

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Performing invasive procedures including CAG in the setting of asymptomatic systolic HF is controversial. Angiography should also be considered in low ejection fraction (EF) patients with evidence of reversible myocardial ischemia on non-invasive testing.1) However, coronary angiography is applied for the elucidation of the etiology of low EF. As the prognosis of patients with ischemic etiology already remains worse,2) prediction of atherosclerosis burden may obviate the need for an unnecessary angiography with potential risks and harms to these vulnerable patients.
It is known that inflammation has a substantial role in the initiation and production of the complex atherosclerotic process3) that lies beneath cardiovascular disease (CVD). The role of inflammation in CVD has been studied and the relationship between various inflammatory markers has been established in the past.4)5) Platelets and leukocytes are the important components of these processes associated with the development of atherosclerosis6) Platelet-to-lymphocyte ratio (PLR) is a new prognostic index that integrates the risk prediction of these 2 parameters. It gives an idea about both the aggregation and inflammation pathways. Increased PLR values emerged as a valuable predictor adverse cardiovascular events in certain types of acute coronary syndromes in the long term7) and in predicting critical limb ischemia in peripheral artery disease.8) Moreover , higher PLR values emerged as a significant index that may independently predict the severity of coronary arterosclerotic disease.9) To date, no study has evaluated the role of PLR in Asymptomatic Low EF patients. We hypothesized that PLR levels could predict the severity of coronary atherosclerosis in the setting of asymptomatic systolic HF.
Subjects and Methods
Study population
The study herein is a single-center and retrospectively designed study, consisting of 156 consecutive patients eligible for selective (CAG) between May 2013 and July 2014 in our clinic. The study was approved by the local ethics committee, and was implemented in complete concordance with the Declaration of Helsinki on human research. We selected only subjects with systolic HF that persisted with an unknown etiology after an initial non-invasive clinical assessment. Inclusion criteria were: left ventricular ejection fraction (LVEF) <40% with global left ventricular hypokinesia and age of ≥18 years.
Information including gender, age, smoking status, hyperlipidemia, hypertension (HT), and diabetes mellitus (DM) were gathered. The definition of HT appeared as a systolic blood pressure (BP) value of ≥140 mmHg and/or a diastolic BP value of ≥90 mmHg at least on >2 office BP measurements or being on an antihypertensive therapy. The definition of DM comprised a blood sugar value of ≥126 mg/dL (7.0 mmol/L) in the fasting state or being on an antidiabetic therapy whereas the status of hyperlipidemia was based on the presence of a blood cholesterol level of ≥200 mg/dL or a triglyceride level of ≥150 mg/dL in the fasting state. Smoking was defined as currently smoking or ex-smokers who forwent smoking within the past 6months.
Patients with moderate or advanced cardiac valvulopathy, malignancy, clinically decompensated congestive HF, haematological disorder, severe kidney or liver dysfunction, active infection or systemic inflammatory conditions, or autoimmune disorders and patients using steroids were excluded from the study.
Biochemical and hematological parameters
After an overnight fasting, peripheral venous blood samples were drawn from patients. Dry tubes were used for biochemical analysis, and EDTA tubes were used for hematological tests. White blood cells and erythrocyte counts, hemoglobin along with hematocrit levels were analysed by an automated hematology device Coulter Counter LH Series (Beckman Coulter Inc, Hialeah, FL, USA). The biochemical measurements were determined by an automated analyzer of biochemistry (Abbott Laboratories, Abbott Park, IL, USA).
Coronary angiography and assessment of coronary atherosclerosis severity
All patients enrolled in the study underwent selective CAG by Judkins technique through the femoral artery. The Gensini scoring system was harnessed to identify the severity of coronary artery disease.10) According to this score, 1% to 25% of stenosis in the lumen of coronary arteries is assigned a score of 1 whereas the stenoses of 26% to 50%, 51% to 75%, 76% to 90%, 91% to 99% and 100% (totally occluded) represent the scores of 2, 4, 8, 16 and 32. The score based on the stenosis degree is thereafter multiplied by a constant number in accordance with the location of lesions along the coronary arteries. A multiplication constant of 5 points is generally assigned for left main coronary artery (LMCA) lesions whereas 2.5 points are assigned for left circumflex (LCX) or proximal left anterior descending (LAD) artery lesions. Regarding LCX and LAD, lesions involving mid segments and distal segments are given the points of 1.5 and 1, respectively. The lesions involving the first obtuse marginal (OM) and diagonal branches, intermediate and posterior descending arteries (PDA) are generally multiplied with a constant of 1 point while the lesions in second OM and diagonal branches are assigned the multiplication constant of 0.5. Assessment of Gensini score was made by 2 interventional cardiologists totally blinded to the laboratory and clinical data and the coronary evaluation of the other cardiologist. In the case of disagreement, a third blinded interventionalist assessed the coronary angiograms.
