

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dental implantation treatment can be applied with high success rates in cases with adequate alveolar bone height and width [1]. Under conditions where residual bone is not available for standard implantation, before the implantation treatment, advanced surgical techniques such as sinus floor elevation, inferior alveolar repositioning, or vertical bone augmentation are commonly required [2]. However, despite the many reports of successful use of advanced surgical techniques, in addition to complication risk, the increase on the morbidity of the patient, treatment period, and total treatment cost should not be ignored [3,4]. In fact, in the presence of a thin ridge and narrow gaps between two natural teeth, mini implants are recommended as an alternative to bone grafting in order to avoid exposing the patient to multiple surgical procedures. Additionally, usage of short, wide implants is recommended when the alveolar crest height is low. The factors affecting the bone-implant interface are determined to be the geometry, diameter, and surface area of an implant located on bone [5]. From the bioengineering perspective, designing an implant that has a geometry that lowers the maximum bone stress induced under standard loading is crucial [6]. Thus, usage of short and mini implants with single crowns have become widespread in such cases [7].
Bhardwaj and Prabhuji [8] measured the proportions of peri-implant crevicular fluid (PICF) and gingival crevicular fluid (GCF) present in order to evaluate their relationship using various clinical indexes to determine their behavior in response to gingival and peri-implant inflammation. They found that PICF and GCF volumes demonstrated a similar nature through increasing grades of inflammation, with PICF showing a stronger correlation with the clinical parameters. As it is difficult to determine a diagnosis of peri-implant disease only on a clinical basis, PICF analysis to measure the disease activity is a reasonable objective basis for diagnosis [9].
Osteoclastogenesis is an extremely gradual process that includes migration, proliferation, differentiation, fusion, and activation of the progenitor cells. This process is coordinated with the interactions of RANK ligand (RANKL), RANK, and osteoprotegerin (OPG) [10]. In a recent study performed on healthy and inflamed periodontal tissues, concentrations and distributions of OPG and RANKL were analyzed and an enhanced ratio of RANKL/OPG was detected in the inflamed tissues. The researchers reported that this ratio change could have been based on either a decrease in RANKL, an increase in OPG, or both [11]. A recent study noted the presence of a correlation between the rise in OPG and the severity of disease [12].
Cathepsin -K (CTSK), which plays an important role in bone remodeling and destruction, is secreted from osteoclasts [13]. CTSK, which effectively catabolizes the bone matrix proteins including collagen type-1 and osteonectin, is an important member of the lysosomal proteins [14]. These characteristics indicate that CTSK plays an important role in osteoclastic activity. Yamalık et al. [15] suggested that CTSK is a biochemical parameter for monitoring periodontal/peri-implant alveolar bone loss.
In light of all this, the aim of our study is to compare dental implants with varying geometry and the same surface properties during the early period after prosthetic loading. The goal of measuring the clinical parameters and PICF levels of CTSK, RANKL, and OPG in this investigation is to predict the best treatment option among the implants for successful long-term outcomes.
MATERIALS AND METHODS
Patients' selection
Thirty patients (13 men and 17 women) with a median age of 50 years (range 26-62) who were partially edentulous were selected for this prospective study from the clinic of the Periodontology Department, Faculty of Dentistry, Selcuk University, Turkey. Informed written consent, approved by the Ethics Committee of the University of Selcuk (Approval number: 2013/7), was obtained from the patients to use their data for research purposes.
The following inclusion criteria were applied: a) age >18 years, b) partial edentulism, c) good oral hygiene, d) absence of any local or systemic diseases that might contraindicate the treatment. The patients were excluded on the basis of the following: a) uncontrolled diabetes mellitus or other systemic disorders, b) uncontrolled periodontal conditions or other oral disorders, c) previous bone grafting at the surgical site, d) not pregnant or lactating. Based on a literature review, it was determined that cigarette smoking may represent an additional risk factor for implant therapy; nonetheless, smoking should not be an absolute contraindication [16]. Thus, smoking patients were not excluded but were informed that smoking is associated with an increased implant failure rate.
