

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Deep vein thrombosis (DVT) is one of the most common complications in stroke patients [1]. Thrombosis formation is caused by abnormality of blood flow, vessel wall, and blood clotting components [2]. Prolonged immobilization of affected limb in patients with brain lesions leads to abnormal blood flow or venous stasis, thereby increasing the risk of thrombi formation. It is reported that DVT incidence in acute ischemic stroke patients is up to 75% [3]. Approximately 20% of DVT confined in calf vein spread to proximal veins and half of these proximal DVT induce pulmonary embolism (PE). About 25% of patients with venous thromboembolism (VTE) die within 7 days from the onset. PE is a life-threatening complication, where the 3-month mortality rate of PE patients is as high as 11.1% [456]. Therefore, early detection and control of DVT are crucial.
Clinically, DVT typically manifests symptoms and signs such as leg swelling, tenderness, pain, warmth or red discoloration [7]. Due to cognitive dysfunction or decreased mobility, patients with brain lesions cannot express or report their symptoms or signs themselves. Therefore, above mentioned clinical features may be obscure making early detection and diagnosis rather difficult. However, it is important to take appropriate screening in advance to prevent further life threatening complications. D-dimer test, which is non-invasive, convenient, and fast, can be a useful to screen patients with suspected DVT. However, it has 88% of high sensitivity but relatively 48% of low specificity [89], indicating that laboratory test cannot be superior to physical examination. Also, the D-dimer level gets affected in some conditions, such as increasing age, female sex, active malignancy, pregnancy, operation, hemodialysis, infection, and warfarin use [10]. Unilateral lower limb swelling is one of the major clinical features in DVT, that is easily detected by physicians irrespectively to patients' level of cognition. Haeger and Sjukhuset [11] reported that this sign is positive in 83% of DVT patients. However, the use of it as a screening tool in DVT is not yet studied. It is not thought to be specific [9].
The purpose of this study can be described in 2 folds. Firstly, to validate if the presence of unilateral lower extremity swelling can be used as a single predictor of DVT among patients with brain lesion. Secondly, to identify the correlation between lower extremity swelling with confirmed DVT to the patients' functional outcome. Effect of other factors such as infection and type of administered medication, and location of DVT, which may directly affect the degree of lower extremity swelling were analyzed separately, in order to exclude possible confounding effect.
MATERIALS AND METHODS
Subjects
All 621 inpatients in our rehabilitation unit were tested for D-dimer. Medical records of 194 inpatients, who had initially elevated plasma D-dimer level (> 0.55 mg/L) and underwent enhanced DVT computed tomography (CT) between May 12th, 2011 and December 30th, 2015 were reviewed, retrospectively. Among them, 79 patients who did not have brain lesion with spinal cord injury, or generalized edema due to medical deconditioning; congestive heart failure, liver cirrhosis, and renal failure, or DVT in both sides were excluded from this study. Irrespective of diagnosis of DVT, a total of 115 patients were finally recruited in our study.
Methods
Baseline parameters of each subject including gender, age, preexisting medical comorbidities, elapsed time from onset, blood test, and urinary analysis, and results of imaging studies were collected. We also investigated clinical data on characteristics of DVT such as location and presence of PE. The popliteal vein, which was classified as a proximal vein, was regarded as the border between proximal and distal vein [12]. In addition, we obtained patients' range of mobility and cognitive function such as Medical Research Council (MRC) scale, Modified Ashworth Scale (MAS), Motricity Index (MI), Berg Balance Scale (BBS), Korean version of Mini-Mental Status Examination (K-MMSE), Global Deterioration Scale (GDS), and Korean-modified Barthel index (K-MBI). Brain lesions were group by its etiology such as infarction, hemorrhage, or tumor. When patients were transferred or admitted to our department, D-dimer test (latex test BL-2P-FDP; Biolinks Co. Ltd., Tokyo, Japan) essentially was performed routinely on the first day. If D-dimer level was elevated (> 0.55 mg/L), DVT CT was performed on a 64-channel multidetector row (Discovery CT750 HD; GE Healthcare, Milwaukee, WI, USA) within a day or 2 from the D-dimer test date. Each slice thickness was 5 mm, and the images were saved to Digital Imaging and Communications in Medicine (DICOM)-images in Picture Archiving and Communications System (PACS). To measure both leg circumferences in CT image, the images were analyzed using NIH ImageJ version 1.49v software [13]. The circumference of bilateral lower limbs, below 10 cm and above 15 cm from the prominence of tibial tuberosity, were measured, respectively [14] (Fig. 1). Also, we measured cross section area (CSA) of the deep fascial membrane in bilateral lower limbs to compare with muscle atrophy in both sides. To increase reliability, one measurer who never know patients' medical history and present status repeated 2 times and had a time gap of 2 days. The difference of 2 cm or more between both sides was regarded as significant unilateral leg swelling [15].
 | Fig. 1Measurement of the circumference of bilateral lower limbs. Thick arrows show DVT in right sural vein and thin arrows indicate normal left sural vein.
