

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The global prevalence and incidence of obesity are increasing worldwide because of urbanization, unhealthy dietary habits, and physical inactivity. Obesity is a major factor contributing to metabolic syndrome (MetS), which is a constellation of atherogenic metabolic risk factors for dyslipidemia, hypertension, and hyperglycemia. MetS is associated with the risk of developing cardiovascular disease that increases morbidity and mortality. In Korea, the prevalence of MetS and obesity has increased continuously and are now estimated at over 30% according to data from the Korea National Health and Nutrition Examination Survey (KNHANES).1)2)
Recent research has focused on the renin-angiotensin system (RAS) for its potential role in various aspects of MetS. The RAS is a crucial neuroendocrine system in maintaining body fluid and electrolyte balance. Short-term activated RAS acutely regulates the homeostasis of extracellular volume and blood pressure; however, its chronic activation is associated with obesity, dyslipidemia, insulin resistance, chronic kidney disease, and hypertension.3) Indeed, RAS blockades such as angiotensin-converting enzyme (ACE) inhibitors and angiotensin II type 1 receptor blockers (ARBs) are important therapeutic agents in the treatment of hypertension. RAS blockade may also serve as an effective treatment strategy to control impaired glucose tolerance and dyslipidemia in patients with MetS.4)
Several clinical trials have demonstrated the benefit of using RAS-blocking agents in prevention and treatment of MetS associated components and their complications.5)6)7) However, the associations of RAS components such as plasma renin activity (PRA), aldosterone, and aldosterone-to-PRA ratio with the parameters of MetS are not elucidated clearly. In the present study, we assessed the levels of RAS components in patients with and without MetS, and investigated the relationships between RAS components and MetS in a population of Korean adults.
METHODS
Study population
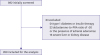
This was a multicenter, cross-sectional study which was performed from January 2016 to February 2017 in Korea. We screened consecutive patients aged ≥20 years who were referred to tertiary cardiology or endocrinology clinics to evaluate glucose metabolism, hypertension, or dyslipidemia status in 6 tertiary hospitals (Seoul National University Bundang Hospital, St. Vincent's Hospital of The Catholic University of Korea, Kyung Hee University Hospital at Gangdong, Keimyung University Dongsan Medical Center, Chungnam National University Hospital, and Chungbuk National University Hospital). Among 892 patients who underwent evaluation of RAS components, including PRA and aldosterone levels, we excluded those who were on current usage or previous usage of diuretics, β-blockers, or RAS blockers (such as ACE inhibitors or ARBs) within 12 weeks. Consequently, all enrolled participants were naïve to these agents for at least 12 weeks prior to the evaluation of RAS components. Patients who had type 1 diabetes mellitus (DM) (C-peptide <0.3 pg/mL) or who were receiving insulin therapy were also excluded from the study. We also excluded patients who were suspected of having primary aldosteronism, based on an aldosterone-to-PRA ratio of >30 or the presence of adrenal adenomas shown by imaging tests, and those with active malignancies or medical histories of severe liver or renal disease. Ultimately, 829 patient participants were enrolled after 63 were excluded (Figure 1). The present study was endorsed by the Clinical Study Committee of the Korean Society of Lipid and Atherosclerosis and approved by the institutional review board of Seoul National University Bundang Hospital (IRB-B-1601-332-307) and each study site. This study followed a retrospective design, therefore informed consent was waived by the institutional review board in all institutes.
