

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia, occurring in 1–2% of the general population.1) AF is associated with a 5-fold increase in the stroke risk, and 1 in 5 cases of stroke is attributed to this arrhythmia.2) Multiple clinical trials have demonstrated the superior therapeutic effect of warfarin compared to that of placebo in the prevention of thromboembolic events among patients with non-valvular AF.3) However, AF patients with comorbidities have a concomitant risk of fatal bleeding, and therefore, clinicians might be reluctant to use vitamin K antagonists (VKAs) despite a high stroke risk.4)5) AF is common in patients with life-threatening cancer and those undergoing active cancer treatments.6) Several studies have suggested that the association between cancer and AF is not limited to the postoperative period.7)8) Despite the excellent effects of VKAs in the prevention of thromboembolisms, VKAs might result in an elevated bleeding risk in patients with cancer and a history of non-valvular AF because of poor international normalized ratio (INR) control.5)9) Moreover, it is difficult to achieve therapeutic drug levels in cancer patients owing to the risk of drug interactions, malnutrition, and vomiting in these patients.5)
Non-vitamin K antagonist oral anticoagulants (NOACs) are a new additional option for stroke prevention in AF patients, which are considered at least as effective and safe as VKAs.10) NOACs have a wide therapeutic window, low inter- and intra-individual variability, and no clear interactions with food, and there is no need for frequent laboratory monitoring and dose adjustments.10)11)12) However, there are little controlled data on the use of NOACs in AF patients with cancer, and active cancer was usually an exclusion criterion in randomized NOAC trials.13) We hypothesized that NOAC administration would result in favorable clinical outcomes in AF patients with newly diagnosed cancer. The aim of this study was to evaluate the safety and efficacy of NOACs in AF patients with cancer by comparing the findings with those for patients receiving NOACs and warfarin. Additionally, we evaluated the clinical outcomes according to time of cancer diagnosis, and dosage and types of NOACs in this study.
METHODS
Patients
The study protocol was approved by the Institutional Review Board of Severance Cardiovascular Hospital, Seoul, Korea (4-2016-0105) and complied with the Declaration of Helsinki. No informed consent was required for study populations. Between November 2005 and June 2015, we identified 2,568 consecutive patients with non-valvular AF who were newly diagnosed with cancer in Yonsei University Severance Hospital. The study subjects were followed up until they developed an event or until the last follow-up date whichever came first. Patients who were not prescribed any oral anticoagulants (OACs; n=867), those who underwent radiofrequency catheter ablation or cardioversion (n=5), and those who had insufficient clinical data (n=45) were excluded. Finally, we enrolled 1,651 patients in this study. The patients were divided into the following 2 groups according to treatment: NOAC group (n=572) and warfarin group (n=1,079; Figure 1).
 | Figure 1Flowchart of patients participating in this study.
AF = atrial fibrillation; NOAC = non-vitamin K antagonist oral anticoagulant; RFCA = radiofrequency catheter ablation.
