

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Stroke is a common and leading cause of various disabilities. Approximately 100,000 people per year in the UK have a first stroke [1] and an additional 30,000 people have recurrent strokes [2]. It has been estimated that between 1983 and 2023, the number of new stroke patients per year will increase by 30% [3]. Majority of stroke survived patients exhibit persisting motor disorders and various manifestations of the upper motor neuron syndrome (UMN) [4]. Stroke-related complication such as spasticity is classified as a sign of UMN syndrome which is a clinical phenomenon observed after lesions of cortical motor areas or corticofugal descending tracts [5]. UMN syndrome includes both positive and negative features; positive features include spasticity and abnormal postures, and negative features include loss of strength and dexterity [6].
Spasticity is commonly defined as a motor disorder characterized by velocity dependent hyperexcitability of muscles to stretch, exaggerated tendon jerks, increased resistance to passive movement and hypertonia resulting from loss of upper motor neuron inhibitory control [7].
The scale used for quantifying and clinically evaluating spasticity is the Modified Ashworth Scale (MAS), which has documented reliability [8]. MAS does not reflect other spasticity related phenomena such as co-contraction during voluntary movements or spasms, and other dystonic posturing of limbs [9]. Despite these limitations, clinicians have commonly used MAS because it is simple and reliable.
In previous studies, the prevalence of post-stroke spasticity was 33%–60% [101112] and spasticity could be triggered by noxious and external stimuli (e.g. pain, incontinence, constipation, infections, inflammation and pressure sores) [13]. Despite the high prevalence, there is no current consensus on post-stroke spasticity, especially in regard to distribution, severity, risk factors and related functional status.
This Korean stroke cohort study was carried out to investigate the prevalence of spasticity at 3 months after first-ever stroke, and to identify distribution, severity and risk factors of spasticity.
MATERIALS AND METHODS
Study design
Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO) is a large, multicenter prospective cohort study with nine participating hospitals from nine distinct areas in Korea. KOSCO aims to comprehensively assess survival rates, recurrence rates, function, mood, and quality of life of patients with ischemic or hemorrhagic stroke. The KOSCO study obtained written informed consent from all patients prior, and the study protocol was approved by the ethics committees of each hospital. The detailed rationale and protocol of KOSCO has been described in the previous article [14]. As the study was based on tertiary-hospital and almost acute stroke patient had treatment in tertiary-hospital, generalization to the Korean patients of KOSCO study could be possible.
KOSCO aims to estimate the prevalence rate of spasticity according to MAS at 3 months after first-ever stroke and determine the risk factors for the same by cross sectional study (Fig. 1).

Study population
For this study, 6,675 patients with acute first-ever stroke from representative hospitals in 9 distinct areas of Korea were enrolled from August 2012 to May 2015 (Fig. 1).
The eligibility criteria is as follows: 1) First-ever acute stroke (ischemic stroke or hemorrhagic stroke) with corresponding lesion and/or evidence of acute arterial occlusion on CT or MRI/A-scan; 2) Age ≥ 19 years at onset of stroke; 3) Onset of symptoms within 7 days prior to inclusion. Patients with following criteria were excluded from this study: 1) Transient ischemic attack; 2) History of stroke; 3) Traumatic intracerebral hemorrhage; 4) Foreign patients.
Spasticity assessment
Spasticity was assessed with MAS, which is a 6-point ordinal scale with documented reliability. Spasticity was defined as MAS score ≥ 1 for any of the passive movements around each joint. All patients were assessed upper limb (elbow flexor) and lower limb (ankle plantar flexor) respectively. The reason for assessment of elbow flexor and ankle plantar flexor is that spasticity primarily affects the elbow and ankle [15]. To minimize the impact of posture and prior exercise on muscle tone, all patients were assessed in a supine position. The test was done a maximum of three times for each joint. To assess elbow flexor spasticity, elbow was fully flexed and forearm was neutral position. And then elbow was fully extended from maximum possible flexion to maximum possible extension. To assess ankle plantar flexor spasticity, ankle was plantar flexed and hip was in neutral rotation and flexion and with knee flexed to nearly 15 degrees [16]. Assessment was performed 3 months after a stroke occurrence by occupational therapists who are skilled in physical examination measuring MAS.
Risk factors for spasticity
The following survey parameters were collected for medical records during the first admission. Survey items consisted of demographics (age, sex, dominant hand, education), physical examination (height, weight, body mass index [BMI]), stroke characteristics (stroke type, stroke side, stroke severity, disability), medical history (hypertension, diabetes, coronary heart disease, atrial fibrillation, left ventricular hypertrophy, peripheral artery disease, hyperlipidemia, low cholesterol, unruptured intracranial aneurysm, arteriovenous malformation, obesity, family history, smoking, alcohol consumption). Presence of cerebrovascular risk factors were assessed by standardized and structured questionnaires, and answers were classified according to the current guidelines of the American Heart Association [17].
