

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Familial Mediterranean fever (FMF) is an autosomal recessive autoinflammatory disease. Recurrent fever, abdominal attacks, pleural attacks, prodromes, and pericarditis are common clinical manifestations of FMF. Mutations in the Mediterranean fever (MEFV) gene encoding of a protein called pyrin appear to cause the disease in many cases. Mutations have been widely found in exons 1, 2, 3, 5, 9, and 10 of the MEFV gene. The five most frequent mutations are E148Q, M680I, M694V, M694I, and V726A (123). Whereas FMF is widely found among Mediterranean and Middle Eastern populations, sporadic cases have been reported in the Far East (4).
Abnormal innate immune system activation, which is responsible for activating inflammasome, is the main player in the pathogenesis of autoinflammatory diseases (5). The proposed molecular mechanism in the pathogenesis of FMF is increased inflammasome activation due to restricted pyrin expression (6). Inflammasomes activate caspase 1 and trigger the release of pro-inflammatory cytokines, such as interleukin-1β (IL-1β) and IL-18. These cytokines stimulate neutrophils and macrophages and induce an inflammatory response (7).
Two different phenotypes (types 1 and 2) might be seen in patients with FMF. Type 1 is characterized by short recurrent episodes of inflammation. The episodes may last from 24 to 72 hours and have variable frequency. The frequency of attacks may vary from once per week to once every 5–10 years. Approximately half of the affected individuals report experiencing a prodrome of discomfort and/or psychological uneasiness up to 24 hours before the actual attack (12). Colchicine is used in the treatment of FMF. It reduces the frequency of attacks and prevents amyloidosis (8).
Chitotriosidase (ChT) is a member of the chitinase family capable of hydrolyzing chitin. This enzyme is mainly secreted from activated and differentiated macrophages, therefore, ChT is a marker of macrophage activation (9). Human ChT is associated with Gaucher’s disease, lysosomal storage disorders, sarcoidosis, Crimean Congo hemorrhagic fever, and beta-thalassemia (10111213). It has also been indicated that ChT can be up-regulated during the immunological response in other acute or chronic inflammatory conditions (14). Therefore, we wanted to investigate whether differences in ChT concentrations or activity could be seen in patients with FMF.
The purpose of this study was to investigate the changes in the activity and concentration of ChT in FMF patients compared to healthy controls. To the best of our knowledge, this is the first study to evaluate both ChT activity and concentrations in FMF patients.
MATERIALS AND METHODS
Patients and controls
The study groups were comprised of 80 FMF patients (37 males and 43 females; 18–68 years old [mean age: 34.86 ± 9.5]) and 80 controls (38 males and 42 females; 23–50 years old [mean age: 35.43 ± 6.44]). FMF diagnoses were made according to the Tel-Hashomer criteria (15). Twenty patients were in an acute attack period of FMF. The diagnosis of FMF attacks was confirmed by the presence of fever, clinical findings of serositis/arthritis, skin rash, and elevated C-reactive protein (CRP > 5 mg/L) concentrations. Seventy-two patients had been receiving stable doses of colchicine (1.5 mg/day), two patients had been receiving stable doses of both Anakinra (100 mg/day) and colchicine (2 mg/day), and two patients had been receiving stable doses of both colchicine and a nonsteroidal anti-inflammatory drug. We obtained information such as age, gender, MEFV mutation types, and the concentrations of some analytes of the study population from the records of the Ankara Numune Education and Training Hospital’s laboratory information system. Patients with impaired renal and thyroid function; diabetes mellitus; rheumatic disease; gut, musculoskeletal, and skin diseases; liver disease; malignancy; and pregnancy were excluded from the study. For the healthy controls, the exclusion criteria included a clinical suspicion of infections (body temperature out of the range of 36°C–38°C, heart rate > 90 rate/minute, respiratory rate > 20/minute, and white blood count > 12,000/mm3 or < 4,000/mm3); the presence of liver disease, kidney disease, rheumatic disease, or malignancy; pregnancy, and smoking. Blood samples were sent by physicians from Ankara Numune Education and Training Hospital, Department of Rheumatology.
Samples
Overnight fasting venous blood samples were collected into red top tubes (Becton Dickenson, UK) after a 12-hour fast. The serum samples were allowed to clot before centrifugation. After centrifugation at 4°C for 15 minutes at 3,500 rpm, serum was aliquoted and immediately frozen at −80°C (Sanyo, Japan).
Determination of ChT concentrations
ChT concentrations were determined by using commercially available ELISA (Sunred, Shanghai, China). The intra-assay and inter-assay confidence interval were < 10% and < 12%, respectively.
Determination of ChT activity
ChT enzyme activity was measured based on the method described by Kurt et al. (12) Briefly, 25 mL of serum was incubated with 100 mL of 22 mmol/L 4-methylumbelliferyl-b-D-N,N,N-triacetylchitotriose in McIlvain’s phosphate-citrate buffer, pH: 5.2, for 1 hour at 37°C. The reaction was terminated by the addition of 120 mL 0.5 mol/L Na2CO3-NaHCO3 buffer, pH: 10.7, and the fluorescence of 4-methylumbelliferone was measured using a Microfluor 2 fluorimeter (Bio-Tek Instruments, Neufahrn, Germany; excitation: 355 nm, emission: 460 nm). Serum ChT activities were expressed as nanomoles of the substrate hydrolyzed per milliliter per hour (nmol/mL/hr).