In addition, the patients agreed to participate in a postoperative control program. At least one and a maximum of seven implants were used, including a total of 78 implants placed in 30 patients. Implants with the same surface features (a sand-blasted and etched surface) were used (Euroteknika, Aesthetica+2, Sallanches, France). Participants were enrolled into the following groups. Patients in the Standard Group (n=27) were provided standard dental implant placement, Short Group (n=26) patients received short dental implant treatment, and Mini Group (n=25) patients received mini dental implant treatment. The diameters and the lengths of implants used in this study are detailed in Figure 1.
Figure 1
Euroteknika Aesthetica dental implants installed in this study: A: Standard dental implant (lengths ranging from 8 mm to 14 mm and diameters from 3.6 mm to 4.8 mm), B: Short dental implant (length 6 mm and diameters ranging from 4.1 mm to 4.8 mm), C: Mini dental implant (lengths ranging from 9 mm to 15 mm and diameter 2.7 mm).

Pre-surgical preparation
All patients received examinations, appropriate treatment, and oral hygiene instruction regarding periodontal diseases and caries before the implant installation. Panoramic radiographs were obtained before implant installation.
Surgical procedure
For each patient, a pre-operative panoramic radiograph was performed to mark implant placement sites, detect magnification errors, and select proper implant lengths. Local anesthesia was administered using Ultracain® (Sanofi, Istanbul, Turkey). A crestal incision was followed by elevation of the mucoperiosteal flaps buccally and lingually. Preparation of implant sites was performed by rinsing them with sterile saline. The implants were inserted according to the recommended procedures. During the one-stage surgery, after inserting the implant, healing abutments was installed and the flaps were adjusted to the implant and sutured. No complications occurred during surgery or the post-surgical healing period in any of the patients, and all the inserted implants had acceptable primary stability. Postsurgical panoramic radiographs were performed to evaluate implant placement and showed that the implant shoulders were at the crestal bone level (Figure 2). Additionally, no guided bone regeneration procedure was performed in any of the cases.

Post-surgical procedure
Patients were prescribed the following medications after surgery: antibiotics (amoxicillin 1g twice a day for 7 days or clindamycin 150 mg four times a day for 7 days for patients allergic to penicillin), analgesics (flurbiprofen 100 mg twice a day as needed) and oral antiseptics (rinses of 0.12% chlorhexidine gluconate for 1 minute twice a day for 15 days). Patients were also instructed not to wear any type of prosthesis that could come in contact with the surgical area following the surgical procedure. Patients were seen at 1 and 2 weeks after the one-stage procedure to monitor healing and postoperative complications. Sutures were removed after 7-10 days.
Restorative procedure
After 4-6 months of healing, the patients were recalled for the restorative treatment. A panoramic radiograph was taken to examine whether radiolucency existed around the implant body. Metal-ceramic crown prostheses were fabricated and cemented within about 1-2 weeks.
Clinical and radiographic evaluations
After the osseointegration period was completed, PICF sampling and clinical measurements were done prior to installation and prosthetic loading was applied in the same day. Sampling and measurements, followed by the installation, were repeated on post-loading days 2, 14 and 90. Panoramic radiographs were taken after surgical procedures and at 90 days.
The plaque index modified by Mombelli et al. (mPI) [17] and gingival index modified by Loe and Silness (mGI) [18] were used. The mPI and mGI were recorded around each implant at four locations: mesiobuccally, distobuccally, mesiolingually, and distolingually. The average of the mPI and mGI scores at the four locations for each implant were calculated.
Using a calibrated pressure-sensitive plastic periodontal probe (the Colorvue™, Hu-Friedy, US), the distance between the marginal border of the gingiva and the tip of the probe was measured and considered to be the probing pocket depth (PPD). The PPD was recorded for six locations around each implant: mesiobuccally, bucally, distobuccally, mesiolingually, lingually and distolingually [19]. The average of the six PPD scores collected for each implant was calculated. The bleeding tendency of the peri-implant mucosa, as a measure of soft-tissue inflammation, was evaluated using the modified sulcular bleeding index (mSBI) [17], measured at four sites around the implant (mesially, distally, and at the buccal and lingual mid-point).