According to their coronary angiograms, subjects were categorized into three groups. The first group comprised 60 patients with a normal CAG (control group). The rest was categorized into two based on their Gensini score: mildly atherosclerotic group (n=64; score of <25 points) and severely atherosclerotic group (n=32; score of ≥25 points).
Echocardiography
All echocardiographic examinations were performed by a certified cardiologist experienced in this field using a Vıvıd-7 (GE Healthcare, Horten, Norway) device in compliance with American Society of Echocardiography (ASE) guidelines.11) LVEF was calculated from apical 4-chamber views, according to a modified Simpson's rule.
Statistics
Continuous variables were defined as means and standard deviation; categorical variables were presented as percentages. The normality of distribution for continuous variables was confirmed with the Kolmogorov-Smirnov test. According to the distribution pattern of continuous variables, Mann-Whitney U test or independent-sample t-test was used for continuous variables, and the chi-square test was used for categorical variables. One-way analysis of variance (ANOVA) or Kruskal-Wallis test was used to compare 3 groups. When there was a significant difference between the three study groups, the comparison of two groups in terms of the relevant parameter was performed with post hoc tests in a one-way ANOVA and with Mann-Whitney U test after Bonferroni correction in Kruskal-Wallis test. Correlations were assessed using either Pearson's correlation test or Spearman's rank test according to the distribution pattern of the variable. Independent associations between Gensini score and independent variables were evaluated through a backward stepwise multiple linear regression analysis by comprehending all parameters showing p value of less than 0.1 on a univariate analysis. Coefficients of standardized β regression along with their significance from the multiple linear regression analysis were also reported. A receiver operating characteristic (ROC) curve analysis was used to determine the optimum cut-off level of preprocedural PLR values to predict severe coronary atherosclerosis. Statistical analyses were performed using SPSS 16.0 (SPSS Inc., Chicago, IL, USA). A two-tailed p value of <0.05 was regarded as statistically significant.
Results
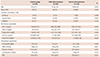
A total of 96 patients with coronary artery disease (men 69%, mean age: 61±11 years) and 60 control subjects (71.2% male, mean age: 54±13 years) with normal coronary arteries were enrolled in the study. Baseline demographic, biochemical, and hematological characteristics of the groups are outlined in Table 1. Baseline echocardiographic properties were similar in three groups and shown in Table 2.
Patients in the severe atherosclerosis group and mild atherosclerosis group were older compared to the control group. (p=0.018 and p=0.01, respectively). Fasting serum glucose ,serum creatinine, triglyceride and HDL level of three groups were similar. Serum LDL was significantly higher in the severe atherosclerosis group than controls (p<0.001); also, it was significantly higher in the mild atherosclerosis group than control group (p=0.03). In severe and mild atherosclerosis groups LDL levels were similar (168.5±6.8 vs. 176.4±10.1, p=0.51, respectively)
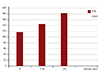
Among hematological parameters, hemoglobin levels and white blood cell count were similar between all three groups. The severe atherosclerosis group had significantly higher platelet counts compared to the mild atherosclerosis group (p<0.001) and controls (p=0.001), though platelet counts of the last two groups were similar (p=0.094). Lymphocyte count was higher in control groups than the others (1.91±0.63 vs. 1.84±0.76 and 1.78±0.70) but this is not statistically important (p=0.704). PLR was significantly higher in the severe atherosclerosis group compared to the mild atherosclerosis (p<0.001) and control groups (p<0.001) (183.5±61.6 vs. 145.2±96.5 vs. 118.4±40.4 respectively, p<0.001 for ANOVA) (Fig. 1).
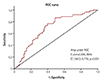
PLR was also significantly higher in patients with coronary artery disease (CAD) (n=96) compared to controls (n=60) (158±88 vs. 118±40, p<0.001). Using a cut-off level of 132, PLR predicted severe atherosclerosis with a sensitivity of 76% and specificity of 60%. The area under ROC curve was 0.695 (95% CI: 0.612-0.779, p<0.001) (Fig. 2).
