

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The success of endodontic treatment depends on both good apical and coronal sealing. This sealing prevents residual bacteria and their endotoxins from reaching the root apex, otherwise possibly leading to treatment failure [12]. For this reason, different techniques and materials have been extensively studied to enhance the performance of fillings and restorations of endodontically treated teeth [345].
Considering the extensive coronal destruction of most teeth requiring endodontic treatment, intraradicular glass fiber posts have frequently been used to keep these teeth in the oral cavity for a longer time. This type of post has been found to be a viable alternative in meeting today's greater aesthetic demands, especially because of its properties, such as modulus of elasticity similar to dentin [6], flexibility [7], and translucency [8].
The most widely used material for cementation of fiberglass posts is resin cement. Considering that this is an adhesive material, the retention of fiberglass posts when cemented with this material depends both on the characteristics of the cementing agent [9] and on the morphological characteristics of the intraradicular dentin [1011].
The smear layer is a substrate of nonhomogeneous structure loosely adherent to the root canal walls composed of organic and inorganic particles, coagulated proteins, pulp tissue, blood cells, bacteria, and fungi [12]. The smear layer may be a factor supporting the persistence of infection, because of the organic and inorganic substrates in its composition. Therefore, it can compromise the intratubular penetration of endodontic sealers [13] and the adhesiveness of luting cements [14]. For these reasons, its removal with chemical substances has been advocated.
The most commonly used irrigating solutions for endodontic treatment are sodium hypochlorite (NaOCl) and chlorhexidine (CHX) [12]. These are used more specifically because of their antimicrobial properties; however, neither can remove the smear layer effectively. The solution most frequently used to remove the smear layer is ethylenediaminetetraacetic acid (EDTA) [12]. However, the vast majority of studies have demonstrated the inability of any of these solutions to completely remove the smear layer, especially when used passively (without any type of activation) [15]. For this reason, ultrasonic activation has been proposed to remove the smear layer. This technique is based on the premise that the energy released by the instrument improves the physicochemical properties of the irrigation solutions by cavitation and transmission of acoustic waves [1617].
Considering that only a few studies, to date, have evaluated smear layer removal after preparation for cementation of intraradicular posts, the objective of this paper was to evaluate this variable, comparing different chemical solutions used with or without ultrasonic activation.
MATERIALS AND METHODS
Selection and preparation of the sample
After approval by the Research Ethics Committee of the Londrina State University (310.888/2013), 45 human lower premolars with a single canal and a completely formed apex, without previous endodontic treatment or anatomical complexities, were selected. These teeth were extracted for periodontal reasons or by orthodontic indication, from patients with ages ranging from 20–40 years. After extraction, the specimens were kept in 0.1% thymol solution until the moment of use. Before performing the instrumentation, the crowns were removed using a low-speed steel cutting disc (Isomet, Buehler, Lake Bluff, IL, USA), standardizing all roots at 15 mm in length.
Instrumentation
Initially, the entrance orifice of the canal and the cervical and middle thirds were prepared using Largo No. 2 (Dentsply Maillefer, Rio de Janeiro, RJ, Brazil) and No. 4, 3, and 2 Gates Glidden drills (Dentsply-Maillefer, Ballaigues, Switzerland), respectively, according to the crown-down technique. The working length was determined by inserting a size 15 Flexo-File (Dentsply-Maillefer) up to the apical foramen, and subtracting 1 mm from this measurement.
The K3 system (SybronEndo, Scafati, Italy) was used for instrumentation, with a file of size 55/0.04 as the final instrument. An amount of 2.5 mL of 2.5% NaOCl (Formula e Ação, São Paulo, SP, Brazil) was used at change of each file, using disposable syringes and 30 G NaviTip needles (Ultradent, South Jordan, UT, USA) calibrated at 1 mm short of the working length. The root canals were dried with absorbent paper cones (Tanari, São Paulo, SP, Brazil), and filled using the lateral condensation technique and Fillapex sealer (Angelus, Londrina, PR, Brazil). Next, the specimens were stored at 37°C and 100% humidity for 7 days to allow the sealer to set.
