

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Uterine clear cell carcinoma (UCCC) is an uncommon variant of carcinoma of the uterus that represents only about 1%–6% of all endometrial carcinomas [123456]. UCCC behaves aggressively with a high propensity towards extra-uterine spread [78]. Up to 40%–50% of patients with disease clinically confined to the uterus may present with extra-uterine disease, even in the absence of myometrial invasion (MMI) [79]. The recurrence rate of UCCC has been reported to be 14% in early-stage, and 56% in advanced-stage disease, respectively [10]. Given the rarity of UCCC, optimal surgical and postoperative management remains undefined [11]. Randomized trials are either too difficult or even impossible to conduct because of the small number of women who are affected [12].
Non-invasive UCCC (UCCC with no MMI) is an uncommon finding that necessitates particular care because of the rarity of the disease, and limited available published data. Given the limited extent of the disease but its aggressive biologic behavior, it is unclear whether adjuvant therapy is warranted in this clinical setting [101112]. Therefore, we focused on combining multi-institutional data sets of women with non-invasive UCCC.
The objective of this retrospective study was to assess the prognosis of surgically-staged patients with non-invasive UCCC and to determine the role of adjuvant therapy.
MATERIALS AND METHODS
The medical records of patients that underwent primary treatment for UCCC from January 1997 to November 2016 at 8 Gynecologic Oncology Centers in Turkey were retrospectively reviewed. The study protocol was approved by the Local Institutional Review Board. All patients provided an informed consent regarding research use of their medical information. The inclusion criterion was post-operative pathology-proven non-invasive UCCC (of pure or mixed histology). We excluded women that had any synchronous malignancy, incomplete medical records, incomplete surgical staging and a lack of follow-up. “Incomplete medical records” referred to the medical records which lacked more than 5 variables among those would be investigated whereas “incomplete surgical staging” defined patients who had no lymphadenectomy. Women with “a lack of follow-up” were those who decided to continue their treatment at other facilities following surgery. Since no survival data were available about the outcome of these patients, they were excluded from the study.
The preoperative diagnostic procedure was endometrial sampling or dilatation and curettage (D&C). No patient had hysteroscopy for diagnostic purposes in the preoperative period. The staging criteria were determined postoperatively and were based on the 2009 International Federation of Gynecology and Obstetrics (FIGO) staging system [13]. To qualify as mixed UCCC, the clear cell histology had to comprise more than 50% of the tumor [9].
The original pathology reports of 232 women that underwent surgical treatment for UCCC were analyzed. Pathological specimens were examined by gynecologic pathologists at each institution. Non-invasive UCCC was defined as the disease without MMI in the surgical specimen after the examination of permanent sections. Surgical staging consisted of total hysterectomy, bilateral salpingo-oophorectomy, pelvic and para-aortic lymphadenectomy, peritoneal washings, omentectomy, peritoneal biopsies and tumor cytoreduction, if required. Surgery was performed by gynecologic oncologists at each participating institution. A systematic lymph node dissection (LND) was arbitrarily defined as the removal of more than 20 nodes [14].
Patient data were collected from review of medical records including clinic notes, operation reports, pathology, and imaging reports. The clinical and pathological characteristics of patients were recorded, including age, preoperative serum CA125 level, presence of lymphovascular space invasion (LVSI), number of total lymph nodes (LNs) removed, number of pelvic and para-aortic LNs removed, peritoneal cytology, number of metastatic pelvic LNs (if applicable), number of metastatic para-aortic LNs (if applicable), requirement for adjuvant therapy, type of chemotherapeutic regimen, number of cycles, adjuvant radiation therapy, length of follow-up, recurrence, and survival.
The clinical follow-up assessment of the disease consisted of pelvic and physical examinations, serum CA125 measurements and imaging studies when clinically indicated. Follow-up visits were scheduled every 3 months during the first 2 years, every 6 months until 5 years, and annually thereafter. The survival status of the patients was determined as dead or alive at the time of the last follow-up.
