

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Reactivation of the varicella-zoster virus (VZV) in the geniculate ganglion is responsible for herpes zoster oticus. When this reactivation is associated with facial nerve palsy and vestibulocochlear symptoms, it is called Ramsay Hunt syndrome (RHS) [1]. Although multiple lower cranial nerves (CNs), including the glossopharyngeal nerve (CN IX), vagus nerve (CN X), and hypoglossal nerve (CN XII), may be involved in RHS, dysphagia has rarely been described. We reported a rare case that presented with severe dysphagia due to cranial polyneuropathy involving trigeminal nerve (CN V), facial nerve (CN VII), vestibulocochlear nerve (CN VIII), CN IX, CN X, and CN XII in RHS and discussed the prognosis of RHS-related dysphagia and rehabilitation according to a literature review. This report was approved by the institutional review board of the hospital and written informed consent was obtained from the patient.
CASE REPORT
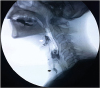
A 74-year-old male patient had progressive left facial paralysis, ear pain, and vertigo that had persisted for 3 days prior to his hospital visit. He was admitted to the Department of Otolaryngology. He complained of difficulty in swallowing saliva, convulsive cough and dysphonia. Physical examination showed House-Brackmann scale (HBS) grade IV left facial palsy without any facial skin eruption. Facial hypoesthesia and a decreased gag reflex were also noted on examination. Meanwhile, multiple vesicular eruptions on the cymba concha were evident in the left ear and flexible laryngoscopy revealed true vocal cord paralysis (Fig. 1). However, neither pure tone audiography nor brain magnetic resonance imaging (MRI) showed any abnormalities. In a nerve conduction study (NCS), the amplitude of the left facial muscles was reduced by approximately 83.5% compared to the right side and showed a considerable latency delay. A blink reflex study revealed incomplete injury of both CN V and CN VII on the left side. Based on clinical manifestations, neurologic exams and other tests, the involvement of CN V, CN VII, CN VIII, CN IX, and CN X was confirmed. He was treated with oral valaciclovir hydrochloride (3,000 mg/day) and methylprednisolone for 5 days. Then, he was referred to the department of rehabilitation medicine to manage dysphagia.
 | Fig. 1(A) Vesicular eruptions on the cymba concha (left) on rigid telescopic examination. (B) Laterally fixed left vocal cords on flexible laryngoscopic examination.
|
Swallowing function was evaluated in a videofluoroscopic swallowing study (VFSS) at 2 weeks from symptom onset. Significant abnormalities were discovered in the parameters of the pharyngeal phase, including triggering of pharyngeal swallow, vallecular and pyriform sinus residue, laryngeal elevation, coating on the pharyngeal wall, pharyngeal time, and aspiration tested by both thick and thin liquids (Fig. 2). Although tongue deviation was not observed in the neurologic examination, partial invasion of CN XII was suspected based on poor laryngeal elevation in VFSS findings. The quantified severity based on the VFSS was calculated as the videofluoroscopic dysphagia scale (VDS) score, which was created according to the odds ratios of various prognostic factors for a possible total score of 100 points [2]. The patient's initial VDS score was 66.5, indicating severe dysphagia. He complained of severe esophagitis and was discharged with a percutaneous endoscopic gastrostomy (PEG) 2 weeks after the onset and began receiving swallowing rehabilitation 5 times per week on an outpatient basis. Swallowing rehabilitation consisted of oromotor stimulation, neuromuscular electrical stimulation (NMES) therapy and exercise training, including the Mendelsohn maneuver, Shaker exercise and Masako maneuver, to improve laryngeal elevation. The entire rehabilitation program was performed for 1 hour per day. After 6 weeks of rehabilitation, facial palsy remained and a blink reflex study without facial NCS was conducted. The latency of ipsilateral R1, R2 of the left side and contralateral R2 of both sides had slightly improved, but were still prolonged. At that time, a VFSS showed improvement in items of bolus formation, tongue to palate contact, oral transit time, vallecular residue, and pharyngeal wall coating. Additionally, no aspiration was evident, but penetration was observed in fluid and solid properties. His VDS score improved to 38.5. Therefore, PEG removal was performed and a modified diet with increasing viscosity from liquid to nectar and pudding with thickening agent was implemented [3]. At 3 months from the onset, facial nerve palsy improved to HBS grade II, and swallowing function returned to normal with a VDS score of 6.5. The remaining abnormal findings were delay of pharyngeal triggering and less than 10% vallecular residue.
DISCUSSION
The patient in this case exhibited cranial polyneuropathy that spread throughout CN V, CN VII, CN VIII, CN IX, and CN X. CN XII also appeared to be partially involved considering poor laryngeal elevation in VFSS findings. Concurrent involvement of CNs such as CN V, CN IX, CN X, CN XI, and CN XII is rare, but leads to various symptoms of neurological deficits including impaired eye movement, trigeminal neuralgia, swallowing difficulty, hoarseness, and tongue deviation. Although the mechanisms are unclear, vasculitis in the carotid, middle meningeal, and ascending pharyngeal arteries, which can be infected by the direct perineural spread of the VZV along anastomotic pathways, may contribute to the development of cranial polyneuropathy in RHS [4]. The involvement of multiple CNs in RHS results in greater loss of function and is associated with a poor prognosis relative to facial nerve palsy regardless of the initial HBS grade. In one study, patients without multiple cranial neuropathies showed a recovery rate of 82.9%, whereas patients with multiple cranial neuropathies had a recovery rate of 54.5% [5].