Independent associations between Gensini score and independent variables were assessed by multivariate linear regression analysis by including all parameters showing a correlation with a p value of less than 0.1 on a univariate analysis (patient age, PLR and LDL). Pre-procedural PLR was independently associated with Gensini score (β=0.347, p=0.001), together with LDL (β=0.259, p=0.001), age (β=-0.180, p=0.014) (Table 3).
Discussion
The present study demonstrated that a high PLR level was independently related to the severity and extent of atherosclerotic heart disease in asymptomatic low EF patients. Patients with high pre-procedural PLR had significantly higher Gensini scores, and there was a strong link between PLR values and Gensini scores of patients with CAD. Additionally, this study showed that pre-procedural PLR >132 predicted severe atherosclerosis with a sensitivity of 76% and specificity of 60%. PLR had an independent association with Gensini score on top of high LDL levels and age as demonstrated by a multivariate analysis. This might reportedly be the first study demonstrating the link between PLR and severity of CAD in the setting of asymptomatic systolic HF.
According to the recommendations of current guidelines for chronic heart failure, cardiac catheterization should be considered in the etiological investigation of patients with left ventricular dysfunction in the presence of risk factors for coronary artery disease, angina, or refractory symptoms of heart failure.1) However demonstrate the ischemic or non ischemic etiology is important for prognosis in low EF patients. Bart et al.2) showed that ischemic etiology might still be considered as an important factor independently predicting a 5-year mortality. In a previous study for elucidation etiology in patients with left ventricle dysfunction, coronary angiography was performed and ischemic etiology was determined as 9.3%.12) Gensini score was used in our study and the detection of the severe coronary artery disease was 20% of the study group.
In a study, coronary computed tomography angiography (CCTA) was compared with invasive CAG in newly diagnosed heart failure patients in terms of detection of the severity of atherosclerotic heart disease has been determined with CCTA similar to invasive coronary angiography.13)
PLR is a new prognostic marker that gives an idea about both the aggregation and inflammation pathways. The role of leucocytes and platelets in atherosclerosis is well known.6)14) Increased platelet and low lymphocyte counts has been shown with poor cardiovascular outcomes in earlier studies.14)15)16)17) It has been shown that PLR is associated with long-term and shortterm mortality in acute coronary syndrome patients.7)18) Yildiz et al.19) showed that higher PLR was associated with poor prognosis in patients with CAD. Acar et al.20) demonstrated that high PLR is related with coronary collateral development in patients with chronic total occlusions. Sarı et al.21) revealed that pre-procedural PLR is associated with coronary atherosclerosis severity.
Oxidized LDL (atherogenic) may emerge as a trigger of endothelial dysfunction strongly associated with the atherosclerotic process. The association between the serum LDL and atherogenesis has been well established.22)23) In our study, pre procedural LDL levels also served as major factors independently predicting the severity of coronary atherosclerosis as expected.
Our study has important clinical implications; PLR which is a simple, cheap, and readily available marker can be used as a prognostic indicator to determine asymptomatic low EF patients who are at higher coronary atherosclerosis risk. In patients with elevated PLR, even if they are asymptomatic, investigation ischemia and performing coronary angiography may impact on prognosis. In patients with low PLR, noninvasive coronary imaging techniques may be recommended for coronary anatomy viewing.
Study limitations
There are several limitations regarding the present study. Sample size was small, enrolment was retrospective and it was a single center design. The amount of coronary atherosclerosis was evaluated only by a coronary angiography. We know it does not provide sufficient data about the coronary plaque burden, and shows only the lumen of coronary arteries. An intravascular ultrasound and/or coronary CT may provide necessary data about the amount of coronary atherosclerosis. We had no data on inflammation markers including C-reactive protein, tumour necrosis factor-alpha, etc. However, assessment of these substances may strengthen the study. We did not analyze other platelet indices including mean platelet volume, platelet distribution width, and inflammatory indices including neutrophil lymphocyte ratio (NLR) or correlation of these parameters with the PLR. Notwithstanding these limitations, this is reportedly the first study focusing on PLR with regard to its predictive value in asymptomatic low EF subjects, and more comprehensive studies are still warranted to corroborate our findings.
Conclusions
This is reportedly the first trial primarily focusing on the potential association between PLR and the severity of atherosclerotic heart disease in asymptomatic low EF patients. Our results indicate that harnessing the index of PLR as well as a variety of clinical variables including advanced age, DM and high LDL levels may work as valuable predictors of atherosclerotic burden, hence severity of atherosclerosis. However, the current information on this issue is still at its infancy suggesting the need for future clinical studies to validate absolute implications of this index in the setting of atherosclerotic heart disease.


 XML Download
XML Download