

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Antibiotic resistance in gram-negative bacteria is a major problem worldwide. Resistance to β-lactam antibiotics is often mediated by β-lactamases, including expanded-spectrum β-lactamases (ESBLs), plasmid-mediated AmpC β-lactamases, and carbapenemases [1]. Clinical isolates of Klebsiella pneumoniae are notorious for harboring a wide range of β-lactamases and are naturally resistant to ampicillin and amoxycillin. β-Lactam antibiotics are often used in the treatment of infections caused by this bacterium [2]. The emergence and rapid spread of drug-resistant K. pneumoniae isolates has become a serious clinical challenge.
β-Lactamases are grouped into four classes according to their amino acid sequence: class A, including KPC and TEM; class B, the metallo-β-lactamases (MBLs) such as VIM, IMP, and NDM-1; class C, the AmpC β-lactamases; and class D, the oxacillinase (OXA)-type enzymes. All four classes of β-lactamases have been described in K. pneumoniae. Carbapenem resistance in K. pneumoniae has been reported in most countries and can be attributed to plasmid-mediated AmpC cephalosporinases associated with porin modifications [34], reduced outer membrane permeability by porin loss in combination with the production of an ESBL, or production of β-lactamases capable of hydrolyzing carbapenems (carbapenemases) [56]. In Turkey, OXA-48 carbapenemases have been identified for a decade [5], initially described in K. pneumoniae [7] and then in various other enterobacterial species [8910]. Only recently, however, an imported case of NDM-1-producing K. pneumoniae has been reported in Turkey [11], but thus far, there have been no reports on locally acquired cases.
In this study, we aimed to characterize the β-lactamases in carbapenem-resistant K. pneumoniae clinical isolates from Turkey. These data serve an important role in understanding and controlling the spread of carbapenem-resistant gram-negative pathogens [2].
METHODS
1. Bacterial strains and antibiotic susceptibilities
The study was performed at the Bezmialem Vakif University Hospital in Turkey between July 2012 and March 2013. During the study period, all non-duplicate clinical isolates of K. pneumoniae obtained from inpatients that exhibited a reduced sensitivity to carbapenems were characterized. Clinical isolates were identified by using standard microbiological procedures and VITEK-2 (bioMerieux, Marcy-l'Etoile, France). The identification of all isolates was confirmed by 16S rDNA sequencing [12]. Susceptibility testing was performed by using the following antibiotics: ampicillin, ampicillin/sulbactam, piperacillin, piperacillin/tazobactam, cefuroxime, ceftazidime, cefoperazone/sulbactam, cefepime, amikacin, gentamicin, netilmicin, tobramycin, ciprofloxacin, levofloxacin, tetracycline, trimethoprim/sulfamethoxazole, imipenem, meropenem, colistin, and tigecycline. Non-susceptibility to carbapenems (imipenem and meropenem) and colistin during susceptibility testing was confirmed by E-test (bioMerieux) in accordance with the CLSI guidelines [13].
2. Detection of β-lactamase genes
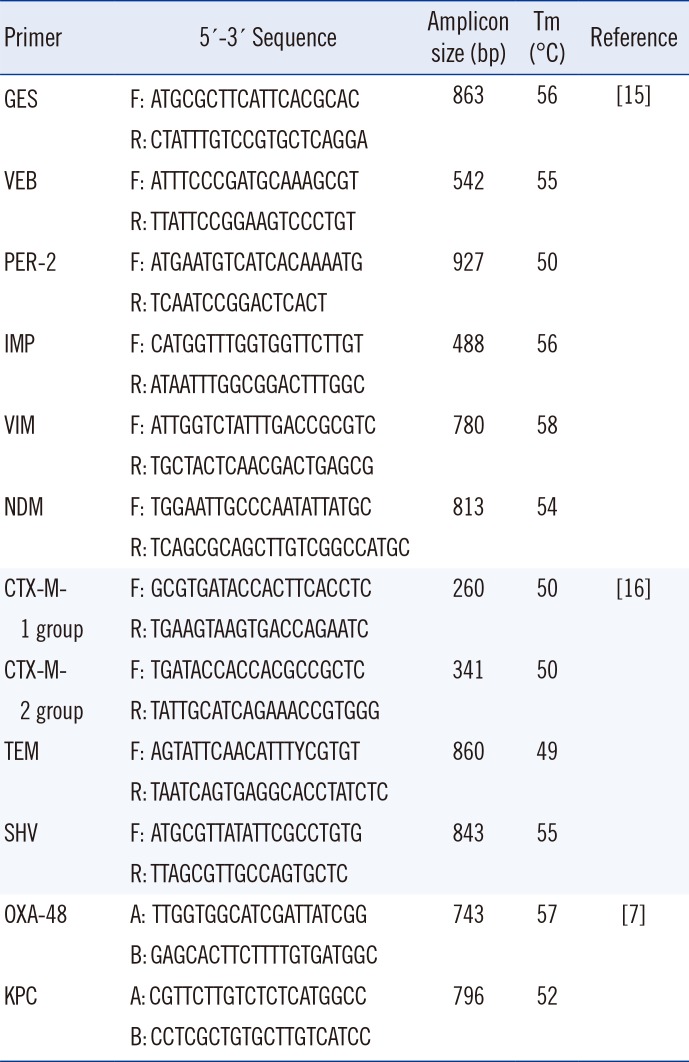
