

 PDF
PDF ePub
ePub Citation
Citation Print
Print



A 80-year-old female patient presented with dyspnea intractable to medical therapy. She received surgical mitral valve replacement with Hancock II (Medtronic, Minneapolis, MN, USA) (Figure 1) 27 mm bioprosthetic valve 11 years ago due to severe rheumatic mitral stenosis. Other comorbidities included atrial fibrillation, stroke, and restrictive lung disease. The echocardiography showed a prolapse of bioprosthetic mitral valve posterior leaflet with severe eccentric mitral regurgitation (MR) accompanied by severe resting pulmonary hypertension. The multi-detector computed tomography (MDCT) showed the degenerative change of mitral bioprosthetic valve with posterior leaflet prolapse.
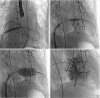
Multi-disciplinary Heart team determined to undergo transcatheter mitral valve-in-valve replacement due to high surgical risk. Based on the MDCT analysis showing 460 mm2 of bioprosthetic valve area, we selected the SAPIEN 3 (Edwards Lifesciences, Irvine, CA, USA) 26 mm transcatheter heart valve with the nominal size (519 mm2), which achieved 13% area over-sizing. After the transseptal puncture, the atrial septum was dilated with a 10×40 mm balloon catheter (Figure 2A). A small-curve Safari wire (Boston Scientific, Marlborough, MA, USA) was placed in the left ventricle. The SAPIEN 3 26 mm transcatheter heart valve was delivered into the bioprosthetic mitral valve (Figure 2B) and deployed under rapid ventricular pacing (Figure 2C). Left ventriculogram showed trivial MR without acute complications (Figure 2D). Fluoroscopy showed that about 20% of the prosthesis was placed on the atrial side of the sewing ring (Figure 3). Patient's symptoms subsequently improved and echocardiography showed trivial MR with mild resting pulmonary hypertension (Supplementary Videos 1, 2, 3, 4).
Bioprosthetic mitral valve dysfunction requiring re-operation was about 40% after 15 years following surgical mitral valve replacement.1) Reoperation is considered a high-risk procedure, particularly in elderly patients with multiple comorbidities.2) Transseptal transcatheter mitral valve-in-valve replacement is a promising treatment strategy for those patients with excellent procedural success and acceptable long-term outcomes.3)4)



 XML Download
XML Download