

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Percutaneous coronary intervention (PCI) is the main strategy for the treatment of obstructive coronary artery disease (CAD).1) In addition, with recent advances in devices and adjuvant pharmacologic agents, PCI indications were expanded to the high-risk patients.2) However, when taking the entire clinical practice into account, limited data are available to describe nationwide contemporary practice patterns of PCI in Korea. Recent registry studies have analyzed the current status of PCI in Korea.3)4) However, these studies analyzed limited populations, with particularly focusing on relatively higher PCI volume centers. Therefore, using claims data of the National Health Insurance (NHI) in South Korea, we sought to evaluate nationwide trends, characteristics, and clinical outcomes of patients undergoing PCI in Korea.
METHODS
Data sources
In Korea, all healthcare providers have had to join the NHI system on a fee-for-service basis. The Health Insurance Review & Assessment Service (HIRA) is a quasi-governmental organization that systematically reviews medical fees to minimize the risk of redundant and unnecessary medical services. Consequently, all NHI claims are reviewed by the HIRA.5) For this study, data from the 2011–2015 claims records of the HIRA were used. Diagnosis codes were used according to the International Classification of Diseases, 10th revision (ICD-10). In addition, specific information about the drugs, devices, and procedures were identified by codes from the HIRA database.5)6) This study was approved by the local Institutional Review Board of Ulsan University Hospital, Ulsan, Korea (approval number: 2016-10-022).
Study population
From the claims database of the HIRA between July 2011 and June 2015, we identified patients aged 18 years and older who had undergone PCI (M6551, M6552, M6561–4, M6571, and M6572) for the diagnosis of CAD (ICD-10 codes I20.X–I25.X). To examine national trends in patients with the first episode of CAD, patients with at least 6 months of eligibility prior to the index day were selected. Specifically, we excluded patients if the HIRA database indicated that they had a previous history of CAD (ICD-10 codes I20.X–25.X) within 6 months of the index day to ensure that it was the patients' first episode of CAD. Additionally, patients were categorized as either those with acute myocardial infarction (AMI) or angina pectoris and analyzed separately. AMI was defined by using the hospital discharge databases of the HIRA (ICD-10 codes I21.X–I22.X)
Study variables
The ICD-10 codes were used to identify comorbid conditions, such as diabetes mellitus, diabetes mellitus with chronic complications, hyperlipidemia, hypertension, congestive heart failure, arrhythmia, valvular disease, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, moderate to severe liver disease, renal disease, cancer, and rheumatic disease.7)8) The Charlson comorbidity index (CCI) was obtained from the ICD-10 codes.7) In the HIRA database, all prescribed medications were recorded with rigorous accuracy. Patients were also considered to have diabetes mellitus, hypertension, and hyperlipidemia if anti-diabetic, anti-hypertensive, and anti-hyperlipidemic drugs were identified from the medication codes within 6 months of the index day. Furthermore, we identified used medications, such as anti-platelet agents, statins, beta-blockers, and angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs).6)
We classified claims as drug-eluting stents (DESs) if DES device codes (J5083XXX) appeared. The claims were designated as bare metal stents (BMSs) if there were BMS device codes (J5231XXX). The claims were also assigned as a non-stent coronary balloon angioplasty if device codes were unaccompanied by any code indicating a DES or BMS.
Clinical outcomes and medical costs
Death was identified by all in- and out-patient claims that indicated death. Myocardial infarction was defined using the hospital discharge databases of the HIRA (ICD-10 codes I21.X–22.X). Coronary revascularizations in the HIRA database were identified using the procedure codes of PCI (M6551, M6552, M6561–4, M6571, and M6572) and coronary artery bypass surgery (O1641, O1642, O1647, OA641, OA642, and OA647). In this current study, for the evaluation of clinical outcomes, the HIRA database was used until July 2016.9) In patients with multiple events, the first event was considered to be the component of the composite outcome.
