

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Arguably, transcatheter closure of secundum atrial septal defects (ASDs) has become the therapy of choice throughout the developed world. Indeed reports on closing superior sinus venosus ASDs, thought to be exclusively within the realm of surgery, are evolving.1) However before we become overly confident, it is worth reflecting on the efforts required to get us to this juncture. The first series of transcatheter ASD closures was reported by Terry King and Noel Mills over 4 decades ago,2) and it took another 25 years before transcatheter ASD closure became commonplace with Food and Drug Administration approval of the Amplatzer Septal Occluder. A similar lag-time existed following the initial report on transcatheter closure of the ductus arteriosus,3) and we are still no closer to a robust transcatheter solution to closure of perimembranous (VSD)'s following concerns regarding heart block on the initial clinical trial evaluating the Amplatzer membranous occluder over a decade ago.4) Therefore significant challenges remain. Recent attempts to identify erosion rates following transcatheter ASD closure have proved difficult due to sub-optimal data monitoring and collection,5) apart from regions where data collection is mandatory. Evaluation of alternative devices has been hampered by the need for multiple separate clinical trials in different countries, deterring industry to commit excessive non-returnable investment to achieve widespread device approval. Although stent design has evolved rapidly promoting opportunities for non-surgical palliation of small infants, none of these stents are specifically designed for the congenital heart population. Development of bespoke stents and devices providing “personalized therapy” suitable for the wide variation in anatomical substrates is achievable within the next 2 decades, however collective efforts are required to bring this to reality. Rather than re-evaluate data on past achievements, this review will focus on the efforts required to achieve these goals and also evaluate evolving therapies particularly in the context of transcatheter valve replacement, hybrid therapies and bioresorbable materials and tissue engineering.
FETAL INTERVENTIONS
It is generally accepted that variations in blood flow may influence vessel or chamber growth in the developing heart. With advances in fetal cardiac screening, over 50% of significant congenital heart lesions can be identified in the antenatal period.6) This provides the potential to alter blood flow and therefore arrest or reverse progressive subsequent chamber or vessel hypoplasia in selected conditions. Progress with fetal cardiac interventions has mirrored other advances in congenital cardiac interventions, with an initial lag-time following the disappointing results of the first report of fetal balloon aortic valvuloplasty in 1991.7) This may reflect the challenging nature of the intervention along with difficulty in identifying optimal candidates and timing, however the publication of a guideline document has provided some clarity.8) A single center cohort of 100 cases of fetal balloon aortic valvuloplasty demonstrated fetal demise in 11%, and biventricular circulation in 43% of the live born cohort.9) Although the majority of children achieving a biventricular circulation required further interventions, these are encouraging results, diverting patients away from palliation with a univentricular heart. The optimal approach to maintaining patency of the fetal atrial septum is less clear-cut with the potential for recurrent restriction in the absence of an atrial stent, which may be more technically challenging.10) Future challenges with fetal interventions may include creating centers of excellence, as a significant learning curve exist and may not be tolerated as demand for optimal outcomes becomes the norm.11)
EVOLVING APPROACHES AND CHALLENGES TO INTERVENTION FOR SEPTAL DEFECTS
Transcatheter secundum ASD closure has largely replaced surgery, however alternative morphological substrates remain a challenge, predominantly due to concerns over device stability. A recent report demonstrated successful closure of a superior sinus venosus defect using a covered stent within the superior vena cava allowing simultaneous redirection of flow from anomalous right upper pulmonary vein into the left atrium.1) The report is notable for the meticulous pre-procedural planning with the use of three-dimensional (3-D) printed models facilitating testing of the concept within the proposed patient's exact anatomy. This report emphasizes the need for patient specific approaches to more complex lesions with technology now providing us the opportunity to model the approach in an exact anatomical replica prior to the proposed intervention, as will be discussed later in the article. Transcatheter closure of rarer defects such as those involving the coronary sinus have also been reported although again detailed pre-procedural evaluation is recommended.12) Inferior sinus venosus defects provide very specific anatomical challenges, however successful closure of defects with deficient postero-inferior rims, although classically associated with high rates of device embolization, are available.13) Ultimately extension of this technology to encompass successful transcatheter closure of all forms of ASDs will require device development. However considering the limited numbers of these defects and the significant costs associated with device development and approval, this scenario remains unlikely in the short to medium term.