K. pneumoniae strains were screened for β-lactamase-encoding genes by PCR. The primers used to amplify the blaSHV, blaTEM, blaCTX-M1, blaCTX-M2, blaGES, blaVEB, blaPER-2, blaNDM-1, blaIMP-like, blaVIM-like, blaKPC and blaOXA-48 genes are listed in Table 1. A single reaction mixture contained 5 µL genomic DNA, 20 pM of each primer, 10 µL reaction buffer, 3 µL 25 mM MgCl2, 200 µM dNTPs, and 1.5 U Go Taq Flexi Polymerase (Promega, Madison, WI, USA), in a final volume of 50 µL. PCR amplification was performed by using standard conditions with varying annealing temperatures (Table 1). All PCR results were analyzed on 1% agarose containing 0.5 µg/mL ethidium bromide and subsequently visualized under UV light. The PCR products for NDM, OXA-48, and TEM β-lactamases were cloned into the pGEM-T Easy vector (Promega) and then sequenced by Macrogen (Amsterdam, The Netherlands). Sequencing results were analyzed by using the alignment search tool, BLAST (http://www.ncbi.nlm.nih.gov/BLAST) [14], and the multiple sequence aligment program CLUSTALW2 (http://www.ebi.ac.uk/Tools/msa/clustalw2/). The remaining genes were evaluated according to their molecular size and PCR results of control groups which were defined as β-lactamase gene carrier bacteria in the earlier studies [71516].
3. Repetitive Extragenic Palindronic (REP)-PCR analysis
REP-PCR was used in the genotyping of K. pneumoniae isolates. The primer pair REP 1 (5'-IIIGCGCCGICATCAGGC-3') and REP 2 (5'-ACGTCTTATCAGGCCTAC-3') was used [17], and the amplification reaction was performed as previously described [15]. The amplified DNA fragments were separated by electrophoresis on a 1.5% agarose gel with a 1-kb DNA ladder (Sigma Chemicals, Ontario, Canada) as the size marker. The amplified DNA bands were visualized under UV light following ethidium bromide staining, and the banding patterns of each strain were captured by using an UVP bioimaging system (UVP, Upland, CA, USA). The REP-PCR fingerprints were analyzed by using the Phoretix gel analysis package (Nonlinear USA, Inc., Durham, NC, USA).
RESULTS
A total of 37 K. pneumoniae isolates were identified during the study period and investigated. All isolates were from hospital-acquired infections, with the majority from patients in the intensive care unit (n=23), followed by patients on surgical (n=7) and medical wards (n=7). Of the 37 isolates, 16 (43%) were associated with bloodstream infections. The remaining isolates came from wounds (n=7, 19%), sputum (n=6, 16%), tracheal aspirates (n=6, 16%), cerebrospinal fluid (n=1, 3%), and a catheter sample (n=1, from anesthesia unit).
According to the antibiotic susceptibility profiles, all 37 isolates were resistant to ampicillin, ampicillin/sulbactam, piperacillin, piperacillin/tazobactam, ceftazidime, cefoperazone/sulbactam, cefepime, imipenem, and meropenem. The lowest levels of resistance were observed for colistin (2.7%) and tigecycline (11%), followed by amikacin (19%) and trimethoprim/sulphamethoxazole (21.6%). Of the 37 K. pneumoniae isolates, 98% carried a carbapenemase gene. More specifically, we detected OXA-48 in 32 isolates (86%) and NDM-1 in seven isolates (19%). No other carbapenemases were identified within this group. We also observed a high prevalence of ESBLs, with all strains carrying a CTX-M-2 group β-lactamase and 23 isolates (62%) carrying CTX-M-1. SHV-1-like and TEM-1-like β-lactamase were also common (97% and 92% of strains, respectively). One of the blaTEM genes was identified as blaTEM-166, a variant of blaTEM-1b that has one amino acid change at position 53 (Arg53Gly).