|
AF was documented using 12-lead electrocardiography or 24-hour Holter recordings. The patients' medical records were reviewed. The patient databases were searched to identify any known or putative risk factors for ischemic stroke.14) Heart failure was considered when hospitalized patients had appropriate symptoms (shortness of breath, fatigue, fluid retention, or any combination of these symptoms) and clinical signs of fluid retention (pulmonary or peripheral) with explainable abnormalities of the cardiac structure and function.15) The congestive heart failure, hypertension, age ≥75 years (doubled), diabetes mellitus, previous stroke or transient ischemic attack (doubled), vascular disease, age 65–74 years, and gender category (female) (CHA2DS2-VASc) and hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR, elderly (age >65 years), drugs/alcohol concomitantly (HAS-BLED) scores were evaluated. Bleeding history was defined as follows: Intracranial, hospitalization, hemoglobin decrease >2 g/L, and/or transfusion. Drugs/alcohol concomitantly was defined as concurrent use of antiplatelet agents (include aspirin, clopidogrel, cilostazol, prasugrel, or ticagrelor), nonsteroidal anti-inflammatory drugs; one point for drugs plus one point for alcohol excess, maximum 2 points.16) Renal insufficiency was considered when serum creatinine was >2 mg/dL, and abnormal liver function was considered when cirrhosis, bilirubin >2 times the upper limit of normal (ULN), or aspartate aminotransferase/alanine transaminase/alkaline phosphatase >3 times the ULN was noted. Dialysis patients and cirrhosis patients were excluded owing to the indication of NOAC. Mean INR values and time in therapeutic range (TTR) of INR 2.0–3.0 were calculated using the linear interpolation methods proposed by Rosendaal et al.17) The percentage of time during which a patient had an INR within 2.0 to 3.0 was taken as the TTR. According to the center's protocol, INR was measured every 8–12 weeks and more frequently when it was not within the therapeutic range. The full doses of NOAC were defined as 150 mg twice for dabigatran, 5 mg twice for apixaban, and 20 mg once for rivaroxaban. The indication of the reduced dose followed the current guideline (dabigatran 110 mg twice a day if patients are aged ≥80 or have an estimated glomerular filtration rate [eGFR] of 30–50 mL/min; rivaroxaban 15 mg once a day if eGFR is 15–49 mL/min; apixaban 2.5 mg twice a day if 2 of the 3 following criteria are present: age ≥80 or serum creatinine ≥1.5 mg/dL or body weight ≤60 kg).10) eGFR was calculated by Cockroft-gault equation.18) Doses not listed above (apixaban 2.5 mg once or rivaroxaban 10 mg once, etc.) were excluded as off-label dose.
Follow-up
The follow-up period was defined as the period from the date of cancer diagnosis to the date of an event or the date of the last visit if an event did not occur. We also set the study endpoint as the point when the first anticoagulation strategy was stopped or changed, according to on-treatment analysis. We evaluated ischemic stroke/systemic embolism (SE), major bleeding, and all-cause death during the follow-up. Ischemic stroke was defined as a neurological deficit with a sudden onset that persisted for >24 hours corresponding to a vascular territory in the absence of primary hemorrhage and was not explained by other causes, including trauma, infection, and vasculitis.19) Major bleeding was defined according to the definition by the International Society on Thrombosis and Haemostasis.20) When a patient experienced both ischemic stroke/SE and major bleeding during the follow-up period, each event was counted separately. However, when analyzing the Kaplan-Meier cumulative incidence rate, we considered the first event only.
Statistical analysis
Normally distributed continuous variables are presented as mean±standard deviation, and compared using Student's t-test for parametric data and the Mann-Whitney U test for nonparametric data. Categorical variables are presented as number (percentage), and compared using the χ2 test or Fisher's exact test.
To reduce the effect of selection bias and potential confounding cohort study, estimated propensity scores (PSs) were used to match the patients who received NOACs to patients who received warfarin. PSs were estimated using a non-parsimonious multiple logistic regression model for the NOAC and warfarin groups. The following variables were considered: age, sex, hypertension, diabetes mellitus, heart failure, chronic kidney disease, history of stroke or transient ischemic attack, history of myocardial infarction or peripheral vascular disease, history of hemorrhage, concomitant antiplatelet, type of cancer, rate of metastatic cancer, and follow-up duration. Cases were then matched, without replacement, with controls 1:1 based on the closest possible value of the PS (nearest neighbor matching). We evaluated the balance between treatment populations according to standardized differences of all baseline covariates, using a threshold of 0.1 to indicate imbalance.21) A matching caliper of 0.2 standard deviations of the logit of the estimated PS was enforced to ensure that matches of poor fit were excluded. The matching procedure was performed using R packages (R Foundation, Vienna, Austria). Based on PS matching, 388 matched pairs were included in the NOAC and warfarin groups. Kaplan-Meier curves for cumulative incidence rate were plotted for the NOAC and warfarin groups and were compared using the log-rank test. All statistical analyses were performed using R version 3.1.1 (http://www.r-project.org/). A p value <0.05 was considered statistically significant.