Dysphagia is an especially rare complication in patients with RHS-related cranial polyneuropathy, and previous reports are summarized in Table 1. It is important to determine the prognosis because a PEG may be required to prevent aspiration pneumonia, if extensive recovery time is required for dysphagia. However, the clinical course and predictive factors for the prognosis of dysphagia in RHS remain unknown despite their significance. Therefore, we conducted a literature review and analyzed some evaluation tools. The amplitude of motor action potentials in an NCS and the HBS scale are known as valuable methods for predicting the outcomes of facial palsy [6]. However, swallowing function was restored within a relatively short period, despite severe neural degradation according to the NCS in this case and in a case reported by Shim et al. [7] Additionally, the initial severity of RHS-related dysphagia based on the results of a VFSS or a flexible endoscopic evaluation of swallowing (FEES) may not affect prognosis, as in this case and in previous reports [78910], in contrast to stroke-related dysphagia. Therefore, electrodiagnostic studies and VDS scores representing the initial severity of dysphagia cannot be used to predict the prognosis of dysphagia in RHS.
Table 1
Summary of the literature related to dysphagia in RHS

| Study | Age | HBS | Involved CN | NCS | VFSS | Swallowing therapy | Recovery time (mon) |
|---|---|---|---|---|---|---|---|
| Lee et al. (this case) | 74 | 4 | V, VII, VIII, IX, X, possibly XII | Yes | Yes | Yes | 1.5 |
| Shim et al. [7] | 48 | N/A | VII, VIII, IX, X | Yes | Yes | Yes | 1 |
| Coleman et al. [8] | 81 | 4 | V, VII, VIII, X, possibly XII | No | FEES | Yes | 8 |
| Kim et al. [9] | 73 | N/A | VII, VIII, IX | No | Yes | Yes | 2 |
| Bharadwaj et al. [10] | 90 | 2 | VII, VIII, IX, X, XII | No | Yes | Yes | 12 |
| Shinha and Krishna [14] | 66 | N/A | VII, VIII, IX, X | No | No | No | N/A |
| Wang and Chen [15] | 25 | N/A | VII, VIII, XII | No | No | No | 1 |
| Nishioka et al. [16] | 78 | N/A | III–XII | No | No | No | 12 |
| Miyazaki et al. [17] | 85 | N/A | VII, VIII, IX, X | No | No | No | N/A |
| Morelli et al. [18] | 82 | N/A | V, VII, VIII, IX, X, XI, XII | No | No | No | 2 |
| Van Den Bossche et al. [19] | 25 | N/A | IX, X, XI | No | No | No | 1.5 |
RHS, Ramsay Hunt syndrome; HBS, House-Brackmann scale; CN, cranial nerve; NCS, nerve conduction study; VFSS, videofluoroscopic swallowing study; FEES, flexible endoscopic evaluation of swallowing; N/A, no available information in the literature.
![]()
Nevertheless, all patients discussed in previous reports, including this case, recovered swallowing function, enabling oral intake, regardless of age and the CNs involved. Although the observation periods varied from 4 weeks to 1 year, the overall outcome of dysphagia in RHS seemed good. Furthermore, we found that patients who received swallowing rehabilitation therapy recovered swallowing function more quickly compared to those who did not receive therapy. Oral feeding was possible within 2 months through swallowing rehabilitation, including the patient in this case, except for 2 cases in which the patients were more than 80 years old [78910]. Elderly patients tend to exhibit greater loss of function, resulting in a difficult recovery [8], and severe cases appear to require a significant amount of time for recovery.
NMES therapy for cervical swallowing muscles can serve as a therapeutic supplement to known interventions in the treatment of dysphagia. The rationale for applying NMES is to stimulate muscle fibers by stimulating the nerve and the motor end plate of the nerve, resulting in the re-education of functional muscle contraction patterns. NMES is commonly applied in post-stroke dysphagia, but is also effective for dysphagia patients of various etiologies [1112]. Exercise rehabilitation for dysphagia consists of exercises to train specific muscles associated with swallowing. The effortful swallowing and the Masako maneuver can increase tongue base retraction and reduce laryngeal residue. Laryngeal elevation can be increased through the Mendelson and Shaker maneuvers [13]. Despite the lack of evidence, rehabilitation therapy seems to partially improve swallowing function in RHS patients. Further studies are required to determine the mechanisms of swallowing recovery after RHS with cranial polyneuropathy.
We encountered a rare case of cranial polyneuropathy manifesting severe dysphagia, and attempted to predict the prognosis of dysphagia in RHS through a literature review and some assessment tools. Although no valuable predictors for recovery have been found, the prognosis for dysphagia in RHS seems favorable. Additionally, swallowing rehabilitation therapy could be beneficial in expediting tube removal.
 XML Download
XML Download