

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Dental maturation and emergence have long been recognized as among the most useful criteria for age estimation.1 This approach is made more favorable by the facts that teeth are less affected by environmental factors and by hormonal systems than bones, and that most of the techniques used are noninvasive and simple to use.2 Prediction of dental age is required in several clinical and scientific disciplines such as orthodontics, pediatric dentistry, archeology, paleodontology, and forensic dentistry. Thus far, many different techniques have been developed, giving results with various levels of accuracy and using different statistical procedures for age estimation, according to tooth formation and eruption (gingival, alveolar) in children and adolescents.3 In these studies, tables for dental age estimation were formed according to mineralization stages and eruption positions in various age groups. These techniques were specific to the populations in which they were developed and might be misleading for other populations.4,5 In two of the early studies, it was reported that the Demirjian technique, which was developed on the basis of French-Canadian children, considerably overestimated the dental age for Turkish children.6,7 These studies indicated that dental development varied between and among different populations, making population-specific studies necessary.
For many years, dental charts prepared from population surveys have been used to determine the ages of individuals for orthodontic and forensic purposes and have been regarded as sufficiently accurate to estimate the actual age of a juvenile or young adult.8 Pedodontists and orthodontists need to know a child's growth, developmental status, and dental age, which are particularly significant for diagnosis and treatment planning.9,10 Dental charts that are prepared according to specific age groups can provide this information.8 In addition, it is known that the atlas method is very effective and efficient, particularly for the identification of juvenile victims in mass fatalities.11
There have been few atlases providing knowledge relative to dental development and eruption. When the historical use of atlases constructed for dental age estimation was researched, Logan and Kronfeld's study was found to be important with respect to a study reporting the first histological sections presenting the order and stages of tooth development.12 The best-known diagrams in the atlas form belong to Schour and Massler.13 Subsequently, with the addition of new materials referenced in dental age estimations, more updated atlases were put into use.14,15 Finally, the London atlas by AlQahtani et al16 was released, containing more charts specifically designed for use in mass fatalities, followed by additional charts by Blenkin and Taylor,17 which were constituted specifically for Australian children. Without question, every single atlas gives the most reliable results for its reference population. For this reason, there is a need for more population-specific charts.
In this study, the aim was to develop dental charts for use in Turkish children and young adults of both genders within the age group of 4.5-22.5 years, according to tooth mineralization and eruption in a format similar to that proposed by AlQahtani et al.16
Materials and Methods
This study was designed as a retrospective cross-sectional evaluation of digital panoramic radiographs (DPRs), which were obtained for clinical purposes from consecutive patients with known dates of birth; these patients were followed up in Istanbul Hospital, Dental Unit, in Istanbul, Turkey. The patients, who resided in the Marmara region (the northwest of Turkey), had similar phenotypic features and were also known to have similar ethnic origins. Ethical approval for the study was received from the Istanbul University, Cerrahpasa Medical Faculty, Ethics Committee. Radiomorphological assessments were performed on 753 DPRs obtained from 350 males and 403 females (Table 1). Radiographs that were unclear or that showed any conditions such as hypodontia, gross pathology, failure of eruption, previous orthodontic treatment, history of systemic diseases, growth and development retardation, and insufficient nutrition were excluded. These data were obtained from clinical records. Microsoft® Office Excel® 2010 (Microsoft Corp., Redmond, WA, USA) was used to calculate the chronological age from the difference between the X-ray date and the patient's birth date. Furthermore, the age groups were determined by considering the midpoints of each age interval (age group 5, 4.50-5.49 years; age group 6, 5.50-6.49 years; age group 7, 6.50-7.49 years, etc.). Thus, 18 age groups were formed for both genders.
The first author with 7 years of experience in assessing mineralization and eruption stages performed all DPRs assessments with appropriate magnification and contrast adjustment on all deciduous and permanent teeth on the left half of the maxilla and the mandible. When a problem was encountered for any reason in the assessment of one of the teeth, the tooth's counterpart on the other side was used. The permanent teeth were evaluated by the classification system described by Demirjian et al18 in eight stages, which we separated further into H stages, namely H1 (root length was complete, apical walls were converging, and approximately 1/2 of the apex closed) and H2 (apex was closed), thus modifying the system to have nine stages (Fig. 1).
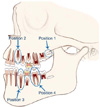
Root resorption on deciduous teeth in the mixed dentition period was evaluated with Moorrees' system,19 modified by AlQahtani et al16 in four classification stages (Ac, apex closed; Res1/4, resorption of the apical quarter of the root; Res1/2, resorption of half the root; and Res3/4, resorption of three-quarters of the root). Eruption position was assessed with Bengston's system20 modified by AlQahtani et al,16 with alveolar bone eruption of the teeth considered in four positions (Fig. 2). After the assessment of the developmental and eruption stages, the median was identified from the minimum to the maximum stages for each stage and for each tooth. To find the median value, the mineralization and eruption stages were first determined according to their rating for each tooth, after which the data were sorted according to their value after all DPRs in that age range had been evaluated. The number in the middle was then chosen as the median value. That is, supposing that there were seven DPRs in the age group of 5 years and that the Demirjian stages of the first premolars were B, C, C, C, C, D, and D, then, the median value became the C stage. These medians were used to construct dental diagrams for both genders.