RESULTS
Patient characteristics
The overall clinical characteristics of the patients are presented in Table 1. The patient age was greater in the NOAC group than in the warfarin group (74.2±8.3 vs. 67.5±8.0 years, p<0.001). The prevalence of hypertension, diabetes, congestive heart failure, stroke/transient ischemic attacks, and major bleeding was higher in the NOAC group than in the warfarin group (all p<0.001). Additionally, the CHA2DS2-VASc and HAS-BLED scores were higher in the NOAC group than in the warfarin group (CHA2DS2-VASc: 3.8±1.7 vs. 3.4±1.4, p<0.001; HAS-BLED: 2.0±1.0 vs. 1.8±1.2, p<0.001). Stomach cancer was the most common malignancy, followed by colorectal cancer (Supplementary Table 1). There was no patient who was prescribed concomitant dual antiplatelet agents with OACs. After PS matching, the baseline characteristics were well matched between the NOAC and warfarin groups. The median follow-up duration was comparable between the NOAC and warfarin groups (1.8 vs. 1.7 years, p=0.593). Baseline characteristics of patient without OAC was shown in Supplementary Table 2.
Table 1
Baseline characteristics of the PS-matched patients
Data are presented as mean±standard deviation or number (percentage).
CHA2DS2-VASc = congestive heart failure, hypertension, age ≥75 years (doubled), diabetes mellitus, previous stroke or transient ischemic attack (doubled), vascular disease, age 65–74 years, and gender category (female); HAS-BLED = hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile INR, elderly (age >65 years), drugs/alcohol concomitantly; MI = myocardial infarction; NOAC = non-vitamin K antagonist oral anticoagulant; PAD = peripheral artery disease; PS = propensity score; SMD = standardized mean difference.
*All p values were not statistically significant.
![]()
Comparison between the NOAC and warfarin groups
During the median follow-up period of 1.8 years, the cumulative incidence rates of ischemic stroke/SE, major bleeding, and all-cause death were lower in the NOAC group than in the PS-matched warfarin group (Figure 2). The rates of ischemic stroke/SE, major bleeding, and all-cause death in the matched population are presented in Table 2. The rates of ischemic stroke/SE (1.3% vs. 5.9%/year, p<0.001), major bleeding (1.2% vs. 5.1%/year, p<0.001), and all-cause death (6.1% vs. 13.3%/year, p<0.001) were lower in the NOAC group than in the PS-matched warfarin group. With regard to ischemic stroke, the incidence rate was 1.3%/year in the NOAC group and 5.5%/year in the warfarin group (p<0.001). With regard to major bleeding, the gastrointestinal bleeding rate was 1.0%/year in the NOAC group and 3.5%/year in the warfarin group (p=0.001). Additionally, the intracranial bleeding rate was 0.2%/year in the NOAC group and 1.1%/year in the warfarin group (p=0.02).
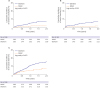 | Figure 2Cumulative incidence of ischemic stroke/SE, major bleeding, and all-cause death in the PS matched NOAC and warfarin groups.
NOAC = non-vitamin K antagonist oral anticoagulant; PS = propensity score; SE = systemic embolism.
|
Table 2
Clinical outcomes according to anticoagulation strategies (PS-matched populations)

Event rate was described as event per 100-patient years.
NA = not applicable; NOAC = non-vitamin K antagonist oral anticoagulant; PS = propensity score; SE = systemic embolism.
![]()
Time after cancer diagnosis and anticoagulation
The numbers of patients with ischemic stroke/SE, major bleeding, and all-cause death according to the duration after cancer diagnosis are presented in Figure 2. Within 1 year after cancer diagnosis, there were 7 ischemic stroke/SE events (1.9%/year) in the NOAC group and 26 events (7.9%/year) in the warfarin group (Figure 3; p<0.001). Between 1 and 2 years after cancer diagnosis, there was 1 stroke event (0.3%/year) in the NOAC group and 8 events (2.5%/year) in the warfarin group (p=0.01; Figure 3). There were similar trends in major bleeding (1.1 vs. 7.9%/year within 1 year; p<0.001 and 0.8 vs. 1.9%/year between 1 and 2 years; p=0.25) and all-cause death (7.2 vs. 17.2%/year within 1 year; p<0.001 and 3.2 vs. 7.0%/year between 1 and 2 years; p=0.03).