The width of peri-implant keratinized mucosa (KT) was measured in millimeters on the facial aspect (mesially, at the mid-point and distally). Differences in color, texture, and mobility between the keratinized mucosa and the lining mucosa served as markers for the detection of the muco-gingival junction. KT was then measured as the distance between the gingival margin and the muco-gingival junction, and measurements were rounded to the nearest millimeter [20]. The average of the values collected for a given implant was then determined.
Radiographs were taken at each of the clinical procedure appointments at implant placement and 90 days after prosthetic loading. Measurements on panoramic radiographs obtained were carried out by measuring the image files after transfer to the image processing program (ImageJ 1.46r, NIH, Maryland, USA), and the actual amount of bone loss (MBLR) was determined. Vertical measurements of the bone level adjacent to the implants were made from the top of the implant, which provides a fixed reference point. Calibration of the measured increments of bone change is necessary in determining actual bone loss from radiographic measurements, particularly on panoramic radiographs, which generally provide an enlarged image of teeth and implants. Formulas from Manz [21] were used for calibration. These calibrated (i.e. actual) measurements from baseline and follow-up appointments were compared for a given implant to determine vertical bone height changes.
PICF sampling
Patients were all scheduled for sample collection at approximately the same time of the day to prevent any cyclical variations from affecting the crevicular fluid volume. To avoid salivary contamination, the selected sites were isolated by cotton rolls and dried with a gentle air spray. A saliva ejector was being concurrently applied during the sampling protocol. The supragingival plaque was removed gently with dry gauze, and a standardized paper strip (Periopaper®, ProFlow, Inc., Amityville, NY, USA) was inserted 1-2 mm into the sulcus. The strip was held in place for 30 seconds and transferred to a precalibrated electronic fluid quantification device (Periotron 8000, Harco Electronics, Winnipeg, Canada). Samples were transferred to Eppendorf tubes that had been stored at -20°C after sampling and the tubes were then stored at -80°C until the day of analysis.
Analysis of PICF samples
RANKL, OPG, and CTSK levels of PICF were analyzed. Analysis was performed using ELISA with commercially available kits (sRANKL: BioVendor, Czech Republic / OPG: RayBio®, US / CTSK: Uscn, PRC) according to the manufacturers' recommended procedures. The minimal detection limits were: sRANKL (0.4 pmol/L), OPG (1 pg/mL) and CTSK (0.065 ng/mL).
Statistical analysis
All data were first analyzed descriptively and were presented as mean±SD values. We used the Wilcoxon signed rank test to compare the baseline data with the data from day 2, 14 and 90 post-loading for each group and the Friedman test to compare parameters among the three implant groups at baseline and at each post-loading follow-up day. The significance level was set at p<0.05. Statistical analysis was performed with SPSS Statistics for Windows version 15.0 (SPSS, Inc., Chicago, IL, USA).
RESULTS
Patient information and clinical findings
In our study, in 30 volunteer patients with a median age of 50, including 17 women and 13 men, 78 single-stage implants were completed. At the beginning of the study, the patients underwent tooth surface cleaning and oral hygiene education. In the follow-up period, if necessary, tooth surface cleaning and oral hygiene instruction were repeated with the patients. The implants used in the study were examined in three groups receiving standard, short, or mini implants (Table 1).
Clinical, radiographic, and biochemical parameters
Changes in clinical and biochemical parameters were inspected relative to baseline (pre-loading day) after the completion of implant osseointegration when loading would be performed and the measurements were repeated on post-loading days 2, 14, and 90. Radiographic evaluation was performed at baseline and day 90. The intragroup distributions of clinical parameters at the follow-up points in time are shown in Figure 3.
Figure 3
Intragroup distribution of clinical parameters at follow-up time intervals. A: distribution of probing pocket depth (PPD); B: distribution of modified plaque index (mPI); C: distribution of modified gingival index (mGI); D: distribution of modified bleeding index (mSBI). The plots indicate the mean±standard deviation of the samples (a)
P<0.05, b)
P<0.01, c)
P<0.001: statistically significant difference at the respective points in time). B, baseline; d, day.