Filling removal for post cementation
The filling material was removed from the cervical and middle thirds using No. 2 Largo drills (Dentsply Maillefer, Brazil) calibrated at 10 mm. The canal was then prepared using a drill compatible with the diameter of the No. 2 fiberglass post from the Exacto system (Angelus), and the specimens were radiographed.
Afterwards, the root canals were irrigated according to the experimental groups (Table 1), using disposable syringes and 30 G NaviTip needles (Ultradent). In the groups where ultrasonic activation was performed, a 0.20 mm cylindrical insert (Irrisonic, Helse, São Paulo, SP, Brazil) was coupled to the device (Profi Class, Dabi Atlante, São Paulo, SP, Brazil) and activated at a power of 20% for 60 seconds, except on the G8 specimens where the activation was performed for only 20 seconds. The final irrigation was performed with 5 mL of 0.9% saline solution (NaCl) in all the groups except for the G1 specimens. Afterwards, the canals were dried again using absorbent paper points (Tanari).
Table 1
Experimental groups according to chemical solution and irrigation method
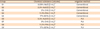
NaCl, saline solution; NaOCl, sodium hypochlorite; CHX, chlorhexidine; PAA, polyacrylic acid; EDTA, ethylenediaminetetraacetic acid; PUI, passive ultrasonic irrigation.
*Halex Istar Indústria Farmacêutica Ltda, Goiânia, GO, Brazil; †Asfer Ind. Quim. Ltda, São Caetano do Sul, SP, Brazil; ‡FGM Produtos Odontológicos, Joinville, SC, Brazil; §DFL Indústria e Comércio Ltda, Rio de Janeiro, RJ, Brazil; ∥Biodinâmica Química e Farmecêutica Ltda, Ibiporá, PR, Brazil.
![]()
Scanning electron microscope (SEM)
Initially, longitudinal grooves were made in the buccolingual direction with a double-faced flexible diamond disc (KG Sorensen, Barueri, SP, Brazil), and the final cleavage was achieved using a pair of cutting pliers to expose the root canal. Afterwards, the hemisections were fixed in circular metal stubs to perform the metallization process. At this stage, the specimens received a surface layer of gold, about 30 nanometers thick, using the Quorum Q150R ES device (Quorum Technologies, Ashford, Kent, England).
Three SEM images at × 2,000 magnification were obtained for each radicular hemisection, using a SEM (VEGA 3, Tescan, Brno, Czech Republic). These high magnification SEM images corresponded to the apical, middle and cervical portion of the prepared canal, 2, 5 and 8 mm short of the remainder of the filling material, respectively. The images were evaluated by a previously calibrated endodontist blinded to the research objectives. Only one score for the amount of smear layer was assigned to each image of each third (Table 2 and Figure 1) [18]. For each specimen, 3 images and 3 scores were obtained totaling 15 scores per group and 135 scores in total.
Table 2
Criteria for scoring the presence or absence of smear layer on the surface of the root canal or in the dentinal tubules

![]()

RESULTS
EDTA was found to have the highest smear layer removal ability, regardless of the irrigation method (with or without ultrasonic activation) (p < 0.05). In addition, the use of ultrasonic activation did not significantly influence smear layer removal when the same solution was used (G2 = G5, G3 = G6, G4 = G7, and G5 = G9, Table 3).
Table 3
Absolute and relative frequency of assigned scores in different groups
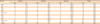
a–nThe same superscript letters indicate statistically significant difference among the groups (Mann-Whitney U test; p < 0.05).
![]()
DISCUSSION
When fiber posts and resin cements are used to restore endodontically treated teeth, dentin adhesion results from the micromechanical retention created by the demineralized dentin surface associated with the formation of resinous tags [19]. Therefore, the cleaning of the root canal wall is a critical procedure to ensure successful treatment [20]. The objective of the present study was to evaluate the removal of the smear layer after preparation for cementation of intraradicular posts, comparing different chemical substances used with or without ultrasonic activation.