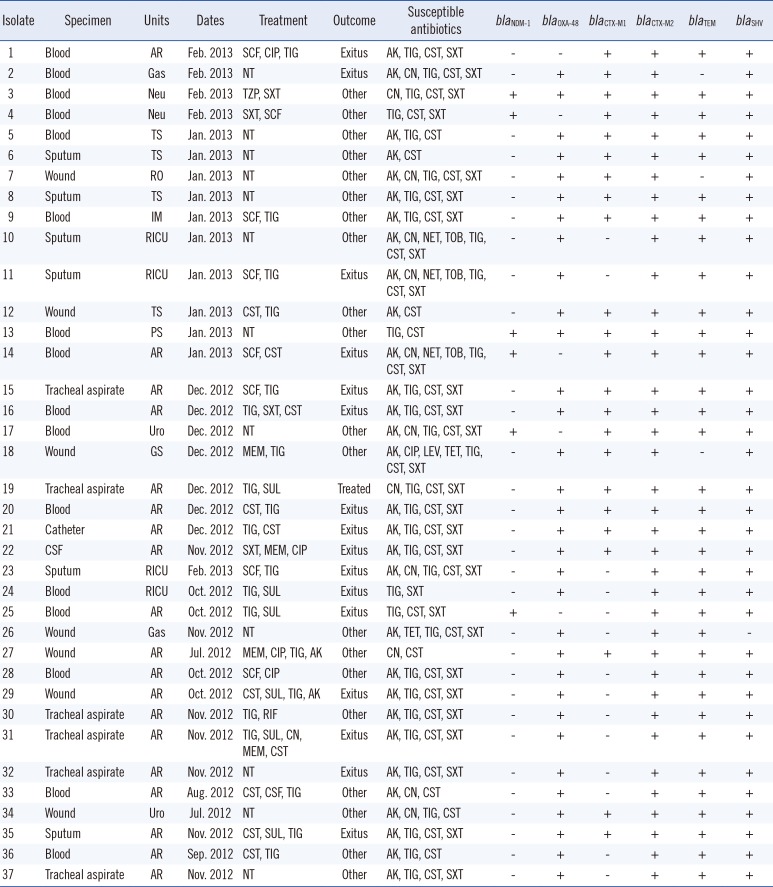
The combination of β-lactamases relative to the site of isolation and susceptibility test results are shown in Table 2. Importantly, all NDM-1-producing strains were isolated from blood. Furthermore, all blood isolates carried at least one carbapenemase (OXA-48 or NDM-1), and two (13%) carried both OXA-48 and NDM-1. The most common combination of β-lactamases in a given strain was OXA-48, SHV-1-like, TEM-1-like and CTX-M-type β-lactamase, with 76% of strains observed with this combination.
All 37 K. pneumoniae strains were typed by REP-PCR (Fig. 1). We observed seven predominant genotypes; the majority of strains (46%) clustered into genotype 6, while 19% and 16% of the isolates clustered in genotype 3 and 1, respectively. Of the 17 genotype 6 isolates, 11 were isolated from the anesthesia and reanimation intensive care unit (ICU), and three were isolated from the thoracic surgery unit. Of the seven genotype 3 isolates, two were isolated from patients who were in the neurology ward at the same time, and two were isolated from the anesthesia and ICU. The remaining isolates were distributed among other wards in the hospital over different times during the 9-month study period (Table 2).
DISCUSSION
K. pneumoniae is an opportunistic pathogen that causes community- and hospital-acquired infections, such as bloodstream and urinary tract infections, and pneumonia [18]. Currently, carbapenems are the most potent antimicrobial agents used in the treatment of serious infections caused by multidrug-resistant gram-negative bacteria. However, carbapenem resistance in Enterobacteriaceae is emerging in Turkey [89] and in other parts of the world [5]. Here, we described the distribution of major β-lactamases in a contemporary group of extensively drug-resistant K. pneumoniae isolates from Turkey. We observed that 19% of isolates carried the NDM-1 carbapenemase, and that all of these isolates came from bloodstream infections and from patients with no recent travel history, suggesting local acquisition. OXA-48 carbapenemases were highly prevalent, and were occasionally found co-existing with NDM-1. Compounding these data was that over 2.7% of isolates were resistant to colistin, a finding that is novel for Turkey and one with serious therapeutic implications. The majority of isolates came from patients in the ICU.