The decision to administer adjuvant radiotherapy, chemotherapy or a combination of both was based on medical comorbidities, and the institutional practices at that time. Recurrence was defined as documentation of metastasis either by biopsy or imaging techniques after a disease-free survival (DFS) ≥3 months. The treatment of recurrent disease included cytoreductive surgery and/or chemotherapy, and/or radiotherapy, if applicable. After treatment for relapse, patients were again evaluated every 3 months for the first 2 years and every 6 months thereafter.
Statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) software (version 22; SPSS Inc., Chicago, IL, USA). The data was expressed as median and range for continuous variables. Binary variables were reported as counts and percentages. Categorical variables were evaluated using the χ2 test or Fisher's Exact test as appropriate for the group size. DFS was calculated from the time of diagnosis to the time of disease recurrence, death or last follow-up. Overall survival (OS) was calculated as the time period between initial diagnosis of UCCC to the date of death or the last contact. Disease-specific survival (DSS) was calculated as the time period from initial diagnosis until the date of disease-related death or the last follow-up. Survival curves were generated using the Kaplan-Meier method, and the differences between survival curves were calculated using the log-rank test. In order to evaluate the prognostic factors for DFS and OS, a Cox-regression model was used. A p-value <0.05 was considered to indicate statistical significance.
RESULTS
During the study period, a total of 7,495 women with uterine corpus cancer were treated at the 8 participating centers. Of these women, 232 (3.1%) had pathologically confirmed UCCC, and 64 patients with non-invasive UCCC were identified out of those 232 women. Non-invasive UCCC represented 27.5% of all UCCCs during the study period. We excluded 5 patients with incomplete surgical staging (patients with no lymphadenectomy) as well as women that had any synchronous malignancy (n=1), incomplete medical records (n=2), and a lack of follow-up (n=3). A total of 53 patients were included in the final analysis (Fig. 1). Profile of patients including their tumor characteristics is shown in Table 1.

Table 1
Baseline characteristics of all patients
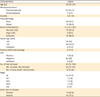
Values are presented as median (range) or number (%).
LN, lymph node; LVSI, lymphovascular space invasion.
![]()
The median age of the patients was 63 years (range: 42–84 years), and median duration of follow-up was 43 months (range: 1–171 months). All patients but 4 received systematic LND. Total number of LNs removed for the patients that underwent non-systematic LND was 15, 16, 17, and 15, respectively. The rate of achieving systematic LND was 92.4%. The median number of LNs removed was 40 (range: 14–100). The median number of pelvic and para-aortic LNs removed were 26 (range: 10–65), and 12 (range: 2–43), respectively.
One patient (1.9%) with non-invasive UCCC was defined as “vanishing endometrial cancer” at the end of the pathologic examination. Thirty-eight cases (71.7%) were designated as pure clear cell carcinoma whereas 15 cases (28.3%) had mixed tumors. Peritoneal cytology was positive in 6 patients (11.3%). There were 7 patients (13.2%) with LVSI whereas the presence of LVSI was unknown in 2 patients. LN metastasis was detected in 3 patients (5.6%) (1 patient with pelvic LN involvement, 1 patient with para-aortic LN involvement, and 1 patient with pelvic and para-aortic LN involvement). Preoperative serum CA125 level was found to be elevated in 8 patients (20.5%). However, preoperative serum CA125 was not obtained in 14 patients.
In the entire cohort, the number of total recurrences was 8 (15.1%). At the time of analysis, 9 patients had died with 7 deaths due to UCCC whereas 2 women were dead of intercurrent disease. With a median follow-up 43 months, the 2- and 5-year OS rate was 89% and 73.5%, respectively. The 2- and 5-year DFS rate for the entire cohort was 88% and 75.2%, respectively. DSS was also calculated. The 2- and 5-year DSS rate was 89.8% and 80.1%, respectively. When the OS rates of the patients with pure and mixed UCCC were compared, the 2- and 5-year OS rates were found to be similar (88.5% vs. 91% and 67% vs. 91%, p=0.230).
