

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Non-steroidal anti-inflammatory drugs (NSAIDs) have a wide range of indications in the treatment of medical and surgical diseases due to their analgesic, antipyretic and anti-inflammatory effects.1,2 They are frequently used in painful and inflammatory conditions such as rheumatologic diseases, orthopedic and gynecologic surgery and in soft tissue traumas. This group of medications is also commonly used in the clinical practice of dentistry, such as in the treatment of oro-facial pain or after oral surgical procedures.3,4
Some NSAIDs are widely used in Turkey, without prescription, for their analgesic and anti-inflammatory properties.
Naproxen, a propionic acid derivative, is a prototypical anti-inflammatory agent which is generally used for the treatment of rheumatoid arthritis, osteoarthritis, primary dysmenorrhea, ankylosing spondylitis, bursitis, tendonitis, juvenile arthritis, acute gout, fever, following dental, obstetric or orthopedic surgery, for prophylaxis and the treatment of vascular headaches. The recommended adult dosage of naproxen sodium for acute pain is 550 - 1,100 mg/day in divided doses. If necessary, the dosage may be increased up to 1,650 mg/day for a short period.5
Etodolac is a pyranocarboxylic acid-derived nonsteroidal anti-inflammatory drug (NSAID) that possesses analgesic activity. Etodolac suppresses the biosynthesis of prostaglandins by inhibition of cyclcoxygenases such as other NSAIDs. Etodolac is used in osteoarthritis, rheumatoid arthritis, tendonitis, bursitis, acute sports injuries, gout, pain of orthopedic pathologies, dysmenorrhea, postoperative pain (surgical and dental procedures) and for pain associated with non-rheumatic inflammatory conditions or vascular headaches. A dosage of 200 - 400 mgr every 6 to 8 hours is recommended for acute pain.3 Earlier studies have reported that etodolac at 50 to 400 mg/day provided dose-related relief of moderate to severe postoperative pain from a variety of surgical and dental procedures.6,7
Nimesulide is a sulfononilide nonsteroidal anti-inflammatory drug with marked anti-inflammatory, antipyretic and analgesic properties and is indicated for osteoarthritis, rheumatoid arthritis, reduction of fever, primary dysmenorrhea and for relief of mild to moderate pain. The recommended adult dosage of nimesulide is 100 mg administered orally as tablets twice daily.8
NSAIDs have severe toxic effects on the gastrointestinal and renal systems; central nervous system, otic, ocular and adverse effects (pruritis, skin eruptions, or rashes, ecchymoses, dermatitis, sweeting and photosensitivity reactions). They can cause gastric mucosal damage, which may result in ulceration and/or bleeding, although they can inhibit platelet aggregation and may prolong the bleeding time but they do not effect the prothrombin time or whole blood clotting time.5 The gastrointestinal and renal side effects of selective COX2 inhibitors are claimed to be fewer than those of the classical NSAIDs.1,2 For that reason their use has become more frequent in recent times.
Studies on the genotoxic potential of these drugs are limited. Various studies have shown that they either have only a weak or no genotoxic effect at all.9-12
Enclosed third molar surgery is one of the most common surgical interventions in oral surgery.13 NSAIDs are given after the surgical operation to prevent complaints and complications. Pharmacologic therapy plays a very important role in acute inflammation. Patients want relief from pain, so the most useful agents are those that provide analgesic as well as anti-inflammatory effects. Various drugs are commonly administered in the postoperative period for the relief of pain and oedema. For these patients, the drugs of choice are NSAIDs which are widely used in routine daily practice.
Analysis of the frequency of Sister Chromatid Exchange (SCE) is a sensitive and reliable technique for the detection of DNA damage caused by various environmental factors, such as various physical and chemical agents and drugs.14-16
In this study, the genotoxic effects of three commonly used NSAIDs were investigated using the frequency of SCEs in peripheral lymphocytes before and after drug use in patients undergoing oral surgery.
MATERIALS AND METHODS
In this prospective study, thirty consequential patients (male/female = 1, age:19 - 25 years, mean age: 21.6 ± 1.90) for whom an enclused third molar operation was planned were randomly and blindly separated into 3 groups (etodolac, naproxen sodium and nimesulid groups). The patients were non-smokers and on no other medications at the time of this study. Written and oral consents were obtained from all of patients. The first peripheric blood samples were obtained prior to commencing therapy and the second after 3 days of NSAID treatment. Patients were given either etodolac 800 mg/day, naproxen sodium 1,100 mg/day or nimesulid 200 mgr/day in two divided doses.