Measurement of anthropometric and biochemical parameters
Height and body weight were measured to the nearest 0.1 cm and 0.1 kg, respectively, while patients were wearing only light clothing and according to standard procedures. Body mass index (BMI) was calculated by dividing weight in kilograms by the square of height in meters. Being overweight and obesity were defined as BMI ≥23 kg/m2 and BMI ≥25 kg/m2, respectively. Blood pressure was measured with the patient in a sitting position after at least 10 minutes rest using an automated blood pressure monitor at the time the patients visited the clinic. Smoking status was classified as currently smoking or not smoking. Alcohol consumption was assessed by asking the amount and frequency of beer, wine, or spirits intake during the previous 12 months, and a current heavy drinker was defined as someone consuming alcohol 3 times or more per week. Physical exercise was assessed by asking the number of days in which the participant performed moderate physical activity in the past week. Regular exercise was defined as three or more times of exercising for at least 20 minutes. The participants' comorbidities such as DM, hypertension, and dyslipidemia with any history of respective medications were identified through a comprehensive review of medical records. According to the American Diabetes Association 2017 guidelines, DM was defined by a fasting plasma glucose (FPG) concentration ≥126 mg/dL (7 mmol/L), or a level of glycated hemoglobin (HbA1c) ≥6.5%.8) Hypertension was defined according to the guidelines of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or the use of antihypertensive medication.9) Dyslipidemia was defined as follows: hypercholesterolemia (total cholesterol ≥240 mg/dL), high low-density lipoprotein (LDL)-cholesterol (≥160 mg/dL), low high-density lipoprotein (HDL)-cholesterol (<40 mg/dL), and high triglycerides (≥200 mg/dL) according to the guidelines of the National Cholesterol Education Program and Adult Treatment Panel III (ATP-III).10) Blood samples for the determination of RAS-related hormones, the primary parameters in this study, were drawn after at least 30 minutes of rest in the sitting position. Samples were collected into prechilled EDTA tubes, immediately placed on ice, and centrifuged at 4°C. Plasma was stored at −80°C until analysis. PRA and plasma aldosterone levels were measured by radioimmunoassay using commercial kits (Fujirebio Co., LTD, Tokyo, Japan and Beckman Coulter, Immunotech, Marseille, France, respectively). We adjusted for the site to account for the potential differences in measurement methods of serum aldosterone and PRA by the different institutions. Participants with MetS were identified by the ATP-III and International Diabetes Federation (IDF) criteria.11) The ATP-III guidelines define MetS as when 3 or more of the following components are present: abdominal obesity, serum triglycerides ≥150 mg/dL, HDL-cholesterol <40 mg/dL (men) or <50 mg/dL (women), blood pressure ≥130/85 mmHg, and FPG ≥100 mg/dL (or known DM). Because the IDF suggests ethnic specific values to define central obesity, we used the specific cut-points for the Asian population (waist circumference >90 cm for men and >80 cm for women).12)



Statistical analyses
The prevalence of MetS in Korea is estimated to be 5.2–31.7% among men and 9.0–40.1% among women.1) The criteria applied for MetS and age range of participants are important factors affecting the incidence of cardiometabolic diseases. In our cohort, we planned to recruit patients aged ≥20 years, so the expected prevalence of MetS would be 15–20% for either sex. We intended to investigate cardiometabolic events such as coronary artery disease, cerebrovascular disease, peripheral arterial occlusive disease, and DM in 3 years. On the assumption of a cardiometabolic event rate of 10% in women and 20% in men for 3 years, we calculated a total of 700 participants to be required for statistical analysis. With a conservative approach and sampling convenience in each site, we planned to recruit around 800 subjects with a 1:1 ratio of men and women in 2015–2016.
Continuous variables are presented as the mean and standard deviation (SD) and categorical variables as counts and percentages. Variables with nonnormal distributions (triglycerides, high-sensitivity C-reactive protein [hsCRP], urinary albumin-to-creatinine ratio, HOMA-IR, HOMA-β, and QUICKI) were logarithmically transformed to achieve a normal distribution. Differences in anthropometric and biochemical variables according to the patient participants' MetS status were evaluated using a Student's t-test. Pearson correlation was analyzed to investigate associations of RAS components with other metabolic parameters. Multiple linear regression analyses were performed to evaluate the associations of MetS components or insulin resistance with various metabolic factors including RAS components. p<0.05 was considered significant. The statistical analyses were performed using IBM SPSS Statistics for Windows (version 21; IBM Corp., Armonk, NY, USA).
RESULTS
Participant characteristics
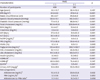
The anthropometric and biochemical characteristics of the participants are shown in Table 1. The mean±SD age of study subjects was 52.8±12.8 years and 56.3% were men. The prevalences of type 2 diabetes mellitus (T2DM), hypertension, and dyslipidemia were 50.8%, 38.7%, and 64.3%, respectively. Sixty-three point two percent of participants with diabetes were taking oral hypoglycemic agents, 37.4% of those with hypertension were taking antihypertensive agents, and 53.1% of those with dyslipidemia were taking lipid-lowering agents. The prevalence of MetS was 39.8%. The mean BMI was 25.9±3.8 kg/m2. The mean±SD of serum aldosterone, PRA, and aldosterone-to-PRA ratio were 17.5±23.8 ng/dL, 2.5±3.7 ng/mL/h, and 13.7±22.7, respectively.
Table 1
Baseline characteristics of the study participants (n=829)

Values are presented as the mean±SD for continuous variables or number (%) for categorical variables.