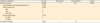
Of 53 women with non-invasive UCCC, 12 women (22.6%) had disease beyond the uterine corpus at the end of comprehensive surgical staging. Of those, 1 had stage IIIA, 1 had stage IIIC1, 1 had stage IIIC2, and 9 had stage IVB disease. Of the 9 women with stage IVB disease, 5 had isolated omental involvement (4 macroscopic, 1 microscopic), whereas 4 had omental metastases in addition to the involvement of other organs such as the appendix, uterine tubes, rectosigmoid colon, and pelvic peritoneum. Preoperative serum CA125 level was elevated in 5 women (55.5%) in this group while there were no data about preoperative serum CA125 levels in 3 women. Clinical and pathological characteristics and outcome of patients with the extra-uterine disease are shown in Table 2. For women with the extra-uterine disease, median survival time was 56 months (95% confidence interval [CI]=18.9–93.07; standard error [SE]=18.91), whereas 5-year OS rate was only 29.2%. For this subgroup of women with the extra-uterine disease, median DFS was 15 months (95% CI=0–54; SE=19.9) and 5-year DFS rate was 31.3%.
Table 2
Clinical and pathological characteristics and outcome of patients with extra-uterine disease

ANED, alive with no evidence of disease; AWD, alive with disease; CRT, chemoradiotherapy; CT, chemotherapy; DOD, dead of disease; DOID, dead of intercurrent disease; EBRT, external beam radiotherapy; LN, lymph node; LVSI, lymphovascular space invasion.
*Paclitaxel and platinum+EBRT; †Paclitaxel and platinum; ‡This patient did not have adjuvant treatment because of poor performance status and medical comorbities. She died of myocardial infarction 1 month after surgery.
![]()
Forty-one women (73.3%) had no extra-uterine disease, and UCCC limited to the endometrium was confirmed after comprehensive surgical staging. The rate of UCCC limited to the endometrium was 17.6% among all UCCCs during the study period. Of those, 13 women (32%) were observed without adjuvant treatment whereas 28 patients (68%) underwent adjuvant therapy. Adjuvant treatment modalities for women with UCCC limited to the endometrium are presented in Table 3. Only 1 patient out of the 13 that did not receive adjuvant treatment had a recurrence on the 38th month after initial diagnosis. The patient recurred in the liver, and she was treated with systemic chemotherapy. She was dead of disease 46 months after initial diagnosis. However, there was no significant difference in terms of DFS between women with and without adjuvant therapy. The 2-year and 5-year DFS rate for patients with and without adjuvant treatment was 100.0% vs. 100.0% and 100.0% vs. 74.1%, respectively (p=0.060). Women that received adjuvant therapy seemed to have an OS advantage at 5 years when compared to the women that did not undergo adjuvant therapy (100.0% vs. 71.4%; p=0.045) (Fig. 2). For 41 women with disease limited to the endometrium, 5-year DFS and OS rate was 95.7% and 90.0%, respectively.
Table 3
Adjuvant treatment modalities and DFS for women with UCCC limited to the endometrium
BRT, brachytherapy; CT, chemotherapy; DFS, disease-free survival; EBRT, external beam radiotherapy; UCCC, uterine clear cell carcinoma.
![]()
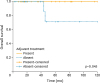 | Fig. 2OS analysis in women without extra-uterine disease (n=41) with regard to adjuvant therapy.
OS, overall survival.
|
Of the risk factors analyzed for the presence of extra-uterine spread in women with non-invasive UCCC, elevated preoperative serum CA125 level was found to be a significant predictor (odds ratio [OR]=11.9; 95% CI=1.18–121.30; p=0.036) (Table 4).
Table 4
Univariate and multivariate analyses of risk factors for extra-uterine disease in non-invasive UCCC
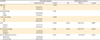
CI, confidence interval; LVSI, lymphovascular space invasion; OR, odds ratio; UCCC, uterine clear cell carcinoma.
![]()
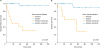
Univariate analysis revealed positive peritoneal cytology, LN involvement and extra-uterine disease as significant factors for both OS and DFS (Table 5). While no significant factor for OS was found in multivariate analysis, positive peritoneal cytology (hazard ratio [HR]=10.8; 95% CI=1.3–90.1; p=0.027) and extra-uterine disease (HR=9.1; 95% CI=1.52–54.71; p=0.016) were found to be independent risk factors for DFS (Figs. 3 and 4).