The PPD value was found to have increased in a statistically significant manner at the follow-up time intervals when compared with baseline (Figure 3A). The mPI values of the standard and short implant groups showed statistically significant increases at post-loading days 14 and 90 when compared with baseline. While a statistically significant decrease was obtained for the mPI value of the mini implant group at post-loading day 2, an increase was detected on day 90 when compared with baseline (Figure 3B). Compared with the baseline, a statistically significant reduction in the mGI value was only detected on post-loading day 2 in the short implant group, with a statistically significant increase in the standard and short implant groups on day 90 except in the mini implant group, which showed no significant change (Figure 3C). When compared with baseline, the mSBI values of the standard and short implant groups displayed a significant increase at post-loading days 14 and 90. Although a statistically significant decrease was detected at day 2 in the mini implant group, the increase found on day 90 in that group was non-significant (Figure 3D).
Furthermore, the intergroup distribution of clinical parameters at follow-up time intervals was also evaluated. Only PPD values revealed intergroup differences at all sampling periods. Thus, no statistically significant differences in terms of PPD values were detected between the standard and short implant groups throughout the study, but the PPD values were statistically significantly higher than in the mini implant group. Unlikely only short implant group was displayed a statistically significant increase on day 2 in comparison with mini implant group.
The distribution of PICF volumes at all sampling periods are displayed in Figure 4. The pre-loading PICF volumes did not differ between the standard and short implant groups, but were significantly higher than the mini implant group. At the end of the study (post-loading day 90), a statistically significant increase was detected in all of the implant groups relative to pre-loading. Additionally, while the increase in the mini implant group at post-loading day 14 relative to baseline was found to be statistically significant, by day 2, the change was not yet statistically significant in any of the groups. Although no statistically significant differences in the PICF volume between the short implant group and other groups were found at the end of the study, the PICF volume in the standard implant group was significantly higher than that of the mini implant group.
Figure 4
Intragroup distribution of peri-implant crevicular fluid (PICF) volumes at follow-up time intervals. The graph indicates the mean±standard deviation of the samples (a)
P<0.05, b)
P<0.01: statistically significant difference). B, baseline; d, day.

According to the distribution of biochemical parameters at follow-up time intervals (Figure 5), no significant differences in any of the groups were detected with regard to the total amounts of sRANKL and CTSK at day 90 compared with baseline (Figures 5B and C). A statistically significant reduction in the total amount of OPG was detected only in the short implant group at the end of study (Figure 5A). Considering the distribution of the OPG: sRANKL ratio, no significant inter- or intra-group differences from baseline were found at the end of the study (day 90) (Figure 5D).
Figure 5
Intragroup distribution of biochemical parameters at follow-up time intervals. A: distribution of total amount of osteoprotegerin (OPG); B: distribution of total amount of soluble RANK ligand (sRANKL); C: distribution of total amount of cathepsin -K (CTSK); D: distribution of OPG: sRANKL ratio. The plots indicate the mean±standard deviation of the samples (a)
P<0.05, b)
P<0.01, c)
P<0.001: statistically significant difference at respective points in time). B, baseline; d, day.

Although no differences were observed between the intergroup KT values of the standard and mini implants at baseline or on post-loading day 90, the KT values of the short implant group were determined to be significantly lower than those of the other groups. Despite the reduction in KT values by the end of the study, no statistically significant intragroup differences were found relative to baseline. Additionally, when the extent of change in KT was compared among groups, no statistically significant differences were observed.