SEM has been the most widely used methods to evaluate the removal of the smear layer [101517182122]. However, one of the main drawbacks related to this methodology is that the SEM allows the evaluation of only reduced areas, without considering the entire area of the root canal. Nevertheless, in the present study, the evaluation focused only on the area corresponding to the cervical and middle thirds. This area was divided into three segments (apical, medial, and cervical) and, because of the dimensions of the instrument used to prepare the intraradicular post, the total area for analysis of each segment was kept to about 1.1, 1.4 and 1.4 mm2, respectively. For this reason, we believe that it was possible to obtain representative images of the general context. Even so, we believe that further studies with similar methodological designs are needed using more complete analysis tools, such as microcomputed tomography.
Just like the results obtained in previous studies, those of the present study also showed that EDTA performed better than NaOCl [2123] and CHX [2224]. Although NaOCl is effective in dissolving the organic matter of the smear layer, it does not act effectively on the inorganic portion of this layer [12]. On the other hand, CHX is unable to dissolve organic matter, thus also compromising its smear layer removal ability [12222425].
In addition, no significant statistical differences were found between groups 5 and 9; that is, the use of ultrasonic activation did not potentiate the effects of EDTA. These results differ from those found in other studies [1521]. Kuah et al. [15] evaluated smear layer removal promoted by 17% EDTA with or without ultrasonic activation for 1 and 3 minutes, and observed that the use of ultrasonic activation was able to potentiate the action of this solution. Lui et al. [21] evaluated smear layer removal by comparing Smear Clear (17% EDTA and surfactants) and 17% EDTA used with or without ultrasonic activation. According to the authors, the addition of surfactants to EDTA did not potentiate the removal of the smear layer. However, ultrasonic activation provided more favorable results, especially when 17% EDTA was used. However, 2 main points need to be taken into consideration. In both of the studies cited [1214], removal of the smear layer was evaluated after instrumentation, whereas, in our study, removal followed preparation for cementation of the intraradicular posts [2627]. In addition, Lui et al. [21] used 75 specimens divided into 5 groups (n = 15), and Kuah et al. [15] used 105 specimens divided into 7 groups (n = 15). In the present study, only 45 specimens were used and divided into 9 groups (n = 5). The use of fewer specimens per group may have influenced the results obtained, and this represents a limitation of this study.
Although polyacrylic acid (PAA) was not used conventionally in the intraradicular space, it was included in this study, considering its indication in dentin conditioning to potentiate adhesiveness [2829]. The results showed that PAA was less effective than EDTA in removing the smear layer. Because PAA is a weak acid with high molecular weight, it only managed to disorganize the smear layer and not remove it effectively [30]. In addition, the action of PAA was not enhanced by the use of ultrasonic activation. This result was already expected, due to its consistency in gel form. However, PAA was used for 20 seconds in this study, according to the manufacturer's recommendations for restorations with glass ionomer cement. Therefore, we believe that further studies are needed to analyze the removal of the smear layer using the PAA for a longer period, considering that root dentin is more mineralized and sclerotic than the coronary dentin [3132], for which this material has presented satisfactory results [2829].
As mentioned previously, considering the particular characteristics of each substance used in the experimental groups of the present study, ultrasonic activation overall, failed to potentiate removal of the smear layer. Another point to consider is the activation method used. In the present study, ultrasonic activation was used for 20 seconds on G8 specimens and for 60 seconds on the specimens from the other groups. Ultrasonic activation at faster cycles produces a cumulative effect on debris removal [33] and facilitates keeping the tip of the activated instrument in a centralized position in the root canal, thus avoiding its contact with lateral root walls [34]. Therefore, in this study, the use of continuous activations may have led to not observing any advantages to using ultrasonic activation for smear layer removal in all the groups.
 XML Download
XML Download