

 PDF
PDF Citation
Citation Print
Print



introduction
Although the vast majority of human papillomavirus (HPV) genotypes causes benign warts of the skin or genital region, infection by some HPV genotypes can lead to the development of malignancy, mainly cervical cancer. Besides, 43% of vulvar and 70% of vaginal cancers are attributable to HPV [1]. Fifteen HPV types are considered carcinogenic or high-risk (HR): 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 73, and 82. Three other HPV types are considered probably carcinogenic or probably high-risk (pHR): 26, 53, and 66. Twelve HPV types are classified as low-risk (LR) types: 6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81, and CP6108 [2]. Elucidation of the role of HPV in cervical cancer pathogenesis has led to the incorporation of HPV testing into (primary) screening strategies. Several strategies have been suggested for early detection of cervical cancer, using cervical cytology and/or molecular tests for HPV detection in cervical smears. The current Belgian screening program is cytology-based, with molecular detection of oncogenic HPV only in case of atypical squamous cells of undetermined significance (ASC-US) or follow-up samples of women previously treated for high-grade lesions. In contrast, co-testing (simultaneous HPV testing and cervical cytology) has become the predominant method of screening for instance in the United States and HPV testing is introduced as the primary screening test in organized screening programs for instance in The Netherlands [3]. Whilst cytology-based screening programs rely on clinician-collected cervical samples, vaginal (self-) collection is likely to become an integral part of screening, as HPV testing gradually gains ground. This is because the success of screening depends highly on the participation of the target population, and screening programs requiring pelvic examination may pose a barrier. Indeed, women who are not or infrequently screened are known to be at highest risk of developing cervical cancer [3]. Incorporation of non-invasive (self-) sampling methods, e.g., vaginal sampling, might increase the acceptance of testing and optimize screening coverage. However, the clinical validity of vaginal swabs has not yet been well established. The presented work explores the interchangeability of vaginal swabs and cervical smears for HPV testing, by means of a prospective study conducted in 303 female sex workers (FSWs) in Belgium. Furthermore, we report on the occurrence of 32 different HPV genotypes in paired vaginal swabs and cervical smears from 54 FSWs with low-grade squamous intraepithelial lesion (LSIL) or high-grade squamous intraepithelial lesion (HSIL).
MATERIALS AND METHODS
The study was approved by the Ethical Committee of the Ghent University Hospital with Belgian registration number, B670201524867.
The study was conducted in 303 FSWs embedded in a health program for sex workers in Flanders (Pasop vzw, Ghent, Belgium), between June 2015 and June 2016. Pasop vzw was founded in 1990 and provides sex work specific occupational health services focused on prevention and outreach, complementary to existing care. The Pasop vzw team consists of 2 general health practitioners, assisted by nurses and social workers. Pasop vzw offers sexually transmitted infection (STI) screening, vaccination against hepatitis B, contraceptive counseling, sex education, and psychological assistance. STI screening is indicated at first contact between the Pasop vzw team and the sex worker, as well as after perceived risk (e.g., condom failure) or when signs or symptoms of STI are present. Women eligible for STI screening were consecutively informed on our study by a physician and invited to participate, after documenting the informed consent. The studied population does not lend itself for longitudinal follow-up, as it consists of anonymized individuals who switch workplace and residence on a regular basis. Therefore, FSW were included consecutively during the selected time frame.
A vaginal Abbott swab (VA) (Abbott Laboratories, Abbott Park, IL, USA) and a ThinPrep cervical smear (CS) (Hologic Inc., Bedford, MA, USA) were sampled consecutively by a physician. Vaginal swabs, sampled halfway the vagina, were taken prior to the cervical samples, in order to avoid potential dilution by the lubricant used during pelvic examination [45]. All samples were sent to the Department of Laboratory Medicine of the Ghent University Hospital at room temperature within a 24-hour timeframe. Immediately after arrival, the VA samples were stored at −20°C and tested for HPV within 1 week, using 600 µL of sample for Abbott RealTime High Risk HPV assay on the Abbott m2000sp/rt systems (Abbott Laboratories). This test is intended to detect 14 HR-HPV genotypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) and to partially genotype 16 and 18 from the other HR genotypes. Each signal is either determined as “Detected” if the cycle number (CN) is less than a fixed assay cutoff cycle or is determined as “Not Detected” if the CN is not generated or if the CN is greater than or equal to the assay cutoff cycle, which applies only to cervical smears. The package insert mentions that the assay tracks HPV genotypes at a variable limit of detection: 5,000 copies/mL for HPV 16, 18, 35, 39, 45, 51, 59, 66, and 68; 20,000 copies/mL for HPV 31, 33, 52, and 56; and 50,000 copies/mL for HPV 58.