Assessment of neurological deficits and functional ability
We performed face-to-face functional assessment using the National Institute of Health Stroke Scale (NIHSS) [18] for stroke severity and modified Rankin Scale (mRS) [19] for general functional level.
Detailed functional outcome measures were as follows:
1. The NIHSS is used to measure stroke severity. The NIHSS is a 42-point ordinal scale, ranging from 0 to 42 with higher scores that measures neurologic deficit, and is frequently used in stroke studies [20]. The scale assesses level of consciousness, extraocular movement, visual fields, facial muscle function, extremity strength, sensory function, coordination (ataxia), language (aphasia), speech (dysarthia), and hemi-inattention (neglect).
2. The mRS is used to measure the degree of disability after stroke. The mRS attempts to measure functional independence, incorporating the World Health Organization (WHO) components of body function, activity, and participation [18]. The scale is ranged from 0 to 6, running from perfect health without symptoms to death.
Ethics
Written informed consent is obtained from all patients or patient’s legally authorized representative prior to inclusion in the study, and the study protocol is approved by the ethics committees of Pusan National University Yangsan Hospital and each ethics committee of the other participating hospitals.
Statistical analysis
Descriptive statistics were used for baseline characteristics and for some of the follow-up data at 3 months after stroke occurrence. The parameters of age, NIHSS scores and occurrence of spasticity were tested by using descriptive statistics and frequency analysis. Chi-square test compared the clinical characteristics of patients with no spasticity versus patients with spasticity at 3 months after first-ever stroke. A χ2 test was performed to explore the risk factors that were identified to be correlated with spasticity at 3 months.
RESULTS
Demographics and stroke characteristics
During the study period, a total of 9,659 stroke patients were screened, and 6,675 patients were included whereas 2,984 patients were excluded (i.e. did not want to participate, wrong diagnosis, did not contact patient and caregivers at 3 months after first-ever stroke). Demographic and clinical data are summarized in Table 1. Mean age of the participants was 68.3 ± 13.5 years, older than non-participants. Mean age of the non-participants was 66.4 ± 13.5 years. The proportion of women was 45.7% and men 54.3%. The stroke type was ischemic in 80.0%, and hemorrhagic in 20.0% of the participants. Stroke severity by NIHSS at admission was 4.8 ± 7.0 in participants and 4.7 ± 7.0 in non-participants. There were no significant differences between participants and non-participants except age.
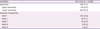
Table 1
Demographics and stroke characteristics of participants and non-participants
All values are expressed as mean (± standard deviation) or number (%).
NIHSS, National Institute of Health Stroke Scale.
*p < 0.05 compared with the independent group.
![]()
Prevalence of spasticity
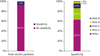
The prevalence of spasticity at 3 months after first-ever stroke is shown is Table 2. Of 4,658 eligible patients, 339 (7.3%) had MAS ≥ 1 in the upper and/or lower extremities at 3 months after stroke onset (Fig. 2). Distribution of severity of spasticity showed as MAS I (4.6%), MAS I+ (1.7%), MAS II (0.7%), MAS III (0.2%), and MAS IV (0.1%) among all participants. In the spastic patient group, 312 out of 339 patients (92.0%) had spasticity in the upper extremity while 200 (59.0%) had spasticity in the lower extremity.
Risk factors associated with spasticity
Spasticity data and their relations to other variables are summarized in Table 3. Correlated risk factor of spasticity was stroke type (p = 0.023). Hemorrhagic stroke was more frequent in spastic patients (25.2%) than non-spastic patients (20.1%). NIHSS score at 7 days after stroke onset was higher (13.3 ± 8.2) in spastic patients than in non-spastic patients (3.7 ± 5.8) (p < 0.001). NIHSS score at 3 months after stroke was higher (10.0 ± 8.0) in spastic patients than in non-spastic patients (2.1 ± 4.5) (p < 0.001). mRS at 3 months after stroke was higher in spastic patients than non-spastic patients (p < 0.001). There was no significant correlation of cerebrovascular risk factors (hypertension, diabetes, coronary heart disease, atrial fibrillation, left ventricular hypertrophy, peripheral artery disease, hyperlipidemia, low cholesterol, unruptured intracranial aneurysm, arteriovenous malformation, family history of stroke, smoking and alcohol consumption) between spastic patients and non-spastic patients.
Table 3
Correlated risk factors of spasticity at 3 months after stroke occurrence
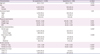
All values are expressed as mean (± standard deviation) or number (%).
BMI, body mass index; NIHSS, National Institute of Health Stroke Scale; mRS, modified Rankin Scale.
*p < 0.05 compared with the independent group.