Device closure of ventricular septal defects (VSDs) in small infants remains a challenge, as the majority of VSD's exist in anatomically unfavorable locations within the ventricular septum, and are usually clinically important soon after birth, when navigating stiff delivery sheaths around the heart may lead to hemodynamic instability. Avoiding the need for splinting the smaller heart with stiffer wires and sheaths is possible using a perventricular approach with good outcomes,14) however a sternotomy is required. Other approaches to circumvent the need for an arteriovenous loop for device delivery with potential consequent valve distortion have included transseptal or retrograde arterial approaches.15)16) Less invasive approaches are also in development with perventricular closure performed with laparoscopic guidance through the chest wall.
Perimembranous defects provide very specific anatomic challenges nestled between the tricuspid and aortic valves and close to the conduction system. Identifying favorable anatomical variances including aneurismal tissue within the VSD,17) along with newer device designs have helped reduce rates of heart block.18) Retrograde delivery of larger devices via a carotid approach has facilitated closure of membranous VSDs in smaller infant who would have otherwise required surgical closure (Figure 1). Newer device design and application of softer existing devices has facilitated successful closure of primembranousVSDs with aortic valve prolapse (Figure 2) and doubly committed sub-arterial VSDs. Ultimately investment in device design is necessary to develop lower profile delivery systems and device characteristics that will ensure device stability with closure rates similar to surgery and minimal trauma to the conduction system.
Figure 1
Series of images outlining retrograde perimembranous VSD closure via a left common carotid cutdown in a 6.8 kg infant. (A, B) Patient positioning with feet pointing towards the head of the table to facilitate access to the left common carotid artery. (C) Insertion of 7 Fr short sheath following left common carotid cutdown. (D) Transesophageal echocardiography image demonstrating a 10 mm Occlutech membranous VSD occluder across the VSD. (E, F) Final LV and ascending aortic angiogram confirming the VSD device in position without residual leak or aortic incompetence.
LV = left ventricular; VSD = ventricular septal defect.
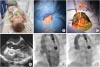
Figure 2
Series of images demonstrating transcatheter VSD closure in a patient with prolapse of the RCC of the aortic valve. (A) LV angiography demonstrating a moderate sized perimembranous VSD (white arrow). (B) Initial aortography demonstrating RCC prolapse (white arrow). (C) Short axis TOE image confirming the defect. (D) TOE image following deployment of 10 mm Lifetech eccentric membranous VSD occluder using a deflectable sheath to deploy from the LV cavity. (E) Final aortogram confirming no aortic incompetence and buffering of the RCC prolapse with the VSD device (white arrow). (F) Final colour Doppler TOE image in the short-axis confirming no residual leak across the ventricular septum.
LV = left ventricular; VSD = ventricular septal defect; RCC = right coronary cusp; TOE = transoesophageal echocardiography; VSD = ventricular septal defect.

The great paradox of congenital heart disease therapy is the need to provide polar opposite interventions on the heart. Whilst efforts are ongoing to provide a robust transcatheter alternative to surgical VSD closure, occasionally the need arises to create a VSD to decompress the left ventricle. Successful stenting of the ventricular septum following radiofrequency perforation has been reported,19) although this is a complex and challenging intervention usually required in smaller infants and therefore not to be undertaken without careful consideration. Whether development of nonthermal, mechanical tissue fractionation using high-intensity ultrasound pulses, or histotripsy will evolve to provide a safer less invasive option for creation of both atrial and ventricular septal communications, remains to be seen.20)
INTERVENTIONS IN SMALLER INFANTS
Progression towards less invasive interventions in smaller infants is an inevitable marker of progress within the field of congenital heart disease. Registry data, however, has shown that morbidity and mortality is not insignificant in low birth weight infants with adverse events reported in over a quarter of infants weighing <2 kg at the time of intervention.21) Multiple variables including type of procedure are likely to be involved. More promising outcomes have been seen with recent reports of transcatheter patent ductus arteriosus occlusion in extremely low birth weight infants, with procedural weights as low as 800 g.22)23) Randomized trials comparing outcomes with surgery and indeed non-intervention to determine if this approach, although technically feasible, improves longer-term morbidity and survival are needed.
