

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Carbon monoxide (CO) poisoning is the leading causes of childhood unintentional poisonings, and is a global public health problem (123). Carbon monoxide is an insidious poison that has no color, odor, or taste. The mechanism of CO toxicity predominantly relates to tissue hypoxia (123). Children are a high-risk group because they are less likely to be able to take preventive action and they have higher oxygen requirements because of their higher metabolic rates (2456).
Sources of CO that cause poisoning are fires with other toxic gases, incomplete combustion of organic fuels in poorly ventilated places, mines, and exhaust gas from cars in closed places like garages (12). In Turkey, the source of carbon monoxide was the inhalation of fumes from coal ovens and gas heaters in bathrooms (45). The heating systems used in houses in Turkey are stoves (natural gas stove included) (57.1%), central heating (37%), air conditioners, electric heaters and other systems (5.9%) (7). The gases used for water heaters are liquefied petroleum gas or natural gas. A defective device or defective installation can lead to leakage or partial combustion of gases during operation of the heater. When ventilation is poor and oxygen is inadequate, CO accumulates in the environment.
Early symptoms of CO poisoning are usually nonspecific, and nearly all organ systems can be effected (2). The most common symptoms on admission are vomiting and altered mental status; the most common sign is impaired mental state (268).
The purpose of our study was to determine the environmental conditions and principle causes of acute CO poisoning in children who were admitted to a pediatric clinic in Ankara, Turkey and to examine the status of acute CO poisoning under regional conditions, as a basis for preventive policies. Another purpose was to determine if the instructive assistance given to the families after the poisoning, in order to prevent recurrent poisoning, was effective.
MATERIALS AND METHODS
Subjected population
Ankara is the capital, and the second socioeconomically most developed among the provinces of Turkey. Ministry of Health, Ankara Training and Research Hospital is located in the central settlement, but in a poor socioeconomic area of Ankara. The study population consisted of children from this area. Informed consent was obtained from all cases or their parents.
This study is a descriptive one which was conducted at the Pediatric Emergency Service during one year period with the diagnosis of acute CO poisoning, and the data was prospectively collected with a standardized form. Annual admission to our Pediatric Emergency Department during the study period was 82,546. Of these, 955 were childhood poisoning cases. Carbon monoxide poisoning consisted 31.6% (n=302) among other causes of poisonings in children. Of these patients, 80 were appropriate for the study, which completed questionnaire and visited to hospital for control examination one month later.
Collection of data
The information was collected at the data form, about sociodemographic features of the children with acute CO poisoning. These were complaints and symptoms at the admission to hospital, the place and source of poisoning, the duration of the CO exposure, blood COHb levels upon admission and discharge. Precautions taken to avoid poisoning before the event were also asked. These were if the chimney was annually cleaned up and isolated, if hot-water heater was routinely controlled and if stove's ventilation holes were closed down during sleep or not. The other collected information were number of people poisoned in the same family, income of the family (9); education status of parents (primary, secondary, high school or university graduate), type of house the family has been living (apartment block or shelter).
The diagnosis was confirmed by taking blood samples for measuring COHb levels. Blood COHb levels higher than 2% levels were registered as abnormal. Nova Biomedical Walthom, MA 02454 USA CO Oximeter was used to analyze blood gases. A child with symptoms but normal COHb level was also accepted as acute CO poisoning if there is a history of CO poisoning at the child or family members.
All children's physical examinations were done; blood gases were obtained, and high flow oxygen was administered with a tight fitting mask. Treatment was continued until symptoms completely resolved and blood COHb levels fell below 2%. The children were divided into three groups according to their symptoms, at admission: Group I; if they only suffer from nausea and vomiting, Group II; if they have headache and vertigo, and Group III; if they have change in consciousness with or without other symptoms.
In our region hyperbaric oxygen treatment is inevitable. Transportation of severely poisoned patients to hyperbaric oxygen centre was difficult during the study period.
The parents were elucidated to take the precautions to cleaning-up and isolating the chimney, control of hot-water heater and keeping the stove's ventilation holes open during sleeping One month after discharge, children were re-evaluated. Physical examination was done and blood pressure measurements were obtained. Also, decrease in school performance, change in temperament, precautions taken (the same questions stated to avoid poisoning in the third item), and recurrence of symptoms (existence of complaints compatible with CO poisoning) after the event were recorded.
