

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The absence of the radius, regardless of its cause, leads to a radial club hand deformity.123456) There are considerable differences of opinion as to whether treatment of this condition is justified. Moreover, aggressive treatment of the traumatic absence of the radial shaft in children is of great clinical concern.6) Amid the continuing debate, we present our experience of aggressive and successful treatment by utilizing a modified Define's one bone forearm surgical procedure. Among the several reconstructive procedures, we chose the Define's procedure to minimize surgery considering the immediate post-traumatic condition of the right forearm and wrist.
Define's procedure is one of the several introduced reconstructive procedures. It consists of detachment of the lower end of the ulna from its periosteal sleeve and its displacement to the radial side of the carpus. We modified the Define's procedure and displaced the osteotomized distal end of the ulna to the remaining metaphysis of the distal radius instead of displacement to the carpus. This modification was to make a one bone forearm in the child; that is, osteotomizing the ulna at the distal metaphysis, detaching the distal end of the proximal ulnar fragment from its periosteal tube, and transposing its distal end to the remaining distal metaphyseal fragment of the radius (Fig. 1). The two bony fragments were stabilized with two thin Kirschner wires. Then, the detached periosteal tube was sutured for filling the tube with blood.
CASE REPORT
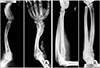
A 5-year-old boy sustained a pedestrian traffic accident on March 18, 1977, which resulted in the loss of the right radial shaft, severe soft tissue injuries to the extensor muscle belly, avulsion of the entire forearm skin with some skin loss, and elbow dislocation (Fig. 2). He was able to move his fingers. Wound debridement and reduction of the elbow were carried out on the day of admission, which was followed by skin graft. The wound was completely covered with the grafted skin, and infection was also controlled by the end of April. The radiograms taken on May 25, 1977 showed the preserved distal physis of the radius. Transposition of the distal end of the osteotomized proximal ulna shaft to the remaining distal metaphysis of the radius was performed on June 8, 1977 (Fig. 3).
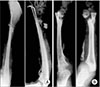
On the radiogram of the right forearm, taken 4 weeks after the reconstructive surgery, new bone formation in the ulna periosteal tube was shown, and complete bone reformation of the ulnar ray was seen 3 months after surgery. Hypertrophy of the ulna was seen 6 months later. At the time, the boy demonstrated almost normal right hand function with a stable wrist (Fig. 3A). Then, the boy was lost to follow up for a while. On January 5, 1979, the boy revisited the outpatient clinic complaining instability of the right wrist with degradation of right hand function. The radiograms taken on the day disclosed pseudoarthrosis at the metaphysis of the radial ray of the bifurcated single bone forearm (Fig. 3B). A periosteal corticocancellous graft harvested from his right tibia was grafted to the nonunion site on January 10, 1979 (Fig. 4). Radiograms of the right forearm, taken 6 months after bone graft disclosed solid union. Follow-up was continued until June 22, 1992 and at the final follow-up, normal wrist and hand function was restored. The forearm lengths of the normal left and the reconstructed right sides were 27.5 cm and 17.5 cm, respectively, at the age of 20 years (Fig. 5). However, there was no growth discrepancy between the radial and ulnar rays of the reconstructed one bone forearm, and no wrist deformity.
Informed consent was obtained from the patient for publication of this case report.
DISCUSSION
Pulvertaft stated that the ideal treatment for the congenital absence of the radius was the correction and freedom from splintage at an early age in order to enable the child to develop a functional pattern of the hand.4) The correction should be complete and permanent without disturbance of growth and loss of wrist movement. Unfortunately, to date this ideal has not been achieved. Surgical methods described thus far also fall short of this ideal in one way or another.
Although many types of surgery have been used for congenital absence of the radius, definitive methods have yet to be established.12356) It is known that prerequisites of the Define's procedure are a reasonably good proximal end of the ulna, a good elbow, and a reasonably good distal end of the radius and radiocarpal joint.6) Before surgery, we were ensured that a bone would form in the well vascularized periosteal tube of the ulna of the child. As Bosworth et al.7) mentioned, one could expect complete regeneration of the lost segment after tibial diaphysectomy by periosteal flap in children younger than 8 years of age. Also, Moon and Kim8) reported bony regeneration in the diaphysectomy defect of the proximal tibia via periosteal osteogenesis for management of chronic osteomyelitis of the tibia in a young adult.
The surgical procedure that includes suture of the longitudinally incised hallow periosteal tube of the ulna together with external immobilization is thought to invite osteogenesis of ulnar ray and successful formation of two rays, thus providing good results. We believe that postoperative external immobilization for a certain period of time plays a key role in periosteal osteogenesis, and thus its importance should be stressed.
Pseudoarthrosis or delayed union can develop at the radial ray as in the current case due to deficient periosteum and poor vascularity of the transposed denuded ulna. Therefore, a periosteocorticocancellous graft seems to be desirable at the time of transposition of the distal end of the osteotomized proximal ulna to the remaining distal metaphysis of the radius in order to obtain good osteogenesis and solid bony union.
Longitudinal growth of the radial and ulnar rays by the distal physis did not occur as much as we had expected during the growth period in our current case. As a result, there was no longitudinal growth discrepancy between radial and ulnar rays. If one of the two rays had continued to grow in excess longitudinally, then the initial success of surgery might not have been sustained because of the radial or ulnar tilt of the hand. Our main treatment goal was to correct the deformity and to restore functions of the forearm, wrist, and hand as much as possible. The procedure described in this report appears to have fulfilled this objective. Forearm shortening did not affect hand function. The disadvantage of this procedure was no restoration of pronation-supination movement.
A case of traumatic absence of the entire radial shaft in a child is presented. The child's forearm was successfully reconstructed by a modified Define's procedure. This simple reconstructive surgical procedure can be considered an effective method of treatment as it improves the function as well as appearance of the hand.



 XML Download
XML Download