

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
We present a clinical case of a 74-year-old man with a personal record of nasal polyps and sinusitis. The patient was first admitted to our Department of Neurology with symptoms of instability and dizziness of 6 months of evolution, which subsided spontaneously. Physical examination revealed amaurosis with an afferent pupillary defect in the left eye associated with conjunctival injection, with a slightly hyperemic optic nerve head and mild proptosis in that same eye, as well as paresthesia of the first branch of the trigeminal nerve on the left side of his face. The patient was hospitalized, and several analysis and diagnostic test was performed, together with a study of autoimmunity and tumor markers, CSF analysis, and brain MRI. The analysis revealed the following abnormal findings: erythrocyte sedimentation rate, 67 mm; antinuclear antibody inconclusive (1/80); positive for anti-DNA (37 UI/mL), perinuclear antineutrophil cytoplasmic antibody and antimyeloperoxidase-IgG (45 U/mL); and negative for antiproteinase 3 IgG. All other studies yielded normal findings.
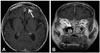
Brain MRI revealed a lesion with signs of aggressiveness in the bilateral nasoethmoid region, with an epidural component in that area, and meningeal thickening and hyperenhancement (Fig. 1). Immunohistochemical studies of a biopsy sample taken from the lesion revealed histiocytosis with foamy histiocytes (positive for CD68, and negative for S100 and CD1a), as well as intense lymphoid infiltration and eosinophils (Supplementary Figs. 1 and 2 in the online-only Data Supplement). These data confirmed the diagnosis of Erdheim-Chester disease (ECD).
Tc-99 scintigraphy was performed, but no lesions compatible with ECD were observed. A body CT scan revealed emphysematous air spaces with paraseptal and centrilobular distributions in both upper lobes. These data, together with the results of aspirometry study, confirmed an interstitial pattern.
Prednisolone was added to the treatment, which resulted in a progressive improvement of the neurological symptoms. The patient was discharged after 10 days of treatment. The patient experienced no recurrence of the symptoms during a follow-up period of 4 years.
EDC is a rare form of non-Langerhans cell histiocytosis, for which there are approximately 400 cases described in the medical literature.1 It is a systemic disease that affects mainly adults between their fifth and seventh decades of life; the prevalence is slightly higher in men.2 ECD is diagnosed through the assessment of clinical symptoms and radiological and histological criteria. The main diagnostic criteria are histological, and are usally sufficient to confirm the disease.2 The histology of ECD is characterized by histiocytic infiltration with special histiocyte that do not contain Birbeck granules, and an immunohistochemical profile that is characterized by positivity to CD68 and negativity to CD1a and S100.3
The cardinal sign of ECD is bone involvement, which is observed in 96% of patients.1 CNS involvement occurs in 51% of the patients with ECD, and is responsible for 29% of all deaths due to the disease.1 The neurological clinical symptoms, in lowering order of frequency, are diabetes insipidus, exophthalmos, cerebellar ataxia, panhypopituitarism, and papilledema.2 Brain MRI describes two patterns: infiltrating and nodular thickening of the dura mater; the former is the most frequently observed.4
The low prevalence of this disease means that no standardized treatment has yet been established.4 However, there are now some first-line drugs, such as interferon-α, which exert positive effect on survival.1 However, the beneficial effects of interferon-α have yet to be clarified.4 Corticoids are used to control the symptoms of ECD.2 Vemurafenib (a BRAF inhibitor) induces a fast clinical improvement in patients who are positive for the BRAF V600E mutation, which is found in 54% of ECD patients.3
The average 1- and 5-year survival rates of the disease are 95% and 68%, respectively.2 Involvement of the CNS has recently been proposed as the only independent clinical prognostic factor for a poor survival.1
The patient described herein presented with neurological symptoms and lung involvement. Only an anatomopathological analysis of biopsy samples allowed a definitive diagnosis, since the patient did not present any other symptoms.
 XML Download
XML Download