![]()
DISCUSSION
This study investigated the prevalence of spasticity in Korean first-ever stroke patients as well as risk factors for spasticity, and difference in functional status due to spasticity at 3 months after stroke occurrence. Among 9,659 screened stroke patients, 6,675 patients met the eligibility criteria while 2,984 excluded patients did not meet the criteria. To determine the prevalence of spasticity, 4,658 stroke patients were enrolled in this study, and 7.3% of these patients showed spasticity. Spasticity was more frequent in the upper extremities than the lower extremities.
In a previous study using MAS, 21% of patients showed spasticity at initial evaluation (mean: 5.4 days after stroke), 19% at 3 months, 21.7% at 4 months, and 42.6% at 6 months [21]. In another studies using MAS, 20%–25% of all patients with first-ever stroke became spastic [15]. Our results report relatively low prevalence (up to 7.3%) (Table 2), which may be due to differences in tested joint, time of evaluation after stroke, and hospital characteristics compared with previous studies. The particularly low prevalence rate noted in this study may be because many patients with mild to moderate severity of stroke symptoms were transferred to the department of rehabilitation medicine.
Until now, few studies investigated small numbers of patients only once in a few months after a stroke. They stated that spasticity was rarely presented during the first month after stroke occurrence but reached its peak 1–3 months after a stroke [22]. Electromyography (EMG) studies have shown similar results that the reflex-mediated resistance increase in muscle tone reaches its maximum between 1–3 months after stroke. Especially after 3 months, the eventual increased resistance to passive stretch is proposed to be due to intrinsic changes of the muscles [23]. Another Swedish study [21] has shown that patients, who became spastic 3 months after stroke, had significantly worse movement function and activity performance than 3 months before (or acute phase) without spasticity. Therefore, we focused on spasticity at 3 months after first-ever stroke in this study.
The initial evaluation findings were considered to be important indicators for planning rehabilitation programs and in optimizing prognoses. In clinical practice, spasticity related risk factors should be identified for better understanding of the course of spasticity. The results of this study revealed associated risk factors of spasticity are stroke type and severity of functional limitation during intensive care phase. Hemorrhagic stroke was more common in patients with spasticity than in non-spastic patients at 3 months after stroke occurrence. In general, hemorrhagic stroke could be related to have severer functional limitations compared with ischemic stroke. In previous studies, an association of acute spasticity with the brainstem, the cerebral cortex (in primary, secondary and supplementary motor area [SMA]) and the spinal cord (pyramidal tract) [24]. Spasticity occurred more often in patients with severer functional limitations. High NIHSS score at 7 days and 3 months after stroke and high mRS at 3 months after stroke were predictive factors of spasticity in this study.
In a previous report, poor functional status and early arm or leg weakness were significantly predictive of abnormal tone, whereas young age, poor functional status, left-sided weakness, smoking history, and severe hand paresis were significantly predictive of more severe muscle tone problems [25]. In another trial, 49 subjects were examined for muscle tone (assessed by MAS), global disability (assessed by mRS), stroke severity, paresis severity, and sensory disturbance (all assessed by the NIHSS) and risk factors were determined for prevalence of spasticity [4]. Similar to findings of other studies, associated risk factors of spasticity were observed, like poor functional status after stroke, but other variables among cerebrovascular risk factors were not found to be significant in this study. These findings demonstrated various risk and predictive factors associated with the development of spasticity as well as the consideration of these factors for therapeutic intervention.
Previous studies have assessed motor function recovery according to the presence of spasticity [26] because spasticity may aggravate motor dysfunction, and delayed motor function recovery can affect on spasticity development. In our results, NIHSS and mRS scores were higher in the spastic patient group.
This study has several limitations. First, some of true population-based stroke patients were lost at 3 months after stroke. Some eligible spastic patients could not be assessed due to contact interruption, not wanting to participate, poor general condition, or death, etc. In addition, participants were older than non-participants statistically. Second, detailed data on rehabilitative intervention received after stroke was not collected, nor its relationship with functional status correlated with spasticity at 3 months after stroke. Third, medication history, especially muscle relaxant (e.g. baclofen, dantrolene, tizanidine, botulinum toxin injection) was not investigated. Forth, the patients with ankle clonus were not excluded. Clonus can be seen with spasticity, but it is not co-exist in all patients with spasticity. Fifth, general risk factors (e.g. pain, incontinence, constipation, infections, inflammation and pressure sores) were not considered.
CONCLUSION
This study has clinical significance. It showed 7.3% prevalence of spasticity in Korean first-ever stroke patients at 3 months, and identified those who carried higher risks of developing spasticity who would particularly benefit from preventive or therapeutic strategies. Risk factors were hemorrhage stroke, higher scores of mRS and NIHSS in acute phase. In the future, prospective studies including timing of initiation, duration, quantification of rehabilitative interventions during post-stroke phase and its association with spasticity are needed to support the result of this study.
 XML Download
XML Download