DVT, deep vein thrombosis.
|
We divided enrolled patients with DVT group and non-DVT group. The presence of unilateral leg swelling in 2 groups was recorded.
All of the evaluation tools such as MRC scale, MAS, MI, BBS, K-MMSE, GDS, and K-MBI were assessed at the time of transfer or admission to our department along with D-dimer test. Static and dynamic balance using BBS; the degree of motor weakness using the MRC scale and MI; spasticity using MAS; cognitive function using K-MMSE and GDS; activities of daily living using K-MBI were assessed.
The existence of urinary tract infection (UTI) was defined as positive with pyuria (> 8 leukocytes per high-power field) or with bacteriuria (positive nitrite or > 1 organism per oil-immersion field) from urinalysis along with D-dimer test [16]. Presence of pneumonia was confirmed based on the results of patients' sputum culture and history of using antibiotics along with radiologically confirmed evidence. Use of medication affecting blood clotting was identified by the previous prescription. In DVT group, the correlation between the existence of leg swelling and scores of each evaluation were analyzed.
Statistical analysis
The descriptive statistics were calculated and presented as counts and percentages for categorical variables and as a mean ± standard deviation for continuous variables. Distribution of DVT group and the non-DVT group were identified by independent t-test and Pearson χ2 test. Reliability analysis of repetitive measurement of both lower limbs was performed. Independent t-test was used to identify the difference in leg circumference in 2 groups. In DVT group, independent t-test was performed to identify the difference in CSA of the deep fascial membrane in both sides. Fisher's exact test was performed to identify a correlation between the circumference of lower limbs with the present state of patients, including the use of anticoagulant/antiplatelet agents, spasticity, the presence of UTI, pneumonia, and location of DVT. Independent t-test was performed to identify a correlation between the existence of unilateral leg swelling and functional outcomes. Values of p < 0.05 were considered to indicate statistical significance. Statistical analyses were performed with SAS Enterprise Guide 5.1 for Windows (SAS Institute, Cary, NC, USA).
RESULTS
A total of 115 patients met the inclusion criteria. Among them, 35 patients were diagnosed with DVT by imaging studies. Average age, sex, the value of D-dimer, treatment, infection such as pneumonia and UTI, medication affecting blood clotting and brain lesion were shown in Table 1 with distribution based on demographic features. If the patient had an operation, the possibility of DVT was increased (p = 0.041). The identity of repetitive measurement was identified (p = 0.999).
Table 1
Baseline characteristics of enrolled patients
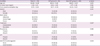
The data are reported as the mean ± standard deviation or the numbers (percentages).
DVT, deep vein thrombosis; UTI, urinary tract infection; PLT, platelet.
*p < 0.05.
![]()
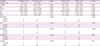
In independent t-test, there was neither significant relationship between unilateral lower limb swelling nor the presence of DVT in distal and proximal limbs (proximal, p = 0.330; distal, p = 0.405) (Table 2).
Table 2
Difference of leg circumference in patients with brain lesions

The data are reported as the mean ± standard deviation. p values were calculated using the independent t-test.
DVT, deep vein thrombosis; CI, confidence interval.
![]()
In DVT patients (n = 35), there was the neither statistically significant difference in CSA of the deep fascial membrane in both sides (Table 3) nor correlation between lower limb swelling and other covariates of patient group (Table 4).
Table 3
Difference in CSA of deep fascial membrane in both sides in DVT patients

The data are reported as the mean ± standard deviation.
CSA, cross section area; DVT, deep vein thrombosis; CI, confidence interval.
![]()
Table 4
Association between patients' status and unilateral low limb swelling in DVT patients
The data are reported as mean ± standard deviation or numbers. p values were calculated using the Fisher's exact test.
DVT, deep vein thrombosis; K-MMSE, Korean version of Mini-Mental Status Examination; GDS, Global Deterioration Scale; K-MBI, Korean-modified Barthel index; MI, Motricity Index; BBS, Berg Balance Scale; MRC, Medical Research Council; UTI, urinary tract infection.
