

 PDF
PDF Citation
Citation Print
Print


INTRODUCTION
Unilateral spatial neglect is a disorder of spatial attention that affects spatial perception, mental imagery, and motor action planning and execution. It occurs as a result of brain diseases such as stroke, with about 50% of all cases involving a right brain injury and 30% involving a left brain injury [123]. Patients with unilateral spatial neglect show inaccurate and slow responses to contralateral stimuli and have difficulty not only with personal hygiene, ambulation, and wheelchair manipulation, but also with reading and social interaction due to hampered motor action [45]. For this reason, patients with spatial neglect have poorer rehabilitation outcomes, higher safety risks during their hospital stay, and longer hospital stays for rehabilitation than those without spatial neglect [67]. Objective and consistent assessment of unilateral spatial neglect is highly critical in rehabilitation medicine, because the ultimate goal of rehabilitation is to improve the patient's competence for daily living by enhancing functional capacity and ameliorating the environment. Hence, an instrument that enables an accurate assessment of the severity and changes of unilateral spatial neglect is essential to meet the goals of rehabilitative therapy and to facilitate communication among patients and medical staff.
However, functional assessment of daily living activities for elucidating hemispatial neglect has been neglected in Korea, as demonstrated by a study examining the trends of purpose-specific assessment tools used by Korean occupational therapists [8]. According to this study, the line bisection test was the most popular (47.9%) for the diagnosis of hemispatial neglect in Korea, followed by the Albert's test (36.8%). The Behavioral Inattention Test, a functional test, was rarely used (2.6%), and the Catherine Bergego Scale (CBS) was not included in the list. These paper-based tests, while widely used in clinical practice, have limitations in the evaluation of functional performance of spatial neglect on the activities of daily living, and may underdiagnose auditory or proprioceptive spatial neglect [9]. CBS has been proposed for these functional assessments and CBS has been used to assess functional aspects, mental imageries, and motor performance as well as personal (body surface), peripersonal (within arm's reach), and extrapersonal function [10]. However, CBS has not been widely applied in clinical practice in Korea because the evaluation guidelines and scoring standards for each subscale are not presented objectively [8].
The Kessler Foundation Neglect Assessment Process (KF-NAP) is an assessment tool for unilateral spatial neglect that was developed by the Kessler Foundation. The KF-NAP addresses the limitations of the CBS, and assesses the perception of left and right space and asymmetrical behaviors by directly observing patients while they voluntarily explore space with eye and head movements in their daily lives. The KF-NAP has been reported to not only assess daily living functions, but also the presence and severity of spatial neglect, and to predict independent functional outcomes at discharge [11]. Thus, we aimed to develop the Korean version of the KF-NAP, which enables a more functional assessment of unilateral spatial neglect, through Korean translation followed by statistical standardization.
MATERIALS AND METHODS
Participants
Thirty patients with brain disease, including stroke and traumatic brain injury, who had spatial neglect symptoms and were diagnosed at the Konkuk University Medical Center were enrolled in the study. The mean age of the participants was 66.3 ± 13.7 years, with 20 men and 10 women. We enrolled 7 patients with cerebral hemorrhage, 21 with cerebral infarction, 1 with traumatic brain injury, and 1 with a brain tumor (Table 1). All patients were cognitively and linguistically capable of understanding the examiner's questions and instructions. We excluded patients who were incapable of performing a 2-stage or higher command because of severe cognitive dysfunction, patients who were incapable of performing daily living activities, and patients with hemianopia.
Table 1
Clinical characteristics of participants (n = 30)
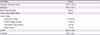
Values are mean ± standard deviation or number (%).
K-MBI, Korean-Modified Barthel Index; K-MMSE, Korean Mini-Mental State Examination.