Clinical outcomes according to different anticoagulation strategies
Figure 4 presented clinical outcomes according to different anticoagulation strategies. A TTR ≥60% was achieved in 61 of 328 patients in the warfarin group (18.6%). The NOAC group showed significantly lower rates of ischemic stroke/SE, major bleeding, and all-cause death than the TTR <60% group (all p<0.01). However, compared with the TTR ≥60% group, the NOAC group showed similar ischemic stroke/SE, but significantly lower major bleeding rates (p=0.03; Supplementary Figure 1).
 | Figure 4Cumulative incidence rates of all clinical events according to anticoagulation strategy. (A) Ischemic stroke/SE, (B) major bleeding, (C) all-cause death.
NOAC = non-vitamin K antagonist oral anticoagulant; SE = systemic embolism; TTR = target therapeutic range.
*Warfarin and TTR <60% groups showed significantly higher rates of all clinical events than NOAC group, †TTR ≥60% group showed significantly higher rates of major bleeding than NOAC group.
|
In the NOAC group, dabigatran, apixaban, and rivaroxaban were prescribed in 140 (36.1%), 138 (35.6%), and 110 (28.3%) patients, respectively. Full NOAC dose was prescribed in 109 (28.1%) patients. Among 279 (71.9%) patients with reduced NOAC dose, 129 patients were prescribed reduced dose according to indication and 150 patients were underdosed. The rates of ischemic stroke/SE, major bleeding, and all-cause death were not significantly different between the full and reduced NOAC dose groups. Likewise, there were no significant differences according to the NOAC type (Table 2). In subgroup analysis according to cancer type and stage, p values for interaction were not significant (Supplementary Figure 2).
DISCUSSION
All clinical outcomes, including ischemic stroke/SE, major bleeding, and all-cause death, were better in the NOAC group than in the PS-matched warfarin group. Additionally, the rate of major bleeding was significantly lower in the NOAC group than in the optimal INR control (TTR ≥60%) group. Especially, within 1 year after cancer diagnosis, the incidences of all clinical outcomes were significantly lower in the NOAC group than in the warfarin group. Finally, there was no significant difference in the clinical outcomes according to NOAC dosage and type. These findings suggest that NOACs could be considered for anticoagulation in AF patients with newly diagnosed cancer.
Large studies have suggested that the occurrence of thromboembolisms is 4- to 8-fold higher in patients with active cancer than in those without cancer.22) However, warfarin is largely underused because of concerns regarding the need for systematic monitoring and the risk of bleeding complications.23) Previous studies have shown that it is difficult to obtain an optimal range of the INR in cancer patients owing to cancer treatment.5) It is difficult to maintain a stable INR in the setting of the concomitant use of chemotherapy agents. Furthermore, cancer itself and other invasive procedures may induce fatal bleeding.10)24) In our study, it is notable that 867 patients were not treated with oral anticoagulation and were therefore excluded from the study. The exact reason for not receiving anticoagulation was not known. Maybe a relatively high proportion of metastatic cancers is associated with short life expectancies and higher bleeding tendency, and therefore it is possible that anticoagulants were not prescribed. Other unspecified factors, such as patient preferences, might have been taken into account for not prescription of OACs. In concerns of major bleeding complication, warfarin was often underdosed and NOAC was prescribed at a reduced dose. In our study, NOACs showed significantly lower incidence rates of all clinical outcomes than warfarin, and lower major bleeding rate when compared with optimally controlled warfarin group. This suggests that the worse outcomes of warfarin are related to poor achievement of optimal TTR and that NOAC may be more useful in this situation.