We also examined and calculated medical costs on the basis of the Korean Won (KRW). Total medical costs were defined as the sum of 3 direct medical costs: inpatient care, outpatient care, and prescription drugs. We assessed 1-year medical costs regardless of events. For the measurement of CAD-related medical costs, we obtained CAD-related claim costs from the HIRA databases (ICD-10 codes I20–25).10)
Statistical analysis
We summarized patient characteristics, procedure/drug information and medical costs from 2011 to 2015 by presenting the mean±standard deviation or frequency (percentage) for continuous or categorical variables, respectively. We analyzed the 5-years trend based on the χ2 test, the logistic regression or the linear regression according to the categorical or the continuous variables. When there are more than three categories such as the device information, we used the multinomial logistic regression model. Survival outcomes, such as all-cause death and death/coronary revascularization, were summarized by the Kaplan-Meier method. Cumulative incidence rates between the angina and AMI groups were compared using the log-rank test. Furthermore, the Cox regression model was used to detect any trend from July 2011 to June 2015 after truncating the survival outcomes at the 1-year time point. Statistical significance was defined as p<0.05 for all two-tailed tests. All data analysis was performed using the R software version 3.3.1 (R Foundation for Statistical Computing, Vienna, Austria; www.r-project.org).
RESULTS
PCI trends across Korea
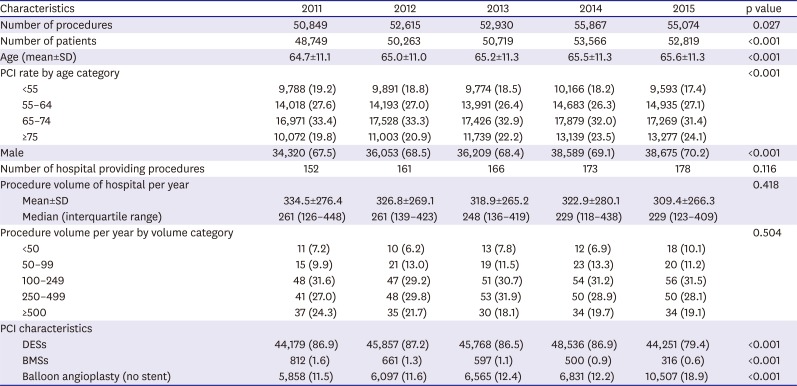
Between 2011 and 2015, a total of 256,116 patients who underwent 267,335 PCI procedures were identified from the claims database of HIRA (Table 1). During a period of 5 years, PCI became more prevalent over time, increasing from 50,849 procedures in 2011 to 55,074 procedures in 2015 (an 8% increase). The mean age of patients and the proportion of male also increased during the same time period. Furthermore, a 17% increase in the number of PCI-providing hospitals occurred between 2011 and 2015 (152 versus 178 hospitals), with a gradual decrease in the mean caseload per hospital (334.5±276.4 in 2011 vs. 309.4±266.3 in 2015). In the PCI procedures, DES was the most frequent device (n=228,591, 85.3%), followed by balloon angioplasty (n=35,858, 13.4%) and BMS (n=2,886, 1.1%). In addition, although DES and BMS showed a gradual decrease over time, balloon angioplasty gradually increased during this period of 5 years.
