

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Coronary artery disease (CAD) is the most important cause of cardiovascular adverse events. Despite modern treatment, the mortality caused by CAD is still increasing.1) Diabetes, hypertension, hyperlipidemia, and smoking are risk factors of CAD that can be controlled. Genetic features are an important and unchangeable risk factor for CAD pathogenesis. Recently, studies investigating the relationship between CAD and genetic predisposition have been increasing.2)3)4) Studies showed that 40% to 60% of the risk for CAD is related to genetic predisposition.5) Until now, more than 30 genetic risk variants for CAD have been identified in genome-wide association studies (GWAS).6) Among them, association of 4 single nucleotide polymorphisms on chromosome 9p21 were found to be related to coronary atherosclerosis and myocardial infarction in different populations.7)8)
The first study describing two of these polymorphisms (rs10757274 and rs2383206) on chromosome 9p21 associated with CAD in a Canadian population.7) These findings were also confirmed in other ethnic groups from Europe, Far-East, Middle-East, and India.9)10)11)12)13) Furthermore, this relationship was independent of traditional risk factors for CAD. The single nucleotide polymorphism (SNP) on chromosome 9p21 was also associated with early onset of CAD, with a 2 fold increased risk of premature CAD.7)14) This genetic variant contributes to the risk of other atherosclerotic diseases such as aortic aneurysms and vascular dementia.15)16) However, in an African population, these associations were not detected, indicating other confounding mechanisms may alter the impact of these genetic variants on CAD development.17) The impact of the 9p21 locus on coronary artery disease severity and outcomes in patients with CAD has been studied by several researchers. However, results from these trials are contradictory.18) Thus, in the present study we aimed to investigate the impact of rs10757274 and rs2383206 polymorphisms in the chromosome 9p21 on the presence and severity of coronary atherosclerosis in a Turkish population.
Subjects and Methods
Study design
This was a single-center, prospective and cross-sectional study. Power analyses were performed using the program of G*Power Version 3.1.9.2 (HHU, Düsseldorf Universitat, Germany) power- and-sample size calculation (Düsseldorf Universität, Germany). Accordingly, (with an effective size w=0.3, α- error value of 0.05 and a power of 0.95, and critical χ2=11.070) the minimum total sample size was 220. We had an opportunity to pool blood of 703 consecutive patients who underwent coronary angiography (CAG) and 646 eligible patients were analysed. In order to increase the actual power of the study, we kept a large number of patients. Our study was conducted in accordance with the guidelines proposed in the Helsinki Declaration and approved by local ethical committee. All the patients gave informed consent before enrollment.
Study population and basal characteristics
Six hundred forty six consecutive patients who referred to coronary angiography by the indication of positive stress test or clinical highly suspicion of coronary artery disease on an outpatient clinic basis at our cardiology department had been involved in this prospective study. Exclusion criteria were unstable coronary syndromes, severe valvular diseases, decompensated heart failure, malignancy, renal or hepatic dysfunction, acute or chronic infection, hematologic and rheumatologic diseases, severe chronic obstructive lung disease. The patients who had revascularization (percutaneous coronary intervention or coronary artery bypass graft operation) history or technically inadequate coronary angiograms were also excluded because calculation of Gensini score is not possible in such cases.
Basal characteristics of the study patients were reviewed. Hypertension was defined as being under active antihypertensive treatment or documentation of blood pressure more than 140/90 mmHg. Diabetes mellitus was defined as fasting glucose level of ≥126 mg/dL and/or glucose level of ≥200 mg/dL at any time or active use of antidiabetic treatment. Smoking was defined as current smoking. The family history of coronary artery disease was accepted as positive if the patient had a first-degree relative who had myocardial infarction, sudden death, or revascularization before the age of 45 for men and 55 for women. We measured height and weight in every patient to determine body-mass index. Blood sample for analysis of blood glucose, renal function tests and lipid profile and genetic analysis had been drawn before coronary angiography. We performed coronary angiography using Judkins technique. All of the angiograms were reviewed by an independent, invasive cardiologist for the presence of CAD. The number of the coronary arteries with >50% stenosis, coronary vessel score was determined. Patients were divided into two groups with respect to coronary vessel score. Patients with vessel score>0 were included in the group of CAD (n=352) and patients with vessel score=0 were included in the control group. The severity of coronary atherosclerosis was determined by Gensini's score which considers both the extent and the severity of the lesions in a coronary angiography.19) This scoring system grades the stenosis in the epicardial coronary arteries (1 for 1-25% stenosis, 2 for 26-50% stenosis, 4 for 51-75% stenosis, 8 for 76-90% stenosis, 16 for 91-99% stenosis, and 32 for total occlusion) and multiplies this number by a constant number, which is determined according to the anatomical position of the lesion. Polymorphism-1 term was used for "rs10757274" and polymorphism -2 was used for "rs2383206". Alleles of AA, AG and GG were determined for each gene.