![]()
DISCUSSION
The results of this study show that lower extremity swelling cannot be used as a single predictor of DVT presence among patients with brain lesion. The degree of leg swelling did not correlate with the actual presence of DVT. Moreover, there was no association between lower limb swelling and functional ability within DVT patients.
We presume that similar circumference of both lower limbs, despite DVT on one side, may be related to muscle atrophy in the hemiplegic side. Morphological study of skeletal muscles of hemiplegic patients has reported that muscle atrophy is caused by disuse, loss of central trophic effect or neurogenic atrophy [17]. According to the mobility of the patient, skeletal muscles can change in size. Prolonged immobilization leads to rapid skeletal muscle loss and decline in functional strength [1819]. Wall et al. [20] reported that the loss of muscle mass and strength occurs as quick as 5 days from the onset of disuse and a substantial increase in skeletal muscle lipid content is not accompanied. In this study, among 35 DVT patients, 23 patients had thrombosis in weaker limb, at least MRC one grade and 12 patients had the same grade in both limbs. To identify this presumption, we measured deep fascial CSA of both proximal and distal lower limbs. However, CSA in DVT side was not always smaller than that in the non-DVT side (Table 3).
At the distribution of patient and control group, recent history of neuro and/or orthopedic which were performed in operation room under general anesthesia, affected the occurrence of DVT (odds ratio [OR], 2.343; confidence interval [CI], 1.026–5.347). Heit et al. [4] reported that hospitalization with surgery is one of the risk factors of DVT and higher at risk than hospitalization with conservative care.
Pambianco et al. [3] found that it has a higher prevalence of DVT on admission to rehabilitation unit than subsequent incidence. His study showed that 21% had a DVT on admission, whereas only 5.5% diagnosed DVT during the study. This means a need for initial screening test in DVT. On admission or transfer to the rehabilitation unit, all of the patients should be ruled out DVT. As a tool for screening DVT, D-dimer assay is a useful test. Kuwashiro et al. [21] reported that D-dimer level was found to be useful for DVT screening in stroke patients and recommended that stroke patients with high D-dimer level (≥ 5.5 mg/L) should undergo imaging study. For a definite diagnosis, it is essential to evaluate imaging studies, such as duplex ultrasonography (DU), CT venography (CTV), and magnetic resonance imaging (MRI) venography [622]. In our study, CTV was performed in patients with suspected DVT. The advantage of DU is non-invasive without radiation and contrast material. However, it is time-consuming to evaluating distal vein and dependent on the operators' experience. Also, small isolated thrombi in calf vein may be easily ignored. Chang et al. [23] concluded that CTV could evaluate venous disorder in pelvis and abdomen and be easily performed than DU and detect other possible causes of leg swelling, which are difficult to DU.
In our study, 26 of the 35 patients with DVT did not have unilateral leg swelling. Nine of 35 among those were diagnosed with DVT in proximal vein and 26 of 35 among those in only distal vein. One of 9 patients in proximal DVT were concomitant with pulmonary thromboembolism (PTE) whereas 4 of 26 patients in distal DVT. Moser and LeMoine [24] reported that distal DVT has a low risk of PTE, contrary to proximal DVT. However, it was diagnosed more in distal DVT than proximal DVT in our study. The reason for the distinction of that is not clear. These results show that distal DVT should not be overlooked as it can also cause PTE.
The possible limitations of this study were, first, patients with normal D-dimer value did not include in our study, so comparison with leg circumference of patients with normal D-dimer value was not carried out. Second, few patients were shown with unilateral leg swelling, which exceeded 2 cm of difference in both sides. Only 7 patients in proximal part and 4 patients in distal were shown unilateral leg swelling. This was a limitation of this study but met conclusion that leg swelling was not seen in DVT patients in stroke. Third, the retrospective nature of this study can be considered as a limitation. Finally, because the circumference of both lower limbs was measured by a manual technique, it might present a measurement error. However, we repeated measurement by intraobserver agreement to reduce error. Moreover, we had a time gap, 2 days, to reduced bias.
In conclusion, swelling in the lower limb, itself, is not a definite sign of DVT and may rather confuse physicians to miss the diagnosis of DVT which can lead to the life-threatening condition by causing complication such as PTE. Therefore, evaluation of DVT is warranted based on clinical presumptions such as elevated D-dimer, decreased mobility, and history of recent surgery, even among patients without noticeable leg swelling.
 XML Download
XML Download