Table 1
Characteristics of patients who underwent PCI and of hospitals that performed PCI in Korea between 2011 and 2015
Characteristics in patients undergoing PCI
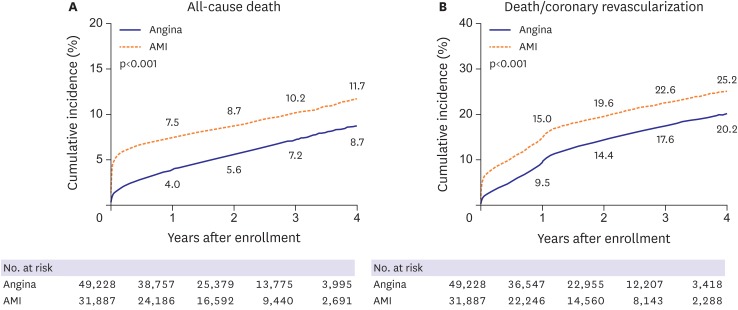
Among patients undergoing PCI, 81,115 patients met the eligibility criteria for the first episode of CAD and were included in the study population (Figure 1). Between July 2011 and June 2015, HIRA claims data indicated that PCI procedures were performed for angina pectoris (n=49,288, 60.7%) or AMI (n=31,887, 39.3%). The mean age of patients was 64.4±12.2 years and 56,576 (69.7%) were men. Diabetes, hyperlipidemia, and hypertension were observed in 27,086 (33.4%), 30,675 (37.8%), and 45,389 (56.0%) patients, respectively. Patients with angina were older and had more comorbid conditions than those with AMI (Table 2). In PCI procedures, DES was the most frequently used treatment modality (93.2%). BMS and balloon angioplasty were also used in 1.3% and 5.5% of patients. The mean number of stents per patient was 1.39±0.64. At discharge, aspirin, P2Y12 inhibitors, statins, beta-blockers, and ACEI or ARB were provided to 76,778 (94.7%), 80,089 (98.7%), 71,411 (88.0%), 57,429 (70.8%), and 54,418 (67.1%) patients, respectively. The mean in-hospital and 1-year total medical costs were 8,628,768±4,832,075 and 13,128,158±9,758,753 KRW. In-hospital mortality occurred in 2,094 patients (2.6%). During the follow-up period (median 2.1 [interquartile range, 1.1–3.2] years), 5,849 (7.2%) deaths and 7,884 (9.7%) coronary revascularizations were observed (Figure 2).
Figure 1
Overview of the study population.
CAD = coronary artery disease; HIRA = Health Insurance Review & Assessment Service; AMI = acute myocardial infarction; PCI = percutaneous coronary intervention.
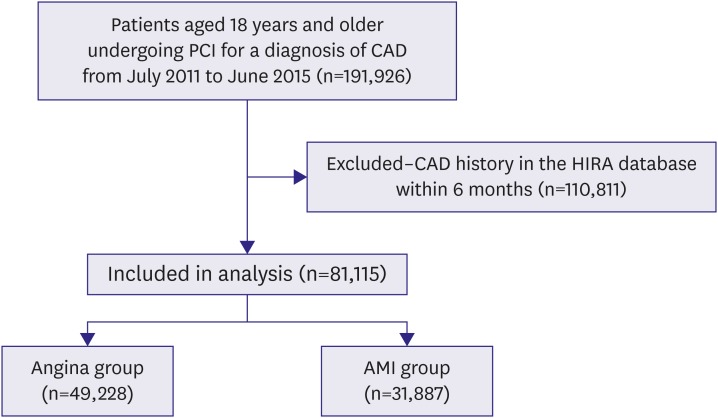
Table 2
Characteristics of patients who underwent PCI in Korea between 2011 and 2015
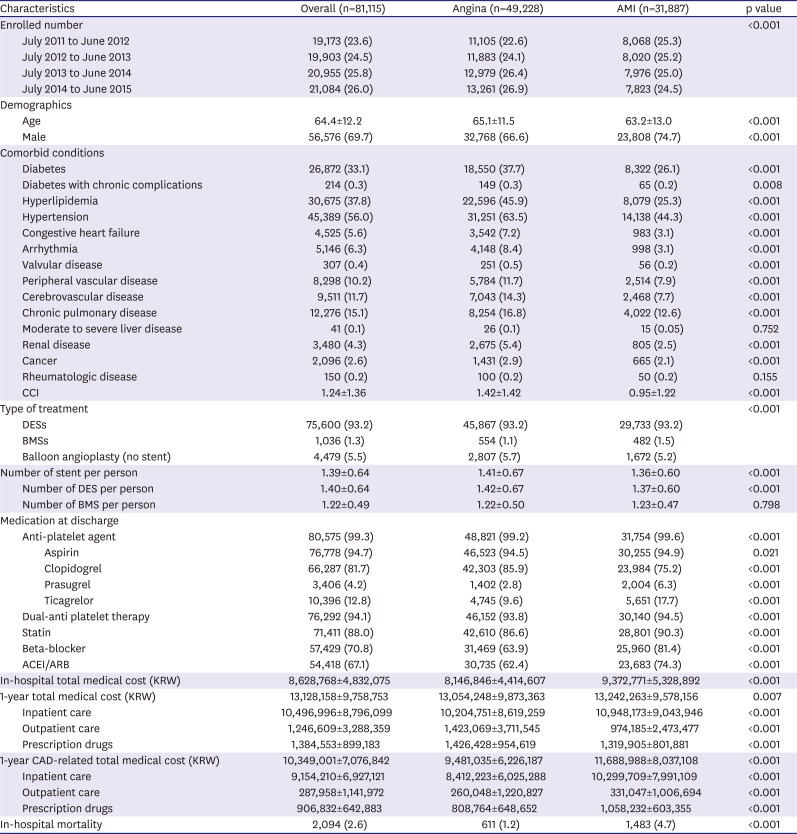
Data shown are number (%) or mean±SD.