Stenting of the arterial duct has re-emerged, following initially disappointing outcomes, particularly since the description of the hybrid approach to hypoplastic left heart syndrome.24) Some centers primarily using this approach for palliation of hypoplastic left heart syndrome have described excellent outcomes with unadjusted survival rates of 84% at one year,25) surpassing standard Norwood surgical result of many contemporary series. Recent registry data would also suggest that procedure outcomes are less affected by volume of procedures with comparable results seen with low and high volume centers.26) No randomized trial data however has been published and in the majority of centers, the hybrid approach is restricted for higher risk cohorts.27) Stenting of the arterial duct to maintain a source of pulmonary blood flow is also evolving perhaps as a consequence of ongoing concerns with outcomes following the surgical alternative of a systemic to pulmonary artery shunt. Two large recent retrospective analyses comparing ductal stenting to surgical shunts have shown favorable outcomes in relation to post-procedural recovery and length of intensive care unit (ICU) stay,27) as well as early and late survival,28) in the ductal stented cohorts. Again this has occurred in spite of the lack of a stent designed specifically for this purpose.
Right ventricular outflow tract (RVOT) stenting in symptomatic infants with tetralogy of Fallot has also evolved to compete with surgical palliation in recent years, leading to shorter ICU and total hospital stay as well as better pulmonary artery growth.29)30) However, the presence of a metal stent within the RVOT may have consequences for subsequent complete surgical repair.31) Stenting across the pulmonary annulus commits the patient to a transannular patch and the long-term impacts of chronic pulmonary regurgitation. Efforts to preserve pulmonary valve function in this setting continue to provide a huge challenge to all involved in care of these patients. Whether advances in transcatheter ablation techniques and equipment may resurrect attempts to remodel subpulmonic muscle bundles and promote growth of the pulmonary annulus, thus augmenting efforts to preserve pulmonary valve function, remains to be seen.32)
HYBRID INTERVENTIONS AND IMAGING PLATFORMS
Hybrid palliation, outside of those already mentioned above, include intraoperative pulmonary artery stenting,33) vascular cutdowns for neonatal interventions,34) as well as transcatheter pulmonary valve replacement.35) Indeed the limits of this approach are bound less and less by anatomical challenges, placing major emphasis on the need for collaboration between surgeon and interventionalist as well as developing an environment that is conducive to both teams working comfortably and efficiently in the same area. Although most large congenital heart disease (CHD) treatment centers now include a hybrid catheterization laboratory, to date guidelines on appropriate layout for such a space and staffing requirements are lacking, as is consensus on appropriate lesions that may be treated in this way and strategies to do so. As the boundaries of reducing procedural mortality are tested, the consequences of smaller hemodynamic alterations become greater. Use of exist angiography has been shown to elucidate unexpected residual anatomical distortions in 56% of patients undergoing surgical correction of congenital heart disease lesions leading to a change in therapeutic management in 50% of this cohort.36)
Significant advances have been made with newer intra-procedural imaging platforms focusing on radiation dose reduction, imaging quality and also advanced imaging modalities, fusing pre-procedural imaging with live acquisition images, or creating 3-D images through rotational angiography. Echocardiography-acquired images can be superimposed onto fluoroscopy images to guide complex closure procedures.37) In a contemporary series of 114 3-D rotational studies in CHD patients, rotational angiography with multiplanar reconstruction was judged to be superior to the diagnostic quality of fixed plane angiography.38) Additional benefits include assessment of nearby structures including the airways that may impact the interventional approach.39) Ultimately however, these imaging modalities are represented on a 2-D screen. Holography provides images created in real time from volumetric data, which float in the air during the procedure, in front of the operator and could provide an intuitive and interactive 3-D display for the interventionalist. Early experience in a clinical setting has been reported,40) however it is unclear as yet how this will translate into guiding interventional outcomes in a meaningful way.