Genetic analysis
Genomic DNA was extracted from the peripheral blood of the study subjects using an extraction kit (Heliosis, Metis Biotechnology, Ankara, Turkey) according to the manufacturer's instructions. Two polymorphisms, named rs10757274 and rs2383206, were screened using polymerase chain reaction - restriction fragments length polymorphism method. A specific primer pair was designed for both polymorphism using Primer Premier 5 Software (Premier Biosoft International, CA, USA).
Briefly, 401 bp DNA fragment containing the region of rs10757274 polymorpism was amplified with the primers: forward 5'-GCTTCTCCCCCGTGGGTCAAATCT-3'; and reverse 5'-AATGAGGGGAGGGAGCATGTCTGT-3'. For the rs2383206 polymorphism, polymerase chain reaction (PCR). reaction was performed to amplify a 270-bp fragment with the primers: forward 5'-GGATTATTGGTGGTTTTCTAG-3'; and reverse 5'-CAAGACATAACTAATGGCTGAA-3'. Reaction conditions for these polymorphisms were as follows: initial denaturation at 94℃ for 5 min and 30 cycles of denaturation at 94℃ for 30 seconds, annealing at 62℃ for 1 min, extension at 72℃ for 1 min, and final extension at 72℃ for 5 minutes. PCR was performed using Eppendorf thermal cycler (Eppendorf, Hamburg, Germany).
After amplification, the PCR products were digested overnight with BsmAI (Fermentas, Germany ) for the rs10757274 polymorpism and AluI for the rs2383206 polymorphism. After digestion with BsmAI, 401 bp PCR product was cut into 370 and 31 bp fragments in the presence of A allele, whereas G allele was undigested. After digestion with AluI (Fermentas, Germany ), 270 bp PCR product was digested into 233 and 44 bp fragments in the presence of A allele, whereas the G allele remained undigested. DNA fragments were separated in 2% agarose gel stained with ethidium bromide, and were visualized by Gel Logic 100 Imaging System (GL 100; Kodak, Rochester, New York, NY, USA). The results were evaluated with two blind observers after image capturing.
Statistical analysis
The SPSS statistical software package (PASW Statistics for Windows, Version 18.0; SPSS Inc., Chicago, IL, USA ) was used for statistical analyses. Normality test for distribution of the continuous variables was performed using Kolmogorov-Smirnov test and histograms. Continuous variables presented as mean±standard deviation and were compared with a t-test or one-way analysis of variance and post-hoc comparisons were performed using Tukey's test. Other abnormally distributed data were presented using median with 25th and 75th percentiles and compared with Kruskal-Wallis test and the Mann Whitney U test was utilized for post-hoc pairwise comparisons. Categorical data was presented as numbers and percentages and compared using the Chi-square test (Fisher exact test, if needed). The potential confounders of CAD were first evaluated by univariate regression analysis and variables with a p of <0.1 were together recruited in a multivariate logistic regression model to find out the independent predictors of the presence of CAD. A p<0.05 was considered statistically significant.
Results
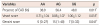
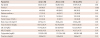
Of 646 consecutive patients, 240 female (37.2%) and 406 male (62.8%) with a mean age of 58.12±11.06 were included in the study. When the baseline characteristics of the patients were considered, 356 of them (55.1%) were hypertensive, 170 were diabetic (26.3%) 264 patients were current smokers (40.9%), and 177 patients had a positive family history of premature atherosclerotic CAD (Table 1). Laboratory findings of the patients are presented in Table 1. The distribution of the alleles was as follows; AA 12.1%, AG 42.3 %, GG 45.7% in gene-1, and AA 17%, AG 50.2%, GG 32.8% in gene-2 (Table 1). The Gensini score of the patients ranged between 0 and 202 with a median value of 9 (0-36). When the presence of the CAD between the alleles were compared in polymorphism-1, there was a significant difference between the alleles (38.9% in AA, 48.0% in GG and 56.4% in AG, p=0.017). However, there was not any difference between the alleles in polymorphism-2. The patients were divided into CAD (vessel score>0) and a control group and the baseline characteristics, laboratory findings and genetic results were presented in Table 2. According to the vessel scores, there was a significant difference between the alleles in polymorphism-1 (AA 0.71±1.04, GG 0.88±1.07, AG 1.06±1.12, p=0.018) (Fig. 1).
