

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Odontogenic keratocyst is a distinctive form of developmental odontogenic cyst because of its specific histopathologic features, an aggressive biologic behavior and a high recurrence rate.1 It has been recently proposed to be named "keratocystic odontogenic tumor" (KCOT) rather than a cyst by the World Health Organization and defined as a benign uni-or multicystic intraosseous neoplasm of odontogenic origin with a characteristic lining of parakeratinized stratified squamous epithelium.1-3 The most common location of KCOT is posterior body of mandible and ramus.4-6 KCOT demonstrates a well-defined radiolucent area with smooth and often corticated margins while large lesion may appear multilocular.1 Most of KCOTs (83.5%) have been found to be unilocular, and only 16.% multilocular.1
KCOT can occur alone or as part of the nevoid basal cell carcinoma syndrome (Gorlin syndrome). Gorlin syndrome is an autosomal-dominant disorder that has various clinical manifestations such as multiple basal cell carcinomas of the skin, multiple KCOTs of the jaws, skeletal abnormalities, eye abnormalities, and central nervous system abnormalities.4 The KCOTs associated with nevoid basal cell carcinoma syndrome displayed different characteristics from non-syndromic cases.3
Treatment of KCOTs remains controversial. The challenges lie in minimizing both the risk of recurrence and the surgical morbidity.5,7 Simple enucleation with or without curettage and marsupilization are conservative treatments of KCOT. Aggressive treatment includes peripheral ostectomy, chemical curettage using Carnay's solution and resection.6 Long-term follow up is mandatory for successful treatment.5
KCOT has a propensity to grow in an antero-posterior direction within medullary cavity of bone, therefore it may be very large before detection since swelling may not be dominant. This feature may be useful in differential clinical and radiographic diagnosis because dentigerous and radicular cysts of comparable size are usually associated with bony expansion.1,4 Definitive diagnosis relies on histological examination. In this report, a KCOT that had caused an expansion of both buccal and lingual cortical bone is described with its features in computed tomography and ultrasonographic exams.
Case Report
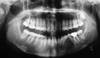
A 30-year old woman presented with a painless swelling in the left mandibular posterior area. The patient had noticed this swelling for approximately 8 months. The patient's medical and familial history was noncontributory. Clinical intraoral examination showed the buccal and lingual bony expansion around the left mandibular canine and first and second premolars (Fig. 1). The teeth involved in the lesion were vital with electrical vitality test except the first premolar. Panoramic radiograph revealed a well-defined unilocular radiolucency extending from the distal aspect of the mandibular left lateral incisor to the distal area of the left second premolar (Fig. 2). The lesion displaced the roots of the mandibular left canine and the first and second premolars.
Axial computed tomographic (CT) images showed an ovoid well-defined scalloped cystic lesion 28×18 mm in diameter without bone septa and calcifications. The lesion caused expansion and destruction buccally and lingually. There was a soft tissue extension without invasion through the cortical perforation. There was no contrast enhancement in the center of the lesion but marked in periphery. Coronal CT images showed an expansive process with scalloped border in mandibular corpus (Fig. 3).
Ultrasonography (US) examination showed a 26.5×20 mm sized, oval, ill-defined dens cystic content with no evidence of internal vascularization. It had a posterior enhancement (Fig. 4).
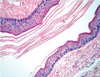
The lesion was surgically removed via an intraoral approach under local anesthesia and histologically reported as a KCOT (Fig. 5). The patient was currently at the fifth month of follow-up without a recurrence.
Discussion
An important characteristic of KCOT is its propensity to grow along the internal aspect of the jaws, causing minimal expansion.1,4 Because a considerable number of KCOTs are asymptomatic and their clinical signs often fail to appear, these lesions are mostly detected in the late stage, which occasionally allow them to reach a large size.4,7,8 Sometimes they are detected only by incidental radiographic findings.7,9 It was reported that swelling and pain were more frequent in East Asians, whereas KCOT discovered as an incidental finding was more frequent in the Latin American reports.3 Boffano et al5 analyzed 261 KCOTs and reported that 37.2% of patients presented with symptoms and 62.8% were asymptomatic with their lesions found incidentally. In the present case, the KCOT caused an unusual clinical sign of buccal and lingual cortical expansion despite its small size.
The radiographic appearance of KCOT may resemble that of many other odontogenic lesions. If it is associated with a crown of an unerupted tooth, it may be indistinguishable radiographically from dentigerous cyst.1,8 The scalloped margin and multilocular appearance of KCOT may resemble an ameloblastoma but the greater propensity to expand of ameloblastoma may help for differentiation of these lesions. KCOT may show similarity to an odontogenic myxoma because of the mild expansion and multilocular appearance.4
Complete radiographic examination is essential in suspicion of KCOT because of its aggressive behavior and high recurrence rate. CT can be used to determine the extent and location of any cortical perforations with soft tissue extension.4 In the present case, axial CT images demonstrated a significant expansion and perforation of the buccal and lingual cortical plates of the mandible. Generally a significant expansion may occur in the upper ramus and coronoid process, however the buccal and lingual cortical plates of the mandible revealed slight expansion only.
US is noninvasive and cost-effective, and recommended as a complementary imaging method for intraosseous lesions of the jaw.10,11 However, it is not useful in the presence of intact and thick cortical bone and usually the growth of KCOT is larger in mesial-distal direction than in the buccal-lingual, maintaining the vestibular and lingual/palatinal bones intact.10 Therefore, US examination could be inconclusive in some KCOT lesions.10,11 In the present case, US examination was effectively used in the assessment of the lesion due to the significant buccal and lingual cortical expansion. US examination showed dense cystic content with no evidence of internal vascularization. This finding was consistent with findings by Lauria et al10 and Sumer et al.11
In conclusion, a keratocystic odontogenic tumor that revealed an unusual expansion of buccal and lingual cortical plates of the mandible was described with its features on CT and US exams.


 XML Download
XML Download