TRANSCATHETER VALVE REPLACEMENT
In the space of 15 years, transcatheter pulmonary valve replacement has evolved to become the procedure of choice to restore pulmonary valve function in appropriately sized dysfunctional right ventricular (RV) to pulmonary artery conduits. Promising short-term results have been substantiated with medium term follow-up demonstrating freedom from need for explantation of 92% at 5 years.41) Evolution of this intervention has brought with it a new set of considerations for the internationalist. Compression of surrounding structures including the coronary arteries,42) distortion of the aorta with potential for aorto-pulmonary fistulae,43) and endocarditis with reported rates of up to 8% with the Melody valve (Medtronic Inc., Minneapolis, MN, USA),44) have all evolved in the consciousness of the interventional community as this procedure has grown. Growing experience with the procedure has lead to reports describing mounting of the pre-stent onto the valve system reducing the steps required for successful valve implantation,45) and extension to patients with smaller RV-PA conduits and bioprsothetic valves.46)47) Limitations due to valve size in patients with dilated native RVOTs have been met with larger-diameter balloon expandable systems,48) with simplification of the technique in these patients obviating the need for pre-stenting (Figure 3). Many dysfunctional RVOT's however remain too large for current balloon expandable systems and clinical experience with a number of self-expanding systems have been reported.49)50)51) It is likely that the variety of anatomical substrates may require a number of different options, with clinical trials on a RVOT flow reducer due to start soon in the US. Hybrid options for the dilated RVOT have also been reported to surgically reduce the size of the RVOT,35) or provide simultaneous internal fillers during valve deployment via a subxiphoid approach.52)
Figure 3
Series of images demonstrating transcatheter pulmonary valve replacement with Venus P valve in a patient with a previous transannular patch. (A) Initial MPA angiogram in the lateral projection confirming a dilated RVOT with free pulmonary incompetence. (B) Balloon sizing demonstrated waisting at 33 mm. (C) Angiography with valve deployment within the left pulmonary artery. (D) Post valve deployment angiography in the main pulmonary artery confirming valvar competence. (E) En-face view of the valve demonstrating near circularity of the valve with no distortion of the aorta seen with aortic angiography. (F) Transthoracic echocardiography with color Doppler confirming no pulmonary incompetence.
MPA = main pulmonary artery; RVOT = right ventricular outflow tract.

Transcatheter valve replacement in CHD patients has evolved beyond the pulmonary valve.53) Of particular interest is the growing experience of hybrid mitral valve replacement with the Melody valve.54) This facilitates avoidance of vitamin K antagonist anticoagulation with potential for “valve growth” as the valve is dilated via the transseptal approach over time. The issue of how to deal with somatic growth remains unique to the CHD population. Although the properties of the Melody valve that facilitate valve function at a variety of diameters are attractive in the short-term, ultimately harnessing advances in tissue engineering to develop a valve with true growth potential has become one of the challenges for the future of this specialty.