![]()
Development of the Korean KF-NAP
Two rehabilitation specialists individually translated the English version into Korean. Both were familiar with the English language, and 1 of them had lived in the United States for more than 10 years and was bilingual in both English and Korean. After this, 1 rehabilitation specialist who did not participate in the first round of translations and a bilingual linguist with native proficiency in English and Korean discussed and analyzed the differences between the 2 translations and integrated them into a single copy. The copy was back-translated by an English-native bilingual translator and sent to the original developers to identify any discrepancies with the original KF-NAP to finalize the Korean version of the KF-NAP.
Preparation of video material to assess the Korean KF-NAP
The entire process of administering the Korean KF-NAP to 30 patients was video-recorded to conduct statistical verification and to use as education material in the future. Each video comprised the 10 criteria of the KF-NAP, which are as follows: limb awareness, personal belongings, dressing, grooming, gaze orientation, auditory attention, navigation, collisions, meals, and cleaning after meals. The video took about 20 minutes per case. As per the Korean KF-NAP evaluation guidelines, the entire process was conducted in the patient's ward, a place familiar to the patient. One occupational therapist delivered the questions and instructions, and the patient's responses were recorded. The patient or the patient's family was fully briefed about the entire process prior to the assessment, and consent for video recording was obtained.
Analysis of the reliability and validity of the Korean KF-NAP
The 30 videos were evaluated in the assessment of the Korean KF-NAP by 5 occupational therapists from 4 university hospitals nationwide. Anyone who participated in the preparation of the videos was excluded from performing these assessments. The assessment guidelines of the Korean KF-NAP were included in the video material to teach the viewers about the assessment categories and scoring method. All evaluators recorded the Korean KF-NAP scores for the 30 patients in the videos and performed a reassessment of the same videos after 2 months. Inter-rater reliability and intra-rater reliability of the 5 occupational therapists from different institutions were tested using the intraclass correlation coefficient (ICC) and Pearson correlation coefficient. Further, the internal consistency reliability of the assessment categories was examined using Cronbach's alpha coefficient. Validity was tested by performing the Albert's test and letter cancellation test, 2 makeshift tests for unilateral spatial neglect. These results were compared with those of the Korean KF-NAP using the Pearson correlation coefficient.
During the Albert's test, the patient is instructed to mark the middle of 36 straight lines that are drawn on the left-, middle-, and right-side (12 each) of a piece of A4 paper, and percent deviation is calculated by counting how many lines on the lesion side are omitted [12]. For the letter cancellation test, consonants are embedded within multiple letters on a piece of paper, and the patient must locate the target consonant. Two or more omissions on the lesion side indicate unilateral spatial neglect [13]. The KF-NAP assesses the patient's asymmetrical behavioral patterns during 10 routine daily activities (i.e., limb awareness, personal belongings, dressing, grooming, gaze orientation, auditory attention, navigation, collisions, meals, and cleaning after meals). Each item is scored as 0 (no neglect), 1 (mild neglect), 2 (moderate neglect), or 3 (severe neglect). In the case of omitted categories, the final score is calculated according to the following equation:
The severity of neglect is determined (absent, mild, moderate, or severe) based on the final score [11]. Statistical analysis was performed using SPSS 17.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p < 0.05.
RESULTS
Validity analysis
The results of the Korean KF-NAP were strongly correlated (r ≥ 0.8) with the results of the Albert test and letter cancellation test, 2 makeshift tests for hemispatial neglect (p < 0.05; Fig. 1).

Reliability analysis
Inter-rater reliability
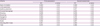
Five occupational therapists who work in different institutions performed 2 rounds of each category of the Korean KF-NAP, and inter-rater reliability of these results was analyzed using the ICC. Details are shown in Table 2. The ICCs for the first and second assessments of the Korean KF-NAP were 0.973 and 0.982, respectively, showing high reliability (p < 0.05; Table 2).