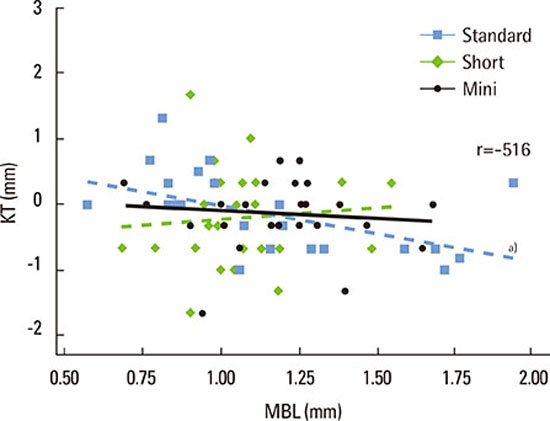
The analysis of the MBL values of the implant groups and implant sites (maxilla/mandible) showed intragroup differences in both the MBL mean and the MBL in each implant site. The average MBL value of the maxilla was higher than that of the mandible. However, the difference observed was only statistically significant in the standard implant group when the MBL values of the maxilla and mandible were compared. A lower MBL was observed at standard mandibular implants than in standard implants in the maxilla. Although the MBL was higher in the maxilla than the mandible, no statistically significant differences were found in the MBL values among the implant sites, in the short and mini implant groups. Moreover, no statistically significant differences were observed in intergroup comparisons of MBL values in the maxilla or in the mandible. When the correlations between intragroup KT changes and MBL values were considered, only their relationship in the short implant group was found to be statistically significant and negative. Thus, as the MBL value in the short implant group increased, the KT value decreased. No significant relationship between KT changes and MBL values was detected in the standard and mini implant groups (Figure 6).
Figure 6
The correlation between intragroup keratinized tissue (KT) alteration and marginal bone loss (MBL) values are presented. a)The relationship only in the short implant group were observed to be statistically significant and negative. No significant relationship was detected in the other groups. r, Pearson's correlation coefficient.

DISCUSSION
The results of this study have shown that changes in PICF levels of sRANKL, and CTSK were not statistically significant in any of the groups, while the OPG level significantly decreased in only the short implant group. Furthermore, CTSK levels demonstrated a positive correlation with sRANKL levels only in the mini implant group, and furthermore, both of them decreased. The sRANKL, OPG, and CTSK levels were not correlated with any of the clinical parameters in any of the groups, except the sRANKL level with mSBI and mPI in the short and mini implant groups, respectively, and the CTSK level with PPD in the mini implant group.
In a previous study, positive relationships were reported between biomarkers of peri-implantitis and clinical parameters evidencing peri-implant destruction [22]. Monov et al. [23] reported no significant correlation between sRANKL and OPG levels and clinical parameters, while Arikan et al. [24], investigating the same biomarkers, reported a significant correlation between OPG and mSBI. The present study also showed no significant correlation between the total amounts of sRANKL and OPG and the clinical parameters in the standard implant groups; likewise, no significant correlations were detected in the short and mini implant groups, excluding significant relationships between sRANKL and mSBI and between sRANKL and mPI, respectively. These differences could possibly be explained by the differences in the detection methodology and detectability rates used in the reported studies [25].
Moreover, in other studies, the relative ratio of OPG: sRANKL was described as a more accurate diagnostic method for evaluation of periodontal disease activity [12]. In periodontitis, the reduction of OPG/RANKL was reported when compared to sites with gingivitis and healthy sites [26]. Despite varying MBL among the groups, in the present study, no significant differences were found in the OPG: sRANKL ratio, as in previous studies. Besides, the observed OPG: sRANKL ratio showed no statistical intra- or inter-group differences relative to the baseline.
Yamalık et al. [15] investigated CTSK activity in peri-implantitis and reported increased activity in peri-implantitis compared to mucositis, while in a more recent study, CTSK activity was higher in both peri-implantitis and mucositis tissue when compared to healthy peri-implant tissues, thus suggesting CTSK to be an accurate biomarker of the loss of implant-supporting bone [27]. Strbac et al. [28] investigated CTSK levels in peri-implantitis and reported that the levels were significantly higher in peri-implantitis cases and were positively correlated to PPD, mSBI, and PI. In addition to a study indicating that the CTSK concentration correlates only with PI [22], another study found a positive correlation of CTSK enzyme activity with PPD and GI [27]. In the present study, while the total amount of CTSK showed no correlation with clinical parameters in the short or standard groups, the total amount of CTSK displayed a positive correlation only with PPD in the mini implant group.