BIORESORBABLE MATERIALS AND TISSUE ENGINEERING IN CONGENITAL HEART INTERVENTIONS
Congenital interventionalists have benefited from advances in other fields of medicine to provide an array of stent sizes and designs for various vessels, albeit none designed specifically for patients with congenital heart disease. This has broadened our scope, however we remain limited by the challenge of somatic growth. Numerous approaches have been reported to deal with somatic outgrowth including high pressure balloon induced fracturing of small diameter stents,55) or novel stent designs, consisting of 2 stent halves connected by reabsorbable sutures.56) Many of the challenges relating to patient size and stenting could be overcome by a bioresorbable option. Indeed in a recent needs analysis survey amongst congenital interventionalists, 41% of respondents chose an appropriate bioresorbable scaffold as the device they would like to have access to, with 27% indicating this would have the greatest impact on improving the morbidity of their patients.57) Experience with currently available coronary scaffolds in CHD lesions has been disappointing with restenosis rates suggesting lack of appropriate radial strength,58) mirroring concerns seen following coronary interventions. The benefits in this cohort of patients are arguably even greater than in adult patients particularly if restoration of vascular function can be achieved in the diseased vessel. Development of a dedicated bioresorbable scaffold for CHD patients is greatly needed, perhaps consisting of a hybrid polymer/biocorrodible material that will provide adequate radial strength at a low enough profile to allow vessel remodeling and promote normal vessel growth.
Bioresorbable occluders particularly for the atrial septum are also attractive particularly with potential for increasing need to access the left atrium in later life. Clinical experience with partially bioresorbable occluders exists,59) however technical concerns (12% implantation failure) and early and late complications rates of 9% and 12% respectively have limited widespread acceptance.60) Clinical trials evaluating completely bioresorbable occluders are ongoing, however the optimal mechanical and degradations properties for a suitable biomaterial for transcatheter ASD closure have yet to be fully elucidated.
REGISTRIES, RISK CALCULATORS, AND DECISION MAKING
Adequate data collection around congenital cardiac interventions has lagged behind adult cardiology and congenital cardiac surgery. Guidelines for interventions in adult congenital heart disease patients were included in a 2008 document,61) with guidelines for interventions in pediatric patients published in 2011.62) There are minor variances in suggested timings of intervention but these documents provide a framework to guide clinical decision-making. However, providing guidelines is only part of the solution. Many more decisions are involved in performing a specific intervention and efforts to reduce variation in practice with the introduction of a standardized clinical assessment and management plan (SCAMP) has been reported.63) Ultimately, part of the journey to come for interventionalists will involve the development of a greater understanding of what influences our decision-making. We are all susceptible to a number of different subconscious traps and biases and it is inevitable that these decisions may impact delivery of care.64) The broader acceptance of the need to submit data from individual units to a registry may help identify suboptimal practice, although these data may not fully identify the reasons why. These registries include procedure specific registries as seen with the Congenital Cardiovascular Interventional Study Consortium (CCISC), or broader registries such as Congenital Cardiac Catheterization Project on Outcomes (C3PO), which uses prospective CHD data across a number of pediatric institutions or Improving Pediatric and Adult Congenital Treatment (IMPACT), which forms part of a National Cardiovascular Data Registry. For the first time since the inception of this specialty, meaningful pooled data are now available to assist in counseling patients and parents regarding the outcomes of interventions in patient subgroups, including the increased risks seen with interventions in children <2 kg,21) and the outcomes of children undergoing balloon aortic valvuloplasty.65) These registries are also providing information for risk adjusted scoring systems such as Catheterization for Congenital Heart Disease Adjustment for Risk Method (CHARM)66) and Catheterization Risk Score for Pediatrics (CRISP)67) facilitating a pre-procedural risk score for a specific intervention in low- and high-risk patients. Finally, these registries are evolving to assess quality metrics in participating centers, providing benchmark goals for radiation doses for specific procedures amongst other outcomes variables.68) The importance of these data may as yet be underestimated, considering the potential impact of radiation exposure through repeated cardiac catheterization on lifetime cancer risk in adults with congenital heart disease.69)
PERSONALISED DEVICE DESIGN AND EVOLVING INTERVENTIONS