Statistical analysis
Data normality was assessed by the Shapiro-Wilk test. Two-sided independent samples t tests and Mann-Whitney U tests were used to compare the differences in the continuous and nonparametric variables, respectively. A χ2 analysis was used to compare the differences in the categorical variables, and the Pearson method was used to assess the correlation between C-reactive protein (CRP) and the activity and concentrations of chitotriosidase in the participants. Analyses were performed using IBM SPSS software (release 22.0, IBM, SPSS Inc., Chicago, IL, USA). P < 0.05 was considered as statistically significant.
RESULTS
The patients had a median duration of illness of 72 (2–360) months. The baseline characteristics of the study population are given in Table 1. The genotype and frequency of the detected mutations in the patients are provided in Table 2. Median ChT activity was 10.00 (6.00–15.00) nmol/mL/hr and 14.00 (6.25–20.75) nmol/mL/hr in the patients and controls, respectively. A statistically significant difference was found in the ChT activity between the controls and the patients (P = 0.027). The median ChT concentrations were 65.40 (46.20–84.92) pg/mL and 125.00 (75.72–143.95) pg/mL in the patients and controls, respectively. There was also a statistically significant difference between the controls and patients in terms of ChT concentrations (P < 0.001). The results are expressed as median percentiles (25th–75th). ChT activity, ChT levels and CRP concentrations in controls and patients have been given with boxplot in Fig. 1A, 1B and 1C, respectively. The mean C-reactive protein (CRP) was 2.58 ± 1.83 mg/dL and 34.20 ± 4.5 mg/dL in patients with an acute attack and an attack-free period, respectively. A statistically significant difference was observed in patients with an acute FMF attack compared to those in an attack-free period in terms of C-reactive protein (CRP) (P < 0.001). However, we did not find any significant difference in terms of the activity (P = 0.136) and concentrations (P = 0.331) of ChT between patients with an acute attack and an attack-free period. We also did not find any statistically significant correlation between ChT activity (P = 0.978, r = 0.003) or concentrations (P = 0.446, r = −0.87) and C-reactive protein concentrations in the patients.
Table 1
Baseline characteristics of study population
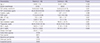
Table 2
Genotype and frequency of detected mutations in patients
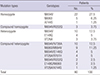
Fig. 1
Box plots for patients and controls. (A) Chitotriosidase activity. (B) Chitotriosidase levels. (C) CRP levels. The image of each group shows the box with median (horizontal line within the box); the interquartile range (IQR), corresponding to the 25th–75th percentiles (lower and upper limit of the box); nearest observations within 1.5 IQRs (the whiskers) and outliers (circles within 3 IQR).

DISCUSSION
Human ChT is a chitin fragmenting enzyme. Although the physiological functions of this enzyme are still unclear, there is evidence that ChT plays a role in the innate immune system (161718). Different studies have demonstrated changes in ChT activity and concentrations in multiple diseases (10111213). However, these changes have not been concurrently evaluated in patients with FMF. FMF is a chronic inflammatory and autosomal recessive disorder. Turkey is one of the countries that has the highest number of patients with FMF. Proteins encoded by Mediterranean fever (MEFV) called pyrin and marenostrin are secreted by neutrophils and macrophages. These proteins regulate the secretion of proteins in neutrophils and macrophages. Point mutations (single substitutions) in the MEFV gene have an important role in FMF pathogenesis. However, the diagnosis of FMF has been made principally according to clinical findings, and has been frequently applied to the MEVF mutation analysis in the case of patients in whom FMF is suspected (192021).
Taylan et al. (22) demonstrated increased concentrations of ChT in patients with FMF. Contrary to this study, we found lower ChT activity and concentrations in patients with FMF. To date, it has been thought that the main, and even the only, source of serum ChT is activated macrophage (12232425). However, it has been demonstrated that polymorphonuclear neutrophils are also a source of ChT (26). Colchicine inhibits the chemotaxis of neutrophils and the release of arachidonate and 5-lipoxygenase in macrophages (27). In our study, 76 patients were receiving colchicine. We thought that the reason for the reduced ChT concentrations and activity in patients with FMF was colchicine use. Colchicine might reduce the expression and activity of ChT by preventing neutrophil leucocytes chemotaxis and macrophage activity.
Familial Mediterranean fever is characterized by periodic attacks that last 1–3 days. The major inflammatory process in acute FMF attacks is the activation of neutrophils in serosal and synovial surfaces. It has been determined that CRP is the only acute phase protein raised during the acute attacks of patients with FMF (28). In our study, we found higher CRP concentrations in patients with an acute FMF attack than in those in an attack-free period. However, we did not find any statistically significant differences in the ChT activity and concentrations in patients with an acute FMF attack compared to those in an attack-free period. Additionally, we did not find any correlation between CRP and the activity and concentration of ChT. Our results are inconsistent with the results of Taylan et al. (22). The discrepancy between results might rely on the great differences in the study population number, the selection criteria for the patients, and differences in the received doses of colchicine. We believe that both ChT activity and concentrations cannot be used to determine and evaluate the acute attack period of FMF.
One of the limitations of the study was that the study population was made up of the same ethnic group, which cannot be generalized to other ethnic groups. Also, we did not adjust our data for body mass index. Another limitation was the lack of data about the patients’ ChT polymorphism.
In conclusion, the findings of the present study demonstrate that FMF patients have decreased ChT concentrations and activity compared to healthy controls. Additionally, we did not find any statistically significant correlation between enzyme activity and concentrations and disease activity. Our study is the first report that shows decreasing ChT concentrations and activity in FMF patients. According to our findings, serum ChT enzyme activity and concentrations may not be considered as a biomarker to evaluate disease activity and the prognosis of disease. However, more studies are needed to evaluate the changes in enzyme activity and the role of ChT in patients compared to colchicine negative patients.
 XML Download
XML Download