Table 5
Univariate and multivariate analyses of all patients for DFS
CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; LN, lymph node; LVSI, lymphovascular space invasion.
![]()

DISCUSSION
This is one of the largest series that reported the results of surgically-staged non-invasive UCCC. We reported on the management of 53 patients with non-invasive UCCC who were surgically staged, among these 41 had disease confined thoroughly to the endometrium.
In the current study, histologically proven UCCC confined to the endometrium represented 17.6% of all UCCCs during the study period with a 5-year OS rate of 90%. In the study by Thomas et al. [11], 16.1% of women with surgically-staged UCCC have been reported to have no MMI with a 5-year OS rate of 78%. Creasman et al. [8] reported that 15% of patients with UCCC had no MMI with a 5-year OS rate of 83%. The prevalence of non-invasive UCCC has been reported to be 14%–16% in previous studies [610]. However, Abeler and Kjørstad [5] reported that 90% of women with no MMI survived 5 years. Our findings associated with the prevalence of the disease and 5-year OS rate are comparable with previous reports.
Since UCCC has a poor survival presumably due to the early metastatic occurrence, it is important to evaluate these lesions in light of those who are surgically staged [8]. Cirisano et al. [7] showed that up to 40% patients with UCCC clinically confined to the uterus had extra-uterine spread, even in patients without deep MMI. Our study revealed that extra-uterine disease might occur in 22.6% of patients with no MMI, including a 5.6% rate of lymphatic dissemination.
The omentum appeared as the most common metastatic site in women with non-invasive UCCC in our study. On the contrary, Thomas et al. [11] reported that no patient was upstaged on the basis of omentectomy or peritoneal biopsies in a series of 99 UCCC patients. The authors characterized omentectomy as a surgical procedure that may not be necessary and suggested close inspection of the omentum and all peritoneal surfaces including the bowel and mesentery in order to exclude occult peritoneal disease [11]. However, Saygili et al. [15] found omental metastasis in 6% of patients with apparent stage I endometrial cancer. The omental involvement was occult (micrometastasis) in most of these cases. Overall, only 5% of their patients had clear cell histology; however, among patients with omental metastasis, 33% were from the clear cell histology group [15]. We found out the rate of omental involvement as 17% in women with non-invasive UCCC. On the basis of our findings, we strongly recommend omentectomy to be a routine component of surgical staging for UCCC, even in women with no MMI.
The most important reason for the poor prognosis of UCCC is the fact that UCCC has a propensity for spreading outside the uterus, early in the disease process [8]. Prior studies have shown that up to 17%–20% of patients that were presumed to have early-stage UCCC were found to have nodal metastasis at the end of complete surgical staging [111617]. In our study, the rate of nodal involvement was 5.6% for women with non-invasive UCCC, including 2 women with isolated LN metastases. Mahdi et al. [17] reported that the number of LNs removed had a significant impact on the 5-year survival rates that persisted in patients with early-stage UCCC who have negative LNs. It should be reminded that the rate of achieving systematic LND was 92.4% in our study, leading to a 5-year OS rate of 90% in women with UCCC truly confined to the endometrium.
For women with UCCC truly confined to the endometrium, there was no significant difference in terms of DFS between women with and without adjuvant therapy in the current study. Although we showed that women who underwent adjuvant therapy seemed to have an OS advantage at 5 years when compared to women that did not undergo adjuvant therapy, this finding might have been biased by the death of a woman with no adjuvant treatment because of an intercurrent myocardial infarction. In our series, only 1 woman (7.7%) with no adjuvant treatment had a hematogenous failure in the liver leading to death 8 months after recurrence. Primary tumor diameter of this patient was 5 mm, whereas histology was pure clear cell carcinoma. Peritoneal cytology and LVSI were negative for this patient.