There are a number of evolving interventions that are gaining traction at present including transcatheter creation of a reverse Potts shunt for patients with RV failure on the background of severe pulmonary hypertension (Figure 4).70) Efforts are ongoing to provide a viable transcatheter alternative to completion of a total cavopulmonary shunt,71) avoiding the need for further surgery and cardiopulmonary bypass on an already compromised circulation. Indeed magnetic resonance imaging (MRI)-guided creation of a superior cavopulmonary shunt has been described in a porcine model,72) and one may wonder if future palliation of some single ventricle conditions may obviate the need for surgery at all and whether we will be performing these interventions without the need for ionizing radiation.73) There are a number of other novel ideas reported having undergone in vitro and non-clinical testing.74)75)76)
Figure 4
Series of images demonstrating transcatheter creation of a reverse Pott's shunt. (A) Initial simultaneous angiography in the descending aorta and main pulmonary artery confirming the proximity of the dilated left pulmonary artery to the descending aorta (white arrows). (B) Deflectable sheath used to advance RF wire (white arrow) towards goose-neck snare in the pulmonary artery. (C) Repeat simultaneous angiography in the descending aorta and pulmonary artery demonstrating separation of the 2 vessels following RF perforation (white arrows). (D) Aortic angiography following implantation of 10×37 mm covered stent and post dilation with 14 mm balloon (white arrow). (E) Pulmonary artery angiography demonstrating right-to-left shunt across the newly created reverse Pott's shunt (white arrow).
RF = radiofrequency.

The future of our specialty will continue to be driven by the need to restore normal physiology with the least invasive means possible. It is clear that this approach cannot be obtained with “a one size fits all” approach. As imaging modalities evolve, it will be possible to compute pre-procedurally variations in anatomical repair and determine the impact on flow patterns. The impact of variations in inferior conduit anastomoses upon Fontan circuit efficiency has been reported.77) Similarly minor flow disturbances may mediate low-grade inflammation in the setting of repaired coarctation of the aorta.78) This may lead to arterial remodeling and impact upon emergence of systolic hypertension in young adulthood. These variances in flow can be measured by MRI.79) Again it is conceivable that modeling of coarctation of the aorta will facilitate a variety of virtual therapies to ensure that the most physiological treatment is provided. A similar approach could be envisaged for septal defect closure with 3-D model printing of bespoke devices from a bioresorbable polymer for individual patients.
Finally, as the field of transcatheter valve replacement continues to expand, focus will need to be directed towards the need for growth. Harnessing the broader medical interest in tissue engineering to patients with CHD, who may benefit most from this technology is paramount. The basic concept is to create living material made by cellularized grafts that, once implanted into the heart, grows and remodels in parallel with the recipient organ (Figure 5). Antenatal identification of congenital heart disease may facilitate early collection of cord cells with development of a cellularized graft or valve, harnessed to a bioresorbable scaffold, delivered via a minimally invasive approach opens up the potential of a one-stage, non-surgical “curative” procedure for these patients.80)
Figure 5
Cartoon illustrating possible future strategies for the surgical management of newborns with CHD. If CHD is diagnosed prenatally, fetal cells may be harvested and iPS generated; as an alternative, umbilical cord stem cells can be isolated at the time of birth. When diagnosis of CHD is made after birth or in babies who require a palliative surgical operation soon after birth, stem cells may be isolated from surgical cardiac leftovers. All these types of cells will allow the generation of a tissue-engineered graft endowed with growth and remodeling potential, necessary for the definitive correction of cardiac defects. Taken from Avolio et al.80)
CHD = congenital heart disease; iPS = induced pluripotent stem cells.

CONCLUSION
In summary, much has been achieved however, much more has yet to be realized. Historically, although at the forefront of innovation, congenital cardiac interventionalists have all too often been left to tail-coat on rapid advances made in adult interventions and left to improvise. Dedicated device requires support from industry and academia with international device registries providing ongoing safety and efficacy data. Future potentials to extend the remit for minimally invasive therapies requires collaboration and continued development of a dedicated environment and tools to maximize optimal outcomes. The potential of personalized “curative” therapies is achievable within a generation however vision and dedication are required from the specialty as a whole to achieve this.
 XML Download
XML Download