BLs have been reported worldwide, and their genes are often located on plasmids and integrons [19]. NDM is a novel MBL enzyme, and its variants are the latest carbapenemases to be recognized and reported worldwide. NDM-1 was first identified in a carbapenem-resistant K. pneumoniae strain from the urine sample of a Swedish patient of Indian origin who traveled to New Delhi [20]. Since then, more than 40 countries have reported NDM-producing isolates [2122]. NDM enzymes have predominately been identified in Enterobacteriaceae, but have also been described in non-fermenters and in members of the Vibrionaceae family [23].
Occasional community-acquired NDM-1-positive isolates have been reported [24], however, the overwhelming majority of isolates have a nosocomial origin. In our study, all isolates were from nosocomial infections and all were from seriously ill patients. All of the NDM-1-positive isolates (n=7) were recovered from blood samples, and six of these were from patients in the ICU. All patients were uninfected at admission, and the organisms were isolated from patients 48 hr or longer after admission.
In Turkey, NDM-1 was first reported in 2011 in a K. pneumoniae isolate from a leukemia patient originally from Iraq [19]. Later, another team investigated NDM-1 in various carbapenemase-resistant gram-negative bacilli, but with negative results [25]. To our knowledge, the current study is the largest report demonstrating the presence of NDM-1 in K. pneumoniae in Turkey. Our results indicate that seven out of 37 (19%) carbapenem-resistant K. pneumonia isolates were positive for NDM-1, an alarming result as efforts to identify NDM-1-producing isolates in 2011 showed negative results.
Another β-lactamase type known as OXA-48 was initially identified in Turkey from a K. pneumoniae isolate from Istanbul, and thereafter, outbreaks of OXA-48-producing K. pneumoniae have been described in Turkey [8910]. To date, 11 variants of OXA-48 have been described [26]. Recently, the molecular characterization of carbapenem-resistant K. pneumoniae in a tertiary university hospital in Turkey was performed on 94 isolates. OXA-48 and NDM-1 were produced in 91.5% and 4.3% of isolates, respectively [27]. In our study, OXA-48 and NDM-1 were observed in 86% and 19% of isolates, respectively. This study reveals that the NDM-1 resistance gene is increasing in prevalence in Turkey. This increase poses a significant threat to Turkish infection control efforts.
TEM or SHV β-lactamase derivatives have been the most prevalent ESBLs in nosocomial pathogens since the 1980s. However, starting from 1995, CTX-M-type ESBLs have emerged worldwide, including Europe, Asia, South America, and Canada [1328]. We demonstrated that these CTX-M-type ESBLs are also highly prevalent in multidrug-resistant K. pneumoniae in Turkey. In a multicenter study conducted in Turkish hospitals, PCR analysis was used for ESBL typing, and CTX-M was the most prevalent enzyme type among blood isolates (71%) of Escherichia coli and K. pneumonia, followed by TEM (49%) and SHV (47%) type enzymes [29].
The CTX-M family can be classified into five major groups: CTX-M-1, CTX-M-2, CTX-M-8, CTX-M-9, and CTX-M-25. CTX-M-15, which belongs to the CTX-M-1 group, is the most widespread of these enzymes around the world [30]. Ours is the first report of CTX-M-1 and CTX-M-2 in ESBL-producing carbapenem-resistant K. pneumoniae strains from Turkey. CTX-M-2 was the most prevalent β-lactamase, found in 100% of isolates, followed by SHV (97%), TEM (92%), and CTX-M-1 (62%). The continued monitoring of antimicrobial resistance to β-lactams in each region of Turkey is urgently required to assist with the development of control strategies for hospital infections.
In conclusion, our study of carbapenem-resistant, K. pneumoniae isolates identified the largest number of NDM-1-producing strains reported from Turkey, and revealed that these strains were highly resistant to a range of clinically important antibiotics. Furthermore, these isolates often carried the OXA-48 carbapenemase, and were associated with serious infections of the bloodstream. All strains also carried multiple ESBLs, with blaCTX-M-2 being the most common. The recent emergence of NDM-1-producing K. pneumoniae on the background of the highly prevalent OXA-48 and CTX-M type ESBLs is alarming for our country.

 XML Download
XML Download