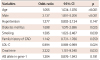
Post-hoc comparisons revealed a significant difference between the alleles of AA and AG (p=0.01). In polymorphism-2, vessel scores were comparable between the alleles. In polymorphism-1, there was a significant difference in term of CAD extent estimated by Gensini score (p=0.041). In post-hoc comparisons, there was no difference in Gensini score between AA and GG (p=0.42). A difference was evident between GG and AG (p=0.04), as well as between AA and AG (p=0.035). Gensini scores did not differ between the alleles in polymorphism-2 (p>0.05 for all). The parameters used for evaluating of presence and extent of CAD in different alleles in polymorphism-1 were presented in Table 3. There were no differences in baseline characteristics and laboratory parameters between the alleles in polymorphism-1 (Table 4). A logistic regression analysis including all the potential confounders was used to search the independent predictors of the presence of CAD (vessel score>0). Age, male sex, diabetes mellitus, smoking, LDL cholesterol and creatinine levels were found to be independent predictors of the presence of CAD (Table 5). Multivariate stepwise linear regression analysis showed that age (p<0.001), male gender (p<0.001), diabetes (p=0.002), family history of CAD (p=0.035) and serum creatinine levels (0.018) were independent factors of the extent of CAD estimated by Gensini score.
Discussion
Several studies showed that the polymorphisms located on chromosome 9p21 have different impacts on predisposition to CAD in different ethnic groups.7)9)10)11)12)13) In this study, we evaluated the importance of these polymorphisms in a Turkish population, and showed that AG allele for "rs10757274" on chromosome 9p21 locus may have a role in progression of CAD. The number of patients with CAD was higher among the group including the patients carrying this allele. Moreover, the angiographic severity of CAD was higher in patients with this allele. However, the relationship with this genetic feature and coronary atherosclerosis was not independent of traditional risk factors for CAD.
Although CAD is still the leading cause of death all over the world, a significant decrease in mortality has occurred in developed countries. This reduction in mortality is not only a result of modern therapy, but also due to effective control of cardiovascular risk factors.20) In an INTERHEART study,20) 90% of the cardiovascular mortality was found to be related with risk factors such as abnormal lipids, alcohol, smoking, hypertension, diabetes and abdominal obesity.20)21) Thus, identification of the all risk factors and their mechanisms has profound importance for the effective treatment and prevention of CAD. Now, sufficient amount of data indicates that genetic predisposition is an independent risk factor for CAD.5) GWAS have defined around 30 risk substitutes for CAD.22) These studies have demonstrated that the 9p21 locus may be characterized by an increased risk of CAD.23) 9p21 locus has been proposed to apply direct impacts on vascular wall independently other conventional risk factors and accelerate the atherosclerotic process.24) The mechanism of the 9p21 negotiates risk for CAD is still unclear. The closest genes which code proteins are the cyclin-dependent kinase inhibitors CDKN2A/2B (rs10757274) that locate about 100000 base pairs upper parts of the 9p21 locus. CDKN2A and CDKN2B play an important role in cell proliferation and they are suppressed by Polycomb proteins during cell growth and then activated during senescence.25) antisense noncoding RNA in the INK4 locus (ANRIL) (known as CDKN2BAS) has been suggested to regulate senescence at the CDKN2A gene locus and it shows a senescence-dependant role in proliferation. Inhibition of ANRIL causes decrement proliferation of human fibroblasts. Reduced expression of ANRIL was associated with atherosclerosis.26) Transforming growth factor beta (TGFβ) is a cytokine that prevents macrophage foam cell formation. TGFβ initiates the expression of the CDKN2A and CDKN2B.27) These are just two of the TGFβ responsive genes that are sited in the environs and are directly under the control of the 9p21 genetic risk locus. SNPs such as rs1333045 that inhibit TGFβ responsive factors at the 9p21 locus and this may lead to the progression of atherosclerotic process.28) These genetic features may act to accelerate progression of atherosclerosis, induce plaque rupture or thrombogenesis. Given that they are acting through an unknown mechanism, which is independent of traditional risk factors, there may be new targets waiting to be identified in the future for more efficient treatment or prevention strategies to control CAD epidemics.