RESULTS
Eighty children with acute CO poisoning were compatible with the study to be included. Of these, 36 (45%) were girls. The mean age was 8.3±4.4 yr (range: one months-16 yr).
Admission of the patients demonstrated seasonal variation. Most of the patients were hospitalized during winter (66.3%, n=53). Remainder of the patients were hospitalized during autumn (18.7%, n=15) and spring (15%, n=12). In summer, no admission happened.
Among the children with CO poisoning, 53.7% (n=43) of them admitted to the hospital between 09.00 pm to 09:00 am, during night. The children were exposed for a 1-10 hr period to CO gas, at home. The reason for delay was that families did not consider that their complaints were due to CO poisoning. In the children of the families with CO poisoning, three or more people were poisoned in the same family in 85.1% (n=68).
The education levels of the parents were low; 86.2% (n=69) of the mothers and 52.6% (n=42) of fathers had no education or were educated from primary school. All of the families had low income and status of the house was apartment block in 51.2% (n=41) of them.
The exposure of the gas occurred in the household setting. Sources of CO were coal or wood stoves in 71.2% (n=57) and gas leakage from hot-water heaters in 28.8% (n=23). Most of the families had not taken precautions before poisoning (68.8%, n=55). These families used stoves and hot water heaters improperly and unsafely. Stove's ventilation hole was closed down during sleep, in order to reduce fuel combustion at night. Because family members share the same room, more than one person was poisoned in a family.
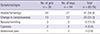
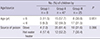
The most common complaints of the children admitting to hospital with acute CO poisoning were headache and vertigo (58.8%, n=47) (Table 1). No association was found with age and source of poisoning (P=0.951 and P=0.366, respectively,) (Table 2).
Median COHb levels at admission and discharge were 19.5% and 1.1% (interquartile ranges: 11 and 0.3) (Wilcoxon P<0.001) (Table 3). An association was not determined between COHb levels at admission with age, source of poisoning, complaints, mother's and father's education levels and family income (P=0.491; P=0.900; P=0.110; P=0.154; P=0.056 and P=0.185, respectively).
One child received hyperbaric oxygen treatment, and the others recovered by administering high flow 100% oxygen. Forty-seven (58.8%) of the children were kept under observation for 24 hr, while 33 (41.2%) were observed for 12 hr duration in hospitals.
All of the children recovered. Unfortunately, however, one child's parents and a father of two siblings in another family, who were sleeping nearby the stove, had died because of CO poisoning.
Altered consciousness indicated in 24 children were transient, and they rapidly (not exceeding for an hour) and completely recovered with a high flow 100% oxygen via a tight fitting mask. One unconscious and convulsive child, whose father had died, recovered also after performing hyperbaric oxygen treatment.
Altered consciousness indicated in 24 children were transient, and they rapidly (not exceeding for an hour) and completely recovered with a high flow 100% oxygen via a tight fitting mask. One unconscious and convulsive child, whose father had died, recovered also after performing hyperbaric oxygen treatment.
One month after discharge, physical examinations of the cases including neurological examination and blood pressures confirmed that their physical conditions were normal. However, seven (8.8%) of them mentioned that their success in academic examination marks had declined, and nine (11.3%) became nervous due to fear of reattack of poisoning.
When compared before poisoning most of the families took precautions after the event (n=69, 86.3%). None of the cases was readmitted to hospitals because of recurrent symptoms or poisoning.
DISCUSSION
Acute CO poisoning was the most frequent cause among all childhood poisonings in our unit. The present study defined the characteristics of children with acute CO poisoning. All acute childhood CO poisonings occurred at home, from coal stoves or from gas hot water heaters. The numbers of people poisoned in the same family were three or more in 85.1% of cases. The reasons for these results included the followings. 1) Most of the families (68.8%) had not taken precautions for stove and hot water usage. 2) Coal stoves and gas hot water heaters were used improperly and unsafely. For example, at night, for reducing coal usage families closed down stove taps. This caused incomplete combustion of coal and CO production. 3) Family members shared the same room. Consequently, more than one person was poisoned. In children with acute CO poisoning, those having well educated parents had higher COHb levels than less educated parents. The reason of this result was time lag between poisoning and admission to hospitals was shorter in well educated parents than less educated ones.