During the preparation of the dental charts, every stage of the permanent and deciduous teeth, independently, was drawn and colored by a medical illustrator in a computer environment with the aid of Adobe® Photoshop® CS3 (Adobe Systems Inc., San Jose, CA, USA). Similarly, the left halves of the maxilla and the mandible were drawn. Teeth in these new dental charts imitate the radiographic presentation for permanent teeth; the color of dentin is fawn with the pulp area dark brown and the enamel white, while for deciduous teeth, dentin is yellow with the pulp area orange and enamel white. The stages of tooth development (median stage) described above, according to the developmental and alveolar eruption criteria were placed on a drawing of an edentulous jaw in the Adobe Photoshop environment. In the dental charts, which illustrated tooth development and eruption, a different jaw drawing was used from the onset of the third molar tooth development (10 age groups). Thus, new dental charts were formed for both genders and for all age groups evaluated.
Intra- and interobserver reliabilities were tested by the re-examination of 50 radiographs after four weeks. The DPRs were randomly chosen from the total sample and re-assessed by an observer who was blinded. The same radiographs were rated by the other observer. In order to calculate the intra- and interobserver agreements, Cohen's kappa test was carried out.
Results
Intra- and interobserver reliabilities for mineralization, eruption, and resorption stages indicated substantial agreement according to Landis and Koch21 (Table 2).
The sample size was 753, which was divided for convenience into 18 age groups at 1-year intervals. The determined midpoints of each age interval (age groups) were very close to the age means of the radiographs belonging to these intervals.
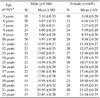
The teeth generally developed earlier in females than in males. This was particularly notable in the age group of 5-14 years. However, this difference was usually in only one stage and not in all teeth (Tables 3 and 4).
The mandibular permanent teeth developed more quickly than the maxillary permanent teeth, in both genders. It was observed that the greatest difference was in the incisors with respect to the tooth development in both jaws.
It was seen that females preceded males in the eruption of permanent teeth and root resorption of deciduous teeth, as generally occurred in mineralization during dentition (Figs. 3 and 4). It was determined that the mixed dentition period ended with the shedding of the second deciduous molars in both genders (Figs. 3 and 4). In the following period, it was observed that tooth eruption except that of the third molars was completed after the age of 12.5 years in both genders.
After the age of 14.5 years, the third molar maturation showed similar developmental patterns. This was also the tooth with the most variation among individuals in the same age groups. In both genders, the third-molar crypt began to form at the age of 8 years. It was also observed that the third molars completed their crown calcification in the age group of 13-14 years. When the minimum and the maximum tooth values except those for the third molars were evaluated in terms of formation and eruption, it was observed that they did not deviate much from the median values. However, considerably more variation was seen in the third molars. Gender differentiation was observed as either one mineralization stage variation or none; however, in three different age groups, more variations were observed, including two maxillary and one mandibular third molar variation (Table 5).
Discussion
Knowledge of the development and eruption stages of permanent teeth is essential for clinical practice in dentistry and forensic disciplines.22 Tooth formation has been widely used for the evaluation and calibration of growth and maturity.2 This information helps us to compare the status of dental maturity in our population with that in previously tested populations. In some fields of dentistry, clinicians frequently use this information, particularly for the treatment of orthodontic patients, for the diagnosis of dental eruption in children, and for surgical interventions. Awareness of a patient's growth potential is one of the most important factors determining the success of orthodontic treatment.23 The dental diagrams generated as a result of this study provide valuable information on resorption, eruption, and mineralization for the age group of 4.5-22.5 years. This application is practical and useful because it is based on the comparison of panoramic images, which are often applied during routine practice, and dental charts. In addition, dental charts offer rapid and practical solutions to problems of dental age estimation for children and young adults, to aid in the identification of disaster victims, particularly by inexperienced investigators.11 The advantages of using this system to estimate the age of an individual are that it is simple and does not require any specialized training to recognize specific stages; further, it does not require the use of specialized equipment beyond the X-ray apparatus.17 However, dental age estimation systems that are atlas-based have some limitations.24 In the atlas-style age estimation technique, specific charts are formed for certain ages. Therefore, the accuracy of the estimation is less accurate than that of other traditional age estimation methods, which give results at the decimal level. For more precise age estimations, traditional methods should be applied.
The charts presented here are in a format similar to the atlas compiled by AlQahtani et al.16 However, the classification system in which tooth development was evaluated is different. These dental charts are specific to every age, illustrating tooth formation and eruption and drawn in a digital environment by digital drawing techniques. The drawings constructed in this manner are more advantageous than manual drawings, because the standardization among the figure sizes can be ensured and the image resolution is high.