ACR, albumin-to-creatinine ratio; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BUN, blood urea nitrogen; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment for insulin resistance; HOMA-β, homeostasis model assessment for β-cell function; hsCRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein; MetS, metabolic syndrome; PRA, plasma renin activity; QUICKI, quantitative insulin sensitivity check index; RAS, renin-angiotensin system; SD, standard deviation; T2DM, type 2 diabetes mellitus.
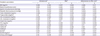
When the participants were divided into 2 groups according to the presence and absence of MetS, BMI, waist circumferences, blood pressure, lipid profiles, glucose metabolism status, and hsCRP levels were significantly different (Table 2). The participants with MetS were more obese, hypertensive, dyslipidemic, and insulin resistant than those in the control group.
Table 2
Characteristics of the participants according to MetS status
Values are presented as the mean±SD.
ACR, albumin-to-creatinine ratio; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BUN, blood urea nitrogen; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment for insulin resistance; HOMA-β, homeostasis model assessment for β-cell function; hsCRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein; MetS, metabolic syndrome; PRA, plasma renin activity; RAS, renin-angiotensin system; QUICKI, quantitative insulin sensitivity check index; SD, standard deviation.
*Log-transformed values were used for analysis. The p values for comparisons of variables between 2 groups were calculated using a Student's t-test.
Among the RAS components, the serum aldosterone levels were significantly higher in MetS group than in the control group (20.6±33.6 vs. 15.3±12.2 ng/dL, respectively, p<0.05) (Table 2 and Figure 2 for the mean±SD). However, other components such as PRA or aldosterone-to-PRA ratio were not different between the groups.

Correlation between RAS components and other clinical parameters
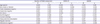
In the analysis of the correlation of the RAS activity with metabolic parameters (Table 3), waist circumferences, systolic and diastolic blood pressures, and triglycerides, which are constituents of MetS were positively correlated with serum aldosterone levels (r=0.228, 0.112, 0.108, and 0.181, respectively, all p<0.01). Serum aldosterone levels correlated positively with HbA1c and HOMA-IR (r=0.092 and 0.235, respectively, both p<0.05) and negatively with QUICKI (r=−0.254, p<0.001). In addition, there was a positive correlation of the hsCRP with serum aldosterone levels (r=0.174, p<0.001).
Table 3
Pearson correlation between RAS components and metabolic parameters
ACR, albumin-to-creatinine ratio; BMI, body mass index; FPG, fasting plasma glucose; HbA1c, glycated hemoglobin; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment for insulin resistance; HOMA-β, homeostasis model assessment for β-cell function; hsCRP, high-sensitivity C-reactive protein; LDL, low-density lipoprotein; PRA, plasma renin activity; RAS, renin-angiotensin system; QUICKI, quantitative insulin sensitivity check index.
*Log-transformed values were used for analysis.
Associations of clinical and biochemical parameters with aldosterone-to-PRA ratio
We evaluated whether basic anthropometric and biochemical parameters including RAS components were independently associated with the number of MetS components or insulin resistance parameters. In the multivariable linear regression analysis (Table 4), serum aldosterone level showed positive and independent association with the numbers of MetS components after adjusting for age, sex, total cholesterol, creatinine, alanine aminotransferase, hsCRP, smoking status, alcohol consumption, and exercise habits (p<0.01). In the multivariable regression analysis with HOMA-IR or QUICKI instead of the number of MetS components, aldosterone level was independently associated with these indices. By contrast, other RAS components, such as PRA or aldosterone-to-PRA ratio, were not significantly associated with the number of MetS components or insulin resistance.
Table 4
Associations of the number of MetS components or insulin resistance indices with various metabolic factors including circulating levels of aldosterone in multiple linear regression analyses
DISCUSSION
In this multicenter study, we found that the circulating level of aldosterone was significantly increased in the MetS group compared with the control group. Serum aldosterone levels were positively correlated with waist circumference, blood pressure, triglyceride, HbA1c, hsCRP, and HOMA-IR, and negatively correlated with QUICKI. Moreover, serum aldosterone level was independently associated with MetS components and insulin resistance indices, such as HOMA-IR or QUICKI, after adjusting for age, sex, total cholesterol, kidney function, liver function, hsCRP, and various health-related behaviors, such as alcohol consumption, smoking status, and exercise habit. These findings suggest that the serum aldosterone level is associated with insulin resistance, which plays a key pathogenic role in development of MetS.