Cancer patients were excluded in previous randomized clinical studies, and there were few cancer patients in phase 3 AF trials.13)25)26)27) Subgroup analysis suggested that the net benefit of NOACs appears to be better than that of warfarin in situations in which the quality of oral anticoagulation is poor.28) Our previous study found that 10% of warfarin-treated cancer patients achieved ≥60% of the TTR during follow-up. The composite endpoint was better in patients with TTR ≥60% than in those with TTR <60% and without oral anticoagulation therapy.5) In present study, the TTR ≥60% group showed lower rates of ischemic stroke/SE and all-cause death when compared to the rates in the TTR <60% group, whereas major bleeding events were not statistically significant according to TTR. Patients in the TTR <60% group were mostly prescribed underdosed warfarin, and this resulted in a lower incidence of major bleeding.
Interestingly, although 71.9% of patients in NOAC group received reduced doses of NOACs, clinical outcomes were not significantly different between the reduced dose and full dose groups. In terms of major bleeding, the frequency of a reduced dose was somewhat higher, although not statistically significant. This may be associated with a stronger bleeding tendency that could not be noted in the reduced dose group. In general, Asians have a smaller body size and body mass index than non-Asians who have been used as subjects in many previous large-scale randomized studies.13)26)27) In the J-ROCKET AF trial, it was found that 15 mg of rivaroxaban in Japanese patients was equivalent to 20 mg of rivaroxaban in Caucasians with regard to the pharmacokinetic profile.29) Furthermore, Chan et al.30) reported that low doses of rivaroxaban and dabigatran reduced the risk of ischemic stroke and bleeding in Taiwanese people when compared to the effect with warfarin. Our study also suggested that low doses of NOACs have superior efficacy when compared to that of warfarin, which may be used more safely in cancer patients.
Approximately 7 of 10 patients with all clinical events showed the events within 1 year after cancer diagnosis. In the early stage of cancer treatment, it is very difficult to maintain proper medication dose due to invasive anticancer treatment such as surgery or biopsy. Therefore, clinical outcomes are likely to occur during early cancer diagnosis. In the present study, NOACs showed lower incidences of all clinical outcomes within 1 year after cancer diagnosis than warfarin. NOACs are known to have a short onset time, short half-life, and low drug to drug interactions compared to warfarin, and this characteristic may be helpful in the early diagnosis of cancer in which anticoagulation is frequently interrupted.12) Therefore, NOACs could be considered in AF patients with newly diagnosed cancer, especially within 1 year after cancer diagnosis.
The present study has several limitations. First, this was a retrospective and non-randomized study, and therefore, it had all the limitations of such studies. To reduce the effect of selection bias and possible confounding in this retrospective cohort study, estimated PSs were used, and most of the baseline characteristics, including the follow-up duration, were well matched. The second limitation is difference in time of enrollment between study groups. Starting in 2015, the number of patients in NOAC group was greater than warfarin, and patients in the warfarin group were enrolled earlier than NOAC group. This difference was corrected by PS matching and limiting maximum follow-up duration, but this difference is a critical limitation of this study. The third limitation is a relatively small number of study populations. Because of this, the effectiveness of the reduced dose in cancer patients and the differences in the type of NOAC could not be clarified. Further large-scale and long-term follow-up studies would be needed to clarify these questions. Fourth, the heterogenicity of cancer might resulted in bias. However, the distribution of cancer was well matched in PS-matched population. Fifth, the chemotherapy drug, and the information of surgery were not investigated. Especially, types of chemotherapy drugs and their durations were heterogenous and we were not able to get all the data. Considering that anticoagulation during chemotherapy may affect bleeding risk, the lack of this data is an important limitation of this study. Large-scale studies with a better design will be needed because the risks of bleeding and thrombosis different according to type of cancer, anticancer medication, and stage.
In AF patients with newly diagnosed cancer, all clinical events were less common with NOACs than with warfarin. Major bleeding rate was lower in NOAC group than optimal INR controlled warfarin group. Finally, although warfarin did not improve the clinical outcomes because of poor INR control caused by cancer treatment during the first year after the cancer diagnosis, NOAC was effective within 1 year. However, there were quite limitations and further well-controlled large-scale studies would be needed to clarify our results.
 XML Download
XML Download