The CS samples were first subjected to cervical cytology investigation at the Department of Pathology of the Ghent University Hospital, using the Bethesda system: negative for intraepithelial lesions or malignancy (NILM); ASC-US; LSIL or HSIL. All smears were screened by a cytologist and supervised by a pathologist in case of any suspected abnormality. In case of HSIL, second reading by senior pathologist was performed. Afterwards, samples were sent to the Department of Laboratory Medicine and stored at −20°C, prior to HPV testing.
In case of LSIL or HSIL abnormity, both VA and CS samples were genotyped using INNO-LiPa HPV Genotyping Extra II (Fujirebio, Ghent, Belgium) following the manufacturer's instructions. This process consist of a multiplex polymerase chain reaction (PCR)-based assay targeting the HPV L1 gene, starting from the DNA extracts generated by the Abbott m2000sp system (Abbott Laboratories), followed by reversed line blot hybridization using the Autoblot 3000H tray (Fujirebio). The assay detects 32 different HPV genotypes: 13 HR-HPV genotypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68); 6 pHR-HPV genotypes (26, 53, 66, 70, 73, and 82); 9 LR-HPV genotypes (6, 11, 40, 42, 43, 44, 54, 61, and 81) and 4 genotypes with unknown significance (unknown risk [UR]-HPV]) (62, 67, 83, and 89). All tests were read manually by 2 independent readers. In case of disagreement, the results were read by a third reader. The INNO-LiPa results were compared between paired VA and CS samples in order to assess the usefulness of vaginal samples for HPV testing. Besides, the results of INNO-LiPa were compared with the results of Abbott, allowing analysis of the importance of the pHR-HPV genotypes not included in the Abbott assay. Results were analyzed statistically using MedCalc software v15.6.1 (MedCalc Software, Mariakerke, Belgium). The difference in prevalence between paired samples was calculated using the McNemar test. The level of agreement between paired samples for each HPV genotype and for each HPV risk group was calculated using the kappa inter rater agreement (<0.20, poor agreement; 0.21–0.40, fair agreement; 0.41–0.60, moderate agreement; 0.61–0.80, good agreement; and >0.81, very good agreement) [6]. The difference in mean number of genotypes in paired samples was calculated using the paired samples t-test.
RESULTS
Within the selected time frame, 303 FSWs participated. The results from 11/303 FSWs were excluded because the vaginal sample contained inadequate volume. The baseline prevalence for HR-HPV was calculated by categorizing each FSW as infected when at least 1 out of 2 samples was positive for the Abbott HR-HPV test. Fifteen FSWs were included twice, of which 8 tested positive on both occasions with intervals of 1 to 7 months. Given the persistent nature of HPV infections, all duplicates were calculated as one episode, resulting in a prevalence rate for HR-HPV of 51% (144/284).
Overall, cervical cytology showed 56% NILM, 26% ASC-US, 12% LSIL, and 6% HSIL. In case of HSIL or LSIL, there was a preponderance of HR-HPV positivity, as shown in Fig. 1. One FSW with HSIL cervical cytology had a negative result on Abbott HR-HPV testing. Genotyping using INNO-LiPa, however, revealed the presence of HPV 67. This genotype is considered to be of UR, but is gaining interest as it appears to be more prevalent in vaccinated women [7].
 | Fig. 1Flowchart of inclusion of FSWs and number of positive results for HR-HPV on CS in function of the result of cervical cytology.