Data analysis of The Wellcome Trust-Case Control Consortium study and German Myocardial Infarction Family Study has detected supplemental loci at 9p21, 6q25.1and 2q36.3 as loci for risk augmentation for CAD with the main SNPs; existing rs1333049, rs6922269, and rs2943634 respectively.9) Similar relationships with SNPs and 9p21 locus has been shown in Canadians (rs10757274, rs2383206), Icelanders (rs1333040, rs23833207, rs10116277 and rs10757278).7)8) Munir et al.18) displayed a relation of 9p21-3 allele with an increased risk of triple vessel disease and severity of atherosclerosis burden measured with the Gensini score in a meta-analysis.
In a very recent study performed by Çakmak et al.,29) the two SNPs of rs2383207 and rs1333049 at the 9p21 chromosome were evaluated in 220 patients with CAD in a Turkish population. Significant differences were seen in frequencies of rs2383207 and rs1333049 variants between CAD patients and healthy subjects. Also, for the two SNPs, the risk genotypes AA and GG were related with an increased risk of CAD. Furthermore, AA genotype was an independent predictor of CAD. Although our study population was similar in terms of race and ethnicity, there are important differences between the two studies. We investigated different SNPs (rs10757274 and rs2383206 polymorphisms) on the same chromosome of 9p21. Our study population was wider and patient selection showed important discrepancies between the two studies. Çakmak et al.29) did not include patients older than 55 years in male -and 65 years in female patients. However, these gene polymorphisms are particularly expected to be related with premature atherosclerosis. Additionally, they accepted patients having a coronary lesion less than 70% as control subjects. Because CAG is a luminographic method many patients might have been under-diagnosed when calculating the vessel score. Finally, they have not mentioned if patients with coronary stents and/or coronary grafts were excluded from the study. This is important since the Gensini score cannot be calculated in such patients. When our study considered the rs10757274 polymorphism, the risk genotype of AG was related with an increased number of vessel score. However, none of the alleles were independent predictors of either presence or extent of CAD. This result can be explained by complex interaction between all confounders for development and progression of CAD.
In contrast to previous studies indicating an independent relationship between polymorphisms on 9p21 gene and CAD, our findings showed that the relationship was associated with traditional risk factors. Thus, these polymorphisms may also be associated with risk factors affecting CAD development such as hypertension, diabetes or hyperlipidemia and may potentiate or accelerate their adverse effects on the coronary vessel wall. So, they may exert their effect through accelerating progression of atherosclerosis. This theory could also explain the relationship between these polymorphisms and premature onset-CAD. Coronary artery disease is also the leading cause of death in Turkish population and the mean age for CAD is relative younger compared to other populations.30) In addition, the finding of increased angiographic severity of CAD, which is determined by Gensini score in our study, also supports this theory. Further studies on larger populations are required to clarify these mechanisms. LDL cholesterol level was lower in CAD group compared to control group. This result was driven by higher use of statins in the CAD group. In the CAD group, patients with a prior diagnosis of CAD had, as expected, hypertension, diabetes, smoking, male gender and elderly patients were more common, all of which were associated with higher CAD risk score and more extent use of statins.
The main limitations of our study are the cross-sectional nature and relatively small number of the study population. Second, it was a single-center study. Third, we investigated only two SNPs though there are many remarkable SNPs associated with CAD. Although the present study was not designed to show the pathophysiological mechanisms which are responsible for the adverse effects of these genetic polymorphisms, the findings of an increase in the Gensini score with an AG allele for gene-1 and the dependence on traditional risk factors indicate that the mechanism of action may accelerate and/or facilitate coronary atherosclerosis. Our study paves the way for performing larger studies on this issue.
In conclusion, our findings showed that the presence of polymorphism, including AG allele on chromosome 9p21, was related to CAD in a Turkish population. Although this relationship was not independent of other cardiovascular risk factors, this genetic feature may potentiate or accelerate their adverse effects on cardiovascular system. This relationship may explain the high mortality and morbidity caused by CAD in this Turkish population.



 XML Download
XML Download