In the study by Thomas et al. [11], 50% of the women with early-stage disease (confined to the uterus) were managed without adjuvant therapy and received close surveillance only, and only 1 patient developed vaginal recurrence. They concluded that systemic chemotherapy was not necessary for patients with surgically-staged stage I/II UCCC whereas they suggested that vaginal brachytherapy alone appeared to be an adequate treatment for women with stage I UCCC confirmed by systematic LND [11]. However, they had no specific recommendations about adjuvant therapy for women with UCCC confined to the endometrium [11].
Nguyen et al. [10] reported that adjuvant treatment may not be needed in stage I UCCC confirmed with surgical staging, particularly for those with lower risk factors such as superficial MMI and no LVSI. Maggino et al. [18] suggested that both chemotherapy and radiotherapy might be unnecessary in patients with stage IA and IB, in their cohort of 65 women with UCCC. They demonstrated excellent prognosis for completely staged patients with stage IA and IB disease treated without adjuvant therapy [18]. Kim et al. [19] reported similar 5-year OS rates for women with and without adjuvant radiation therapy with stage IA UCCC. The 2017 National Comprehensive Cancer Network (NCCN) guidelines state that observation after surgery is an option for patients with “no residual disease” in the hysterectomy specimen in patients with FIGO stage IA disease with no MMI [20].
Although no significant difference in terms of DFS was observed in patients with and without adjuvant therapy, there seemed to be a trend in favor of adjuvant treatment in women with non-invasive UCCC in the current study. However, it should be reminded that the number of women that did not receive adjuvant therapy was only 13 in our study. Our findings suggest that observation might be proposed as a reasonable option for women with UCCC limited to the endometrium confirmed by complete surgical staging. However, it is obvious that a definitive conclusion about this issue cannot be drawn from these retrospective data we presented.
In the current study, positive peritoneal cytology and extra-uterine disease were found to be independent risk factors for DFS in non-invasive UCCC. Although positive peritoneal cytology was excluded from 2009 FIGO staging for endometrial cancer [13], its prognostic value in women with UCCC is unknown. Combining multi-institutional data sets of women with UCCC is essential to study the prognostic impact of peritoneal cytology [21].
Non-invasive UCCC has rarely been studied. The existing reports on UCCC are restrictive and conflicting because of sample size, inclusion criteria, treatment variability (lack of surgical staging, adjuvant therapy), definitions, and assignment of histologic subtype (pure vs. mixed) or a combination of these factors [22]. In the current study, we only included women with histologically proven non-invasive UCCC if the patients had comprehensive surgical staging and if the clear cell component was more than 50% after pathological analysis. In conclusion, our study is one of the largest retrospective cohorts of non-invasive UCCC.
Limitations of our study include the lack of comprehensive central pathology review, its multicentric and retrospective nature as well as the variation in decision-making and patient selection for adjuvant treatment modalities. Data interpretation is constrained by variation in institutional practices. We culled patients from 8 Gynecologic Cancer Centers; the study period was long during which some minor and major changes occurred associated with surgical techniques and adjuvant treatment modalities. Therefore, possibly analyzing clinical outcomes among patients with and without adjuvant treatment may not be equally balanced and objectively represented. In addition, various adjuvant treatment modalities might have affected the validity of the outcome. However, given the low rate of UCCC, the study design used here was necessary to achieve a satisfactory sample size. Although a comprehensive central pathology review would be ideal, patients with UCCC included in this study do reflect the “real world” diagnosis and practice in Turkey. However, it should be emphasized that all pathologic specimens were interpreted by experienced gynecologic pathologists at each institution participated in the current study. Despite the above limitations, our study contributes to the limited body of knowledge on this topic.
Our findings have important clinical implications. First, our data demonstrate that extra-uterine disease may occur in the absence of MMI in women with UCCC. A high rate of upstaging (22.6%) has been shown after complete surgical staging. This finding highlights the importance of complete surgical staging in this setting. DFS is significantly associated with positive peritoneal cytology and extra-uterine disease. Second, the omentum appears to be the most common metastatic site in women with non-invasive UCCC. Therefore, omentectomy should be a routine component of surgical staging in UCCC, even for women with no MMI. Third, observation might be proposed as a reasonable option for UCCC patients with disease truly confined to the endometrium. However, this finding should be validated in further studies involving the larger number of patients.
 XML Download
XML Download