Table 2
Inter-rater reliability measured by the ICC
![]()
Intra-rater reliability
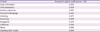
Table 3 shows the intra-rater reliability (Pearson correlation coefficient) for the 2 rounds of assessment of the categories of the KF-NAP results obtained by the 5 occupational therapists. All 5 occupational therapists displayed very high intra-rater reliability as assessed using the Pearson correlation coefficients for the KF-NAP scores exceeding 0.9 (p < 0.05; Table 3). However, some therapists showed low intra-rater consistency for some categories.
Table 3
Test-retest reliability measured by correlation coefficients

O1, occupational therapist 1; O2, occupational therapist 2; O3, occupational therapist 3; O4, occupational therapist 4; O5, occupational therapist 5.
![]()
Internal consistency
All categories of the Korean KF-NAP showed high internal consistency, with Cronbach's alpha coefficient exceeding 0.8 (Table 4).
Table 4
Internal consistency reliability of each category of the Korean KF-NAP
![]()
DISCUSSION
Visual/sensation tests or paper-and-pencil tests, such as line bisection and cancellation tests, are widely used to assess hemispatial neglect in rehabilitation medicine. Although these tests are clinically popular, they have limitations in assessing unilateral spatial neglect in patients' daily living, and it is difficult to diagnose unilateral spatial neglect related to auditory, proprioceptive, or motor functions [11]. For this reason, the tests used to confirm the presence of hemispatial neglect in the clinical setting have a low sensitivity, and clinicians show low consistency in their assessments [14]. Thus, behavioral assessments are needed to assess the clinical manifestations of hemispatial neglect in patients' daily lives so as to comprehensively examine various mechanisms and types of hemispatial neglect [15]. In a study assessing hemispatial neglect following a stroke, Azouvi et al. [14] reported that functional assessment of daily living activities, such as the CBS, had higher sensitivity than paper-and-pencil tests, including the bell test, figure copying, clock drawing, line bisection, reading, and writing.
The KF-NAP is an assessment tool for hemispatial neglect developed by the Kessler Foundation by modifying and complementing the CBS [11]. Because this tool was developed for use in the western countries, adaptation and standardization for use in Korea is needed. Assessment instruments that have been verified in one country are not useful in other countries when the same tool is simply used in a different language; such tools must be translated and modified in relation to the language and culture of the country before usage [16]. Therefore, for functional assessment of hemispatial neglect in daily life, we translated the KF-NAP into Korean, verified the inter-rater and intra-rater reliability of the translated version for standardization, and found that the resulting Korean KF-NAP is a highly reliable tool. Reliability was tested by analyzing the agreement of the raters' assessment results for each category. As those who instructed, interpreted, or executed the Korean KF-NAP, the raters assessed each category after understanding the assessment guidelines. Because the occupational therapists who performed the Korean KF-NAP only read the assessment guidelines before conducting the assessment and did not receive the same training for KF-NAP because they work in different institutions, the high consistency of test-retest results and high agreement among the raters suggest that there was a good understanding of the guidelines, which are sufficient to administer the test easily. However, in the test-retest reliability analysis, gaze orientation, personal belongings, auditory attention, collision, and meals in 1 of the 5 therapists showed a moderate correlation with Cronbach's alpha coefficient of 0.5–0.7. This may be due to the difference between the interpretation of the degree of reaction or the determination of the short-time image rather than the analysis of the patient's behavior during the whole evaluation time. Since most of the evaluators' scores showed a strong correlation, a more accurate assessment could be made if the guideline was fully understood. Furthermore, a comparison with the results of paper tests for hemispatial neglect revealed that the Korean KF-NAP has high validity and that it does not in any way fall short of the traditional paper tests in diagnosing hemispatial neglect. Overall, this suggests that the Korean KF-NAP could serve as another useful tool in the assessment of hemispatial neglect resulting from brain diseases.
In conclusion, we developed the Korean KF-NAP by translating the KF-NAP and statistically verifying it. Our findings suggest that the Korean KF-NAP enables an objective and comprehensive assessment of hemispatial neglect in Korean patients with brain diseases.
 XML Download
XML Download