, and only diagnostic codes for the primary underlying condition, such as stroke, head trauma, or neurodegenerative disease, were entered into the system. Physicians may defer coding epilepsy or seizure in children due to the social stigmatization and negative attitudes toward epilepsy.23
Our study was subject to several limitations. Because we used the HIRA database, and thus included only patients actively seeking medical attention, we were able to estimate the prevalence of treated epilepsy but not that of all epilepsy cases. This may have resulted in underestimation of the actual prevalence of epilepsy in Korea, although the treatment gap is anticipated to be minimal because of the high accessibility to health institutions and the 70–100% coverage of costs for AEDs in Korea. Another overlooked group was patients who used AEDs that were not recorded in the HIRA database; for example, patients who covered the costs themselves to avoid stigma and those who were reimbursed by means other than NHI, such as automobile insurance or industrial accident compensation. Our medical records survey was performed only at institutes that agreed to join the study, which could result in a selection bias in the estimation of diagnostic validity. In spite of these limitations, our study had strengths in that it was performed nationwide and covered the entire population, and the prevalence was estimated by diagnostic validation according to strata based on an extensive survey of medical records.
Conclusions
We have estimated the nationwide prevalence of epilepsy using claims data from administrative health database complemented by a medical records survey. We were able to calculate reliable age- and sex-specific prevalence, by applying stratified diagnostic validity from a medical records survey of a large number of samples. The overall prevalence was comparable to those found in other East Asian countries. The age-specific prevalence appeared as a U-shaped graph, being higher among the young and the elderly. Administrative health data may reveal variability in diagnostic validity according to the method of case ascertainment, age, and sex, and a significant number of treated patients with epilepsy may not show diagnostic codes for epilepsy or seizure. Our study may provide a basis for further epidemiologic studies using administrative health databases.


 XML Download
XML Download