

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The anomalous origin of the coronary artery arising from the opposite sinus (ACAOS) is a rare coronary artery anomaly which potentially may cause coronary ischemia when an aortic intramural course of the vessel is present.1) When ischemia caused by a phasic compression of the intramural decourse is confirmed, stenting or surgical un-roofing are generally proposed. A 47-year-old hypertensive man with acute coronary syndrome and ST changes in the inferior-lateral wall underwent emergent coronary angiography. The left circumflex presented a sub-occlusive lesion which was treated with a III-generation drug-eluting stent (DES). The right coronary artery (RCA) originated from the opposite sinus with a decourse which appeared closed to the left stem, anterior to the aorta with no impingement (Figure 1). A computed tomography (CT) angiographic scan failed to clearly demonstrate an intramural course (Figure 2). Because of a residual thoracic discomfort and abnormal electrocardiogram, a new transthoracic echocardiogram was performed in order to ruling out eventual procedure-related complications. An intramural decourse of the proximal portion RCA was clearly visible in the parasternal short axis view (Figure 3). A new coronary angiography with intravascular ultrasound examination of the intramural course demonstrated a phasic compression of the intramural decourse not apparent on the previous coronary angiography (Figure 4). A III generation DES has been successfully implanted (Figure 5) with ST changes and symptomatology resolution (Figure 6). Emotional or environmental stress and hypertensive status may have a potential role in phasic lumen reduction of the proximal vessel lumen in case of ACAOS when an intramural de-course is present. A careful use of both non-invasive and ancillary invasive imaging tools are fundamental for the proper management of such rare anatomo-pathological entity.2)
Gianluca Rigatelli, MD, PhD
Figures and Tables
Figure 1
Subselective right coronary angiography demonstrating an anomalous origin (asterisk) of the RCA from the left coronary sinus of valsalva on anteroposterior view.
RCA = right coronary artery.
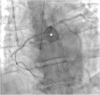
Figure 2
A CT angiographic scan demonstrate an anomalous origin (asterisk) of RCA (A) without a clear demonstration of the intramural course of the vessel (B).
CT = computed tomography; RCA = right coronary artery.

Figure 3
Transthoracic echocardiogram in parasternal short axis view shows an intramural decourse (asterisk) of the of the proximal portion of RCA (A, B: the red conturns highlight the borders of the aortic annulus and the intramural wall of the vessel).
AW = atrioventricular valve; AV = aortic valve; CAW = common atrioventricular valve; RCA = right coronary artery.

Figure 4
Urgent coronary angiography in right anterior oblique projection (A) and IVUS examination: a compression of the intramural course is apparent being the proximal part of the vessel squeezed into an elliptical shape with clearly reduced luminal area and no real plaque burden (B). The rest of the vessel is free from significant atherosclerosis (C).
IVUS = intravascular ultrasound.



References
1. Angelini P, Uribe C, Monge J, Tobis JM, Elayda MA, Willerson JT. Origin of the right coronary artery from the opposite sinus of Valsalva in adults: characterization by intravascular ultrasonography at baseline and after stent angioplasty. Catheter Cardiovasc Interv. 2015; 86:199–208.

2. Rigatelli G, Cardaioli P. Endovascular therapy for congenital coronary artery anomalies in adults. J Cardiovasc Med (Hagerstown). 2008; 9:113–121.
 XML Download
XML Download