Because there were fewer radiographs belonging to the age groups including earlier periods of dentition, diagrams belonging to these periods could not be prepared. For the same reason, there were fewer samples from the age group 4.5-5.5 years than for the other groups.
Several methods have been described for the assessment of dental development from radiographs.18,25,26,27 Among them, Demirjian et al has shown the mineralization of teeth in 8 stages, whereas Nolla et al used 10 stages and Moorrees et al 14 stages, with comprehensive drawings. One of the most efficient and popular age and maturity estimation method has been Demirjian's.18 Selection of tooth stage assessment is a significant factor that affects reproducibility.10,28 Consequently, to show the stages of tooth mineralization, the Demirjian classification system has been preferred because it is well known internationally for evaluating the dental maturity of children and is highly reproducible.
Even though dental age estimation with the atlas style has some limitations compared with that by other techniques, these charts have been recommended for use as a screening tool for age assessment, particularly in mass disasters.
Some researchers have suggested that using fewer stages increased intra- and interobserver repeatability.10,29,30 This approach was unquestionably true, but with increased repeatability came decreased precision. Repeatability alone was inadequate. If there were numerous stages, each defining a narrow, specific developmental interval, age estimations would be more accurate.31 This was why it was believed that the use of the preferred classification system for age estimation, with increasing stage numbers that did not create repeatability problems, would be appropriate.28 Thus, Demirjian's classification system was modified for this study. Thorson and Hägg32 reported the presence of a stage called "late G" when investigating the accuracy and precision of the third molar development in a Swedish adolescent population. Similarly, Solari and Abramowich33 divided Demirjian's F and G stages into two additional stages. We described the H1 stage between stages G and H in Demirjian's classification system because the need arose during the assessment of the developmental stages of the teeth. The stage described was compatible with the 13th stage of Moorrees' classification system.26 The stage in which tooth maturation was completed, with the closing of the apex, was referred to as the H2 stage. Thereby, Demirjian's classification system with eight stages was modified to have nine stages. The additional stage might improve the accuracy in dental age estimation. In particular, we observed that to differentiate correctly between the two stages (H1 and H2), a magnifying glass was required for the evaluation of conventional panoramic radiographs and for appropriate magnification adjustments for DPRs.
During our evaluations, the classification stages of the Demirjian method were used only for determining mineralization stages because the aim of this study was not to estimate the dental age of DPRs but to illustrate charts to facilitate the determination of tooth mineralization and eruption stages for specific age groups. This was the reason that we used seven teeth not only from the left side of the jaw, as in Demirjian's age estimation technique, but also from the left mandible and both the third molars.
In many studies, it has been reported that dentition shows gender differentiation, with that in girls preceding that in boys.18,25,34,35 In this study, it was found that tooth maturation occurred earlier in girls except for the third molars. Third molar mineralization was similar in both genders except for a one-stage difference in one of the jaws in three age groups. This finding was congruent with those in the studies in which the third molar mineralization had been studied in different populations.31,36,37 In two different studies conducted in two remote areas of Turkey in which the third molar mineralization was evaluated according to Demirjian's classification system, gender differentiation was reported in one of them at only one stage,38 and in two stages in the other.39 When the data between the studies were compared for gender differentiation, they were found to be similar.
A good comparison could not be made among tooth development stages with earlier atlases, which were based on tooth formation because most atlases were not developed according to gender differences, and the ranges of age groups were defined differently. However, when a general comparison was made, it was found that the maturation of the teeth except that of the third molars occurred at approximately 15 years of age; this finding was similar to the results obtained with earlier atlases.13,14,16 In the age groups in which the third molar development was assessed, the significant deviation of the minimum and the maximum values from the median showed that variations in the formation of this tooth were more than those in the formation of the other teeth, as reported previously.40,41
As a parameter of developmental morphology, tooth eruption is different from tooth mineralization as it can be determined by both clinical examination and assessment of dental radiographs.42,43 For dental age estimation, the use of gingival eruption is not suitable in either archeological specimens or dental radiographs of the living.12,44 For this reason, during the development of the new charts, the assessments were made according to alveolar bone eruption. As shown in the atlas of AlQahtani et al,16 in this study, it was also observed that the mixed dentition period ends when deciduous teeth were shed in children at the age of approximately 12 years. Despite this, in the atlases of Schour and Massler13 and Ubelaker,14 the mixed dentition period ended about 1 year earlier than in our study. It was thought that this difference could arise from the differences in genetic and environmental factors of the societies whose tooth formation and eruption data were taken as a reference when the atlases were being formed.
The dental charts presented here included information that could be beneficial for dental clinicians in making appropriate diagnosis and planning orthodontic and surgical procedures. Moreover, these charts provided datasets of preliminary dental age estimation for Turkish children and young adults. Dental development and eruption data of children in the age group of 4.5-22.5 years were peculiar to the Turkish population. For these data to be used for clinical or forensic applications in different populations, a validation study should be conducted on sufficient samples of the respective populations.







 XML Download
XML Download