

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Patent foramen ovale (PFO) is the persistence of the normal fetal communication between the right and left atria. It is a common benign condition; up to 27% of the population has PFO.1) But under certain hemodynamic circumstances, PFOs can open and act as a conduit for thrombi to pass from the systemic venous circulation to the systemic arterial circulation, predisposing to stroke and paradoxical embolism.2) Herein, we describe a new method in device closure of PFO, introduction of delivery sheath over coronary sinus catheter into the left atrium in a challenging case.
Case
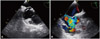
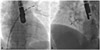
A 34-year-old female with cryptogenic stroke was admitted to our hospital. On a physical examination, she had left paraplegia. Her electrocardiography was in sinus rhythm. Transthoracic echocardiography was normal, except interatrial septal aneurysm. Thus, transeosaphageal echocardiography was performed, which revealed interatrial septal aneurysm and PFO (Fig. 1). Hence, percutaneous closure of PFO, under general anesthesia with the guidance of transesophageal echocardiography (TEE), was planned. A 7 Fr sheath was introduced through the right femoral vein, and 80 U/kg of unfractioned heparin was administered, intravenously. PFO was attempted to cross unsuccessfully with multipurpose, right Judkins, and right Amplatz diagnostic catheters. After a right atrium angiography, we crossed PFO with coronary sinus catheter to assess the reference entry point, and then another 7 Fr catheter was inserted to the left femoral vein and tried to cross PFO with Multipurpose, right Judkins and Amplatz diagnostic catheters over normal and hydrophilic guide wires under the guidance of coronary sinus catheter, but could not passed through PFO. Thus, we pulled the catheters and inserted 9 Fr delivery sheath from the left femoral vein, then inserted 7 Fr coronary sinus catheter through the delivery sheath and crossed PFO with coronary sinus catheter (Figs. 1A and 2A), and deployed the delivery sheath over coronary sinus catheter into the left atrium, and pulled back the coronary sinus catheter and inserted the Amplatzer PFO occluder through the delivery sheath, successfully deploying the occluder (Figs. 1B and 2B). The patient was discharged uneventfully with aspirin 100 mg and clopidogrel 75 mg per/day medication.
Discussion
Patent foramen ovale closure is performed in a standard catheterization laboratory, under physiological monitoring and fluoroscopic guidance. TEE examination is complementary for optimal results.3) General anesthesia is required for TEE guided procedures. Procedure was performed through the femoral venous access, and intravenous unfractioned heparin 80-100 U/kg was administered. The multipurpose diagnostic catheter is commonly used to cross PFO, but in unsuccessful cases, the right Judkins and Amplatz diagnostic catheters may be used. Right atrial angiography may be performed in challenging cases to understand the atrial anatomy. PFO is frequently crossed with coronary sinus catheter and radiofrequency ablation catheters, during electrophysiological studies. In laboratories that are familiar with electrophysiology procedures, coronary sinus catheter may be used for the localization of PFO; furthermore, it may be used for crossing PFO in order to deploy the delivery sheath into left atrium, for saving time in prolonged cases, in different atrial anatomy and when usage of classical maneuvers and catheters are unsuccessful.
Moreover, blade septostomy may also be used when classical methods failed, but it is associated with major complications, including cardiac perforation, vascular injury and conduction disturbances. But crossing the PFO, with coronary sinus catheter, is safely used electrophysiology procedures.
In conclusion, this promising method, deploying the delivery sheath over coronary sinus catheter, may be used easily and safely when routine maneuvers fail.
 XML Download
XML Download