ACEI = angiotensin-converting enzyme inhibitor; AMI = acute myocardial infarction; ARB = angiotensin receptor blocker; BMS = bare metal stent; CAD = coronary artery disease; CCI = Charlson comorbidity index; DES = drug-eluting stent; KRW = Korean Won; PCI = percutaneous coronary intervention; SD = standard deviation.
Trends in patients undergoing PCI for angina
In patients undergoing PCI for angina (Table 3), a 10% increase in the number of patients was noted between 2011–2012 and 2014–2015 (11,105 vs. 13,261; p=0.021). The average age of patients and proportion of male increased over time. However, there was no significant difference in comorbid conditions of patients, reflected by the CCI. In PCI procedures, the proportion of patients treated with DES showed a modest increase for 4 years. On the contrary, the proportion of BMS significantly decreased during the same period. The mean number of stents per patient decreased from 1.42±0.66 in 2011–2012 and 1.40±0.69 in 2014–2015. In the discharge medications, although the use of statins was much improved over 4 years, the use of ACEI or ARB was significantly reduced. The 1-year total and CAD-related medical costs significantly decreased from 2011–2012 to 2014–2015, which was mainly due to the reduction of in-hospital medical costs. However, no significant differences were found in the incidence of clinical outcomes for 4 years.
Table 3
Characteristics of patients with angina who underwent PCI in Korea between 2011 and 2015
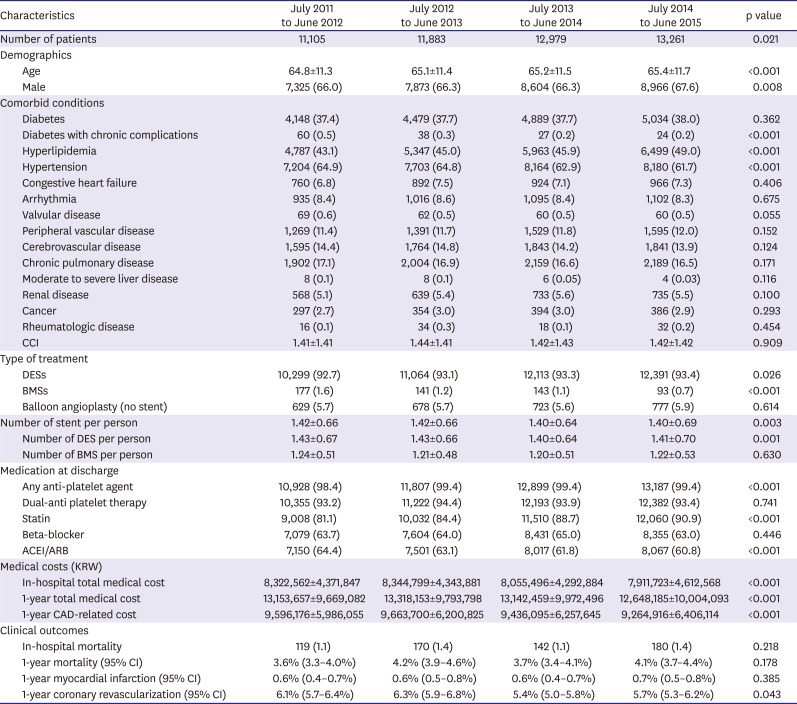
Data shown are number (%) or mean±SD.
ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; BMS = bare metal stent; CAD = coronary artery disease; CCI = Charlson comorbidity index; CI = confidence interval; DES = drug-eluting stent; KRW = Korean Won; PCI = percutaneous coronary intervention; SD = standard deviation.
Trends in patients undergoing PCI for AMI
In patients who underwent PCI for AMI (Table 4), the number of patients marginally decreased between 2011–2012 and 2014–2015 (8,068 vs. 7,823; p=0.052). The proportion of male significantly increased during 4 years. However, the mean age and CCI of patients did not differ during same period. In PCI procedures, DES was the most commonly used device with a modest increase. Conversely, the use of BMS significantly decreased over time. In the discharge medications, the use of statins was significantly increased. However, beta-blockers and ACEI or ARB use was significantly reduced. In-hospital medical costs gradually decreased from 2011–2012 to 2014–2015. However, the improvement in clinical outcomes was not observed.
Table 4
Characteristics of patients with AMI who underwent PCI in Korea between 2011 and 2015
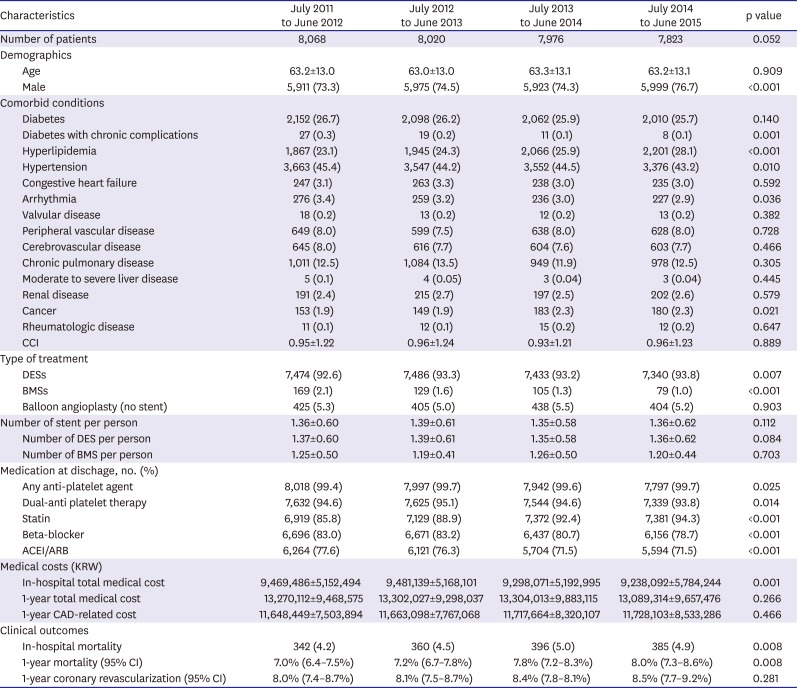
Data shown are number (%) or mean±SD.
ACEI = angiotensin-converting enzyme inhibitor; AMI = acute myocardial infarction; ARB = angiotensin receptor blocker; BMS = bare metal stent; CAD = coronary artery disease; CCI = Charlson comorbidity index; CI = confidence interval; DES = drug-eluting stent; KRW = Korean Won; PCI = percutaneous coronary intervention; SD = standard deviation.
DISCUSSION
In the present analysis using NHI claims data in Korea, our main findings were as follows: 1) In patients who underwent PCI for the first episode of CAD, the number of patients for angina significantly increased, but the number of those for AMI marginally decreased; 2) Irrespective of clinical presentations, DES was the most commonly used device; 3) The use of medication at discharge was still inappropriate and clinical outcomes did not improve between 2011–2012 and 2014–2015.
There are limited data available to provide a contemporary snapshot of PCI in Korea. A recent large-scale multicenter registry described the current status of PCI in Korea.3)4) However, these efforts may be limited somewhat either by short-term clinical outcomes or institutional selection. Therefore, considering the nationwide situation in clinical practices, this present study was designed. Well-controlled and reliable data from the HIRA database in Korea (i.e., a quasigovernmental organization) enabled to provide an overview of the national trends for PCI. In addition, compared with the 2014 Korean Percutaneous Coronary Intervention (K-PCI) registry,3)4) the similar age ranges for patients and similar proportion of male, diabetes, hypertension, hyperlipidemia, and intervention for AMI or angina were noted. The frequency of DES usage (93.2% vs. 91.3%) and in-hospital mortality (2.6% vs. 2.3%) did not differ between our study and the 2014 K-PCI registry. Therefore, we believe that this study reflects the contemporary status of PCI in Korea.