Peripheric lymphocytes were cultured using a modified procedure of the peripheric blood culture method developed by Moorhead et al.17 A stock medium was prepared by the addition of 20% fetal bovine serum, 1% Penicilinle-streptomycine, 1.5% PHA-M (PHA-M, Biochrom KG, Berlin, Germany) and 1% L-glutamine to 100 mL of Ham's F-10 medium (Biochrom KG, Berlin, Germany). In each culture tube, 0.3 mL of the blood sample, with heparin was added using a sterile syringe. At 24 hours, 100 microliters of the stock solution (50 µg) containing 0.5 mg/mL Bromodeoxyuridine (BrdU) (BrdU, Sigma Chemical Company, St. Louis, MO, USA) was added to achieve a final concentration of 0.5 µg/mL. After the BrdU addition the culture tubes were covered with light resistant paper and incubated for 72 hours at 37℃. After 70 hours, colchicine (0.2 µ/mL) was added.Two hours after the addition of colchicine (Colchicine powder, Sigma chemical CO, St. Louis, MO, USA) (at 72nd hours), the culture tubes were removed from the incubator. After standard harvesting procedures, slides were stained by the fluorescence plus Giemsa (FPG) method18 using Hoechst 33258 dye exposure to fluorescent black light and Giemsa staining. Every point of exchanges was counted as a SCE: terminal exchanges were scored as one SCE and interstitial ones as two SCEs (Fig. 1). The frequencies of SCE per metaphases before and after treatment for each individuals were evaluated. In this study, a statistical analysis was performed using the Kruskal Wallis and Wilcoxon tests to compare the percentage of SCE in different sample groups, which were calculated with the Graph Pad Prisma V.3 computer programme.
RESULTS
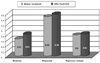
The SCE frequency per metaphase was calculated in all patients and compare within each group before and after 3 days of medication. These findings are shown in Table 1. In the Etol group, the SCE frequencies were 8.65 ± 1.56 and 8.83 ± 1.40 before and after treatment, respectively. The corresponding frequencies for the nimesulid and naproxen groups, were 9.49 ± 1.42 and 9.59 ± 1.44, and 8.8 ± 1.27 and 8.84 ± 1.14 respectively (Fig. 2). When all groups were combined, the SCE frequencies per metaphase were 8.93 ± 1.41 and 9.08 ± 1.33 before and after NSAIDs treatment, respectively. There was no statistically significant difference in the frequencies of SCE between the preoperative and postoperative values of the etodolac (W = - 21; p = 0.32), nimesulid (W = - 11; p = 0.62) and naproxen sodium (W = - 4; p = 0.82) groups. The differences between the groups before the treatment (KW = 1.69; p = 0.42) were found to be statistically insignificant. The difference between the groups (KW = 2.19; p = 0.33) after the treatment was also not significant (Table 2).
DISCUSSION
Cytogenetic markers, such as chromosomal aberrations (CAs), and micronuclei (MN), and SCE, are among the most widely used in the indication of the early biological effects of DNA damaging agents. In addition to cytogenetic markers, various molecular genetic techniques, including the Commet assay, have been used in the evaluation of mutagenicity / carcinogencity. The main difference between cytogenetic analysis and the Commet assay is the kind of changes detected. The Commet assay can detect repairable defects or alkali labile sites, whereas cytogenetic analysis can detect only chromosomal aberrations that have occurred at least one cell cycle earlier.19
Sister Chromatid Exchange can be defined as the exchange of parts between sister chromatids.20 Although the mechanism is not well understood,21 SCE is thought to occur during the replication process, and is accepted as a reliable test for the evaluation of DNA damage.22,23 Viral infections,22 cigarette smoking,24 advanced age,25,26 malignant diseases,27 medications10,11,12,28 and UV light20,26 have all been shown to increase the frequency of SCE.
In the present study, the in vivo genotoxicities of three NSAIDs, namely etodolac, nimesulid and naproxen sodium, were evaluated by SCE in peripheral blood samples. Although the genotoxicities of other NSAIDs have been evaluated in various studies,9-12 according to our knowledge, this is the first report of genotoxicity studies for etodolac and nimesulid with the use of an in vivo SCE assay.
Kullich and Klein10 reported no increase in the frequencies of SCE after 2 weeks of treatment with various NSAIDs, including diclofenac, flurbiprofen, ibuprofen, indomethacin, isoxicam, ketoprofen, piroxicam, pirprofen, and tiaprofenic acid. A study on rat bone marrow cells revealed a weak genotoxic effect of the non-selective COX2 inhibitors ibuprofen, ketoprofen and naproxen sodium.11
Özkul et al.12 reported a slight statistically insignificant increase in the frequency of SCE with the use of naproxen sodium.
In our study, the average SCE frequency per metaphase was slightly higher after treatment, without reaching statistical significance. Also, the short term use of selective (etodolac) and non-selective NSAIDs (nimesulid and naproxen sodium) were not associated with any genotoxic effect that could be detected using the SCE method in peripheric lymphocytes.
It is concluded that in the short term therapeutic application of these drugs there are no genotoxic effects on the chromosomes of peripheral blood lymphocytes. However, further studies will be required to understand the possible genotoxic effects of their long-term use.



 XML Download
XML Download