The studies conducted in Turkey were also compatible with our study that the source of CO was the inhalation of fumes from coal ovens and gas heaters in bathrooms (45). Aşırdizer et al. (4) reviewed CO poisoning was the leading cause of all home accidents, accounting for 34% of the cases. Sources were coal ovens in 51% and gas water heaters in 36% of the cases. Another study reported that in their study group CO poisoning was due to improper combustion of recently marketed steam coal in inadequately ventilated bucket stoves (10).
In our study, children with acute CO poisoning most frequently complained from headache, vertigo and change in consciousness. Our findings were compatible with those of other studies, which have evaluated symptoms and signs in acute CO poisoning in childhood (8101112). Emri et al. (10) reported that during the years 1986 to 1990, an increase in number of cases of acute CO poisoning was observed in the Emergency Department Hacettepe University Hospital in Ankara, Turkey. Among these patients, nausea or vomiting and headaches were the most common complaints (occurring in 100% and 85%). At least transient impairment of alertness was observed in 29% of cases. In another report that authors presented 74 children, aged from 1 to 17.8 yr, the most frequent symptoms were altered mental state (52.7%), dizziness (37.8%), headache (32.4%), nausea (31.1%), vomiting (25.7%), and syncope (23%) (13).
Although none of the children died in our study, CO was found to be the most frequent cause of death among fatal poisonings (2). Other studies reported their mortality rates in acute childhood CO poisoning as 1.3%, 3.7%, and 23.1% (81214). Chou et al. (15) investigated characteristics and outcomes of children with CO poisoning with and without smoke exposure. Children having smoke inhalation due to closed-space fire had a significantly higher risk of dying than those children with CO poisoning alone (22.6% vs. 0%). A combination of smoke inhalation, low temperature, high COHb level, respiratory arrest, and cardiac arrest was highly associated with death. The causes of lack of death in our study may be that there were no fire burns and COHb levels were not very high in our study group (median 19.5%, maximum 45.7%).
Poverty is their main barrier to obtain and use cleaner fuels (16). The types of fuels used increase in cleanliness, convenience, efficiency, and cost, as people's socio-economic conditions improve (17). In our study group, families had low income and used coal and wood stoves to heat their homes. This is an evidence demonstrating that acute childhood CO poisoning in Ankara is associated with poor socio-economic characteristics.
In our study control physical examinations of the children, implemented one month later, revealed that children recovered without neurological sequel, but seven of them had temperament change and nine had lower school performances after the event. The onset of psychic troubles in adult cases of CO poisoning may lag 3 to 240 days, in about 10%-30%, but they were associated with neurological problems (18). Delayed neurological syndromes are uncommon in children treated with normobaric oxygen (12). However, the follow-up in our study is short, and a call of children and reassessment might be necessary, because we cannot be sure that more children may develop problems. We think that these cases should be followed for a long period.
In this study, one important aspect of information about CO poisoning to emphasize might be identifying the sources of CO. Childhood acute CO poisoning occurs as a home accident because of not taking precautions regarding stoves and hot-water heaters used at homes. In view of the fact that poisonings occur particularly during sleep, using CO detectors, which sound on alarm in the presence of elevated CO, should be used (6). Reduction of CO production at home must be a public health measure in reducing the incidence of CO poisoning of children.
Physicians working in emergency medicine should consider inviting other household members for evaluation and guidance, who are sharing same environment with poisoned patients. Furthermore, the physicians should educate the people at high risk of poisoning about the fact that the poisoning is preventable. The poisoned children should not return to the same environment without taking precautions or prevention measures.
In conclusion, acute CO poisoning in Ankara arises mainly from stoves or hot water heaters used at homes of low economic status. Instructive assistance given to the families after the poisoning was effective to prevent recurrent poisoning. This study emphasizes that all people who have risks of CO poisoning should be educated to prevent poisoning. In countries that uncontrolled heating systems like coal stoves and hot water heaters are being used, there is a need to take environmental and policy controls to curb this public health problem.

 XML Download
XML Download