In Korean patients undergoing PCI for the first episode of CAD, the total number of PCI procedures increased between 2011 and 2015, with a progressive increase of patients with angina and a gradual decline of those with AMI. With cognition of importance and impact of cardiovascular disease, in many western countries, health programs have been developed for the prevention and management of major cardiovascular risk factors such as diabetes, hypertension, and hyperlipidemia.11)12) Consequently, control of these cardiovascular risk factors has improved cardiovascular outcomes in these countries.13)14) In Korea, CAD has become one of the leading causes of death because of prolonged life expectancy and rapid westernization.15)16) In the present study, no significant changes in comorbid conditions reflected by the CCI were detected in angina group between 2011–2012 and 2014–2015. However, the absolute number of patients with major risk diseases such as diabetes, hyperlipidemia, and hypertension increased in the same period. In AMI group, although the proportion of diabetes or hypertension was stabilized, the proportion of hyperlipidemia also increased during 4 years. Therefore, to reduce the burden of CAD in Korea, tailored management for cardiovascular risk factors with a risk prediction model, considering differences of risk factors attributable to development of CAD in a Korean population, is necessary.
In the early-generation DES, clinical data were challenged by less favorable long-term safety issues such as stent thrombosis and late failure.17)18) Accordingly, these findings led to a marked improvement in stent design, and the development of new drugs and drug-carrier systems. Based on these enhanced properties, newer-generation DES demonstrated better clinical efficacy and safety than those of BMS and first-generation DES.19)20) A registry data also indicated that routine use of DES was associated with a decline in the incidence of restenosis and stent thrombosis.21) Furthermore, even in patients with ST-segment-elevation myocardial infarction, newer-generation DES showed advantages in efficacy and safety over BMS.22) Reflecting these findings, BMS use continued to decline between 2011 and 2015, while DES implantation was on the rise. DES has become the main strategy for PCI in Korea regardless of clinical presentations.
In the present study, clinical outcomes between 2011 and 2015 did not improve. To enhance clinical outcomes of patients with CAD, appropriate medical treatment is important.23) Optimal medical therapy (OMT), defined as the combination of at least 1 anti-platelet agent, statin, beta-blocker, and ACEI/ARB, is the suggested initial treatment strategy and recommended for all patients with CAD.24)25) In the SYNergy between percutaneous coronary intervention with TAXus and cardiac surgery (SYNTAX) trial, a post hoc analysis demonstrated that the lack of OMT was associated with adverse clinical outcomes of patients with complex CAD requiring coronary revascularization.24) However, in the current study, the number of patients taking OMT in the angina and AMI groups were 20,731 (42.1%) and 19,249 (60.4%), respectively. Overall, only 39,980 (49.3%) patients were taking OMT. Accordingly, the use of OMT remains suboptimal. In the literature, OMT provided clinical benefits in patients with CAD.24)25) Therefore, to improve clinical outcomes, OMT should be considered for all patients undergoing PCI unless contraindicated.
Our study had several limitations. First, the present study was based on administrative data from the HIRA in South Korea. Similar to previous studies using administrative databases, our study lacked patient clinical data and test findings. Thus, our findings might be limited by uncertainties in unmeasured confounding variables that may affect the management of patients.8)26) Second, although we used a database from a quasi-governmental organization, a possibility that these data did not fully reflect patient outcomes still exists. Additionally, we did not specify the cause of death.
This study provides a contemporary overview of PCI procedures performed in Korea. In addition, it provides an important perspective on many healthcare aspects, including trends, characteristics, clinical outcomes, and medical costs. Together with the further researches with nationwide database, we hope that this study encourages the further development of clinical guidelines and implementation of these guidelines into clinical practice to improve cardiovascular outcomes in Korea.
 XML Download
XML Download