Recent research has focused on the crosstalk between insulin signaling and the RAS.3) The RAS consists of a cascade of enzymatic reactions in which liver-derived angiotensinogen is cleaved by renin and released into the circulation to form angiotensin-I. Angiotensin-I is then converted to angiotensin II, which is a potent peptide for vasoconstriction and the release of aldosterone. In addition to this endocrine system, there is also a local or tissue RAS, which acts like a paracrine hormone system within the kidney, adipose tissue, heart, and blood vessels.15) Considerable evidence suggests that RAS may also be able to modulate insulin actions.3) Chronic activation of RAS is known to lead to both the onset of DM and the progression of its micro- and macrovascular complications.15) Moreover, its modulation with ACE inhibitors or ARBs have shown preventive and therapeutic effects for cardiovascular and renal damage in patients with DM.16)17)
From the perspective of blood pressure, not only patients with primary aldosteronism, but also individuals with normal blood pressure showed that serum aldosterone levels were associated with an elevation of blood pressure.18) Plasma aldosterone concentrations are also independently correlated with BMI in overweight patients in both hypertensive and normotensive patients.19)20) Hyperinsulinemia, and high levels of complement C1q tumor necrosis factor-related protein or fatty acid oxidation products, are reported to contribute to increased secretion of aldosterone in obese patients.21)22)
By contrast, associations between serum aldosterone level and parameters of impaired glucose tolerance, such as FPG and insulin resistance were suggested in observational studies.23)24) Hyperaldosteronism can contribute to impaired carbohydrate metabolism by attenuating insulin release from pancreatic β-cells because of hypokalemia, fibrosis, or inhibitory effect of steroid on β-cells. Associations between aldosterone production and insulin resistance assessed by an oral glucose tolerance test were demonstrated even in healthy and overweight individuals.20)25) Recent evidence supports a direct role for aldosterone in the development and progression of insulin resistance. The prevalence of insulin resistance in patients with primary aldosteronism was reported to be as high as 50%, and either surgical treatment or medical treatment of hyperaldosteronism restored normal insulin sensitivity.26)27)
Interestingly, previous studies that investigated the relationship between serum aldosterone levels and lipid metabolism have shown inconsistent findings. Some studies showed significant correlations between plasma aldosterone level and HDL-cholesterol or triglyceride levels, whereas others did not show any association.28)29) In the present study, serum aldosterone levels were significantly associated with serum triglyceride, but not with serum HDL-cholesterol levels.
Although measurement of PRA and serum aldosterone levels is not difficult or expensive, its clinical implication has not been fully investigated. Plasma aldosterone levels, but not PRA are associated with MetS in native Africans or African Americans.24) The longitudinal follow-up of the Framingham Offspring study demonstrated that the serum aldosterone levels, but not renin, are associated with the incidence of MetS and changes of metabolic risk factors.30) Furthermore, the causality and molecular interactions between aldosterone and insulin signaling are not fully elucidated. It is possible that hyperinsulinemia directly stimulates adrenocortical aldosterone production or potentiates angiotensin II-mediated aldosterone secretion.28) Increased levels of serum aldosterone may further decrease insulin sensitivity by induction of oxidative stress and inflammation, suppression of the insulin signaling pathway, regulation of hepatic gluconeogenesis, and impairment of adipocyte function.21)
There are several advantages and unique features of the present study. First, by contrast with previous studies of mainly black or white people of European ancestry, this is the first large scale study of a Korean population to investigate the relationship between serum aldosterone levels and MetS. Second, patients who were suspected of having primary aldosteronism were excluded. Third, all participants were drug-naïve, particularly for RAS-blocking agents. Therefore, the findings of the present study can help to explain the associations between RAS activity and MetS more precisely than previously understood.
Nevertheless, this study also has several limitations. First, because of the cross-sectional nature of the study design, which compared the data at the time of survey, conclusions regarding causality cannot be drawn. Second, we did not measure serum angiotensin II or ACE levels that might be able to prove the relationship between RAS activity and MetS. Prospective studies are needed to investigate the causal relationship between increase in aldosterone levels and future cardiometabolic events.
In conclusion, serum aldosterone levels were higher in Korean adults with MetS than in those without. Aldosterone levels were independently associated with MetS components and insulin resistance indices after adjusting for demographic, biochemical, and lifestyle factors. The present findings have clinical implications in demonstrating that measurement of circulating aldosterone concentration is helpful in assessing insulin resistance and the risk of MetS. Further mechanistic studies are needed to elucidate the causal relationship between increase in aldosterone levels and metabolic derangement.
 XML Download
XML Download