Furthermore, in a study performed by Mogi and Otogoto [14], a positive correlation between CTSK and RANKL levels was detected, suggesting that excess production of RANKL resulted in the formation of active osteoclasts and led to CTSK production in osteoclasts in the periodontium, thus contributing to osteoclastic bone resorption at the relevant site. Another study showed that CTSK activity is correlated with PICF volume [27]. In the present study, no statistical difference was observed in the total amounts of CTSK on follow-up when compared to baseline. Additionally, a positive and significant correlation was detected only in the mini implant group considering the CTSK and sRANKL levels; a reduction in both levels was found at the end of the study when compared to pre-loading. No correlation was shown between the total amounts of CTSK in any of the groups and the PICF volume.
The long-term survival of dental implants was proven in both the maxilla and mandible [29]. Clinical reports indicate that mandibular implants possessed higher survival rates than implants in the maxilla (especially the posterior maxilla) [30,31]. On the other hand, according to the study performed by Koldsland et al. [32], no statistically significant difference was observed between the maxilla and mandible with regard to the loss of implants. According to the results of the present study, when the MBL values of the maxilla and mandible were compared within groups, while no differences were observed in the short and mini implant groups, the MBL values of the standard implants placed in the maxilla were significantly higher than the mandible. Besides, individual intergroup comparison of the MBL values of the maxilla and mandible showed no statistically significant differences. Furthermore, it has been agreed that when less than 2 mm of radiographically marginal bone loss around the implants occur, the prognosis of implants is very good to excellent [29].
There is no consensus in the literature regarding the influence of the presence or absence of KT on the long-term health of implants [33]. Some studies have presented an association between lack of KT and increased soft-tissue recession, increased bleeding on probing, slight bone loss, greater accumulation of plaque and greater gingival inflammation [20,34,35]. However, another study showed no relationship between implant survival and KT width [36]. In the present study, however, the intragroup reductions were observed with regard to pre-loading KT values, but none of the differences were statistically significant. In the relationship with intragroup MBL values, KT displayed a statistically significant and negative correlation only in the short implant group.
The clinical parameters used in the diagnosis of periodontal diseases (including bleeding on probing, probing pocket depths, and relative clinical attachment levels) were considered not sensitive enough to provide correct diagnostic information on the risk ratio, disease onset and activity, prognosis, and treatment outcomes when applied to the diagnosis of peri-implant diseases [22]. This is probably due to the different biology of the peri-implant tissues compared with periodontal tissues [37] and to other factors related to the implant and its prosthetic design, which can clearly affect the accuracy of probing [38].
Yamalık et al. [15] indicated that it is not possible to precisely determine the bone loss during the destructive peri-implantitis process. They specified the importance of CTSK analysis for diagnosis due to the alterations related to alveolar bone loss occurs in an early period in the GCF/PICF enzymatic profile. In addition to CTSK levels, increased levels of RANKL, and OPG: RANKL ratio are considered indicators of periodontal inflammation and of periodontal disease activity and severity [22].
Consequently, biochemical parameters of bone resorption may reflect the active stage of tissue destruction and the silent phase of the disease. Thus, prospective longitudinal studies are needed to correlate disease progression with biochemical parameters of bone resorption within the PICF. These studies could help to identify an early diagnostic marker of peri-implantitis that will work before clinical parameters are measurable. The obtained data could contribute to detecting the transition from peri-implant mucositis to peri-implantitis and also yield information about the pathophysiological mechanisms underlying the different stages of peri-implantitis [28]. Additionally, although the number of follow-ups and their time intervals may have been too short to draw firm conclusions from the present study, our findings may be useful in the clinic to inform the early detection and prevention of implant failure or implant-related diseases and also to predict the best treatment option for long-term success.
In the present study, the bone loss around the dental implants with varying geometry was considered to be acceptable for a good prognosis of implants in the early period post-loading due to in the lack of substantial alterations of the OPG: sRANKL ratio and CTSK levels at the end of the study compared to baseline. Results similar to those from standard implants were obtained with both short and mini dental implants in the post-loading period within the limitations of this study. Additionally, longer-term follow-up studies are needed.
 XML Download
XML Download