ASC-US, atypical squamous cells of undetermined significance; CS, ThinPrep cervical smear; FSW, female sex worker; HPV, human papillomavirus; HR, high-risk; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion; NILM, negative for intraepithelial lesions or malignancy; +, positive; −, negative.
*Significantly higher positivity rate than NILM (p=0.001); †Significantly higher positivity rate than ASC-US (p<0.001); ‡Significantly higher positivity rate than NILM (p=0.019); §Significantly higher positivity rate than ASC-US (p=0.001).
|
Comparison of the Abbott HR-HPV results on paired VA/CS samples revealed that HR-HPV was detected more frequently in vaginal swabs (137/284 [48.2%]) than in cervical smears (118/284 [41.5%]) (p=0.005). This finding necessitated further genotyping by INNO-LiPa, in order to thoroughly compare the occurrence of different HPV genotypes, rather than to compare only the presence or absence of HR-HPV. For this analysis, we made a sub-selection of the 54 FSWs with HSIL or LSIL cervical cytology results, because those groups have the highest clinical relevance and showed preponderance of HR-HPV positivity (Fig. 1). In this subpopulation, 2/54 FSWs were excluded due to sample shortage, leaving 104 samples from 52 FSWs to be processed. Analysis of the occurrence of the 32 different HPV genotypes included in the INNO-LiPa assay revealed an overall prevalence of 98% (51/52) for any HPV genotype; 87% (45/52) for HR-HPV; 44% (23/52) for pHR-HPV; 54% (28/52) for LR-HPV; and 33% (17/52) for UR-HPV (Table 1). The 1 FSW with a fully negative genotyping analysis had LSIL cervical cytology. The difference in prevalence between paired samples was significant only for UR-HPV: 31% (16/52) in VA compared to 17% (9/52) in CS (p=0.040).
Table 1
HPV types identified in paired VA and CS samples collected from 52 FSWs
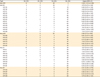
CI, confidence interval; CS, ThinPrep cervical smear; FSW, female sex worker; HPV, human papillomavirus; HR, high-risk; LR, low-risk; pHR, probably high-risk; UR, unknown risk; VA, vaginal Abbott swab.
![]()
As the main purpose of our study was to investigate the interchangeability of vaginal swabs and cervical smears for HPV testing, we calculated the sensitivity and specificity for vaginal swabs, using the results on cervical smears as the gold standard. The sensitivity and specificity were 100% and 70% for the detection of HR-HPV; 100% and 91% for pHR-HPV; 75% and 67% for LR-HPV; and 89% and 81% for UR-HPV.
Table 1 shows the level of agreement (kappa) between paired samples for each genotype and for each risk group [6]. Complete agreement between paired samples was achieved in only 27% of cases for all HPV genotypes; in 60% of cases for all HR-HPV genotypes; in 88% of cases for all pHR-HPV genotypes; in 60% of cases for all LR-HPV genotypes and in 83% of cases for all UR-HPV genotypes.
Paired analysis revealed that HPV positivity was often detected exclusively in VA samples, especially for non-HR genotypes (Fig. 2). In the light of HPV screening, however, equivalent detection of (p)HR-HPV genotypes is the key issue. When considering the HR and pHR groups combined, there was complete agreement between VA and CS. In contrast, for the non-HR groups combined, a substantial number of samples (36% [13/36]) was positive only in VA.
 | Fig. 2Paired analysis of HPV positivity for each risk group in VA and CS from 52 FSWs.
CS, ThinPrep cervical smear; FSW, female sex worker; HPV, human papillomavirus; HR, high-risk; LR, low-risk; pHR, probably high-risk; UR, unknown risk; VA, vaginal Abbott swab.
*Significant difference between VA and CS (p=0.039).
|
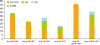
The mean number of genotypes identified in VA samples (mean=3.5; 95% confidence interval [CI]=2.8–4.2) was significantly higher than in CS samples (mean=2.6; 95% CI=2.1–3.0) (p=0.001) (Fig. 3). This difference was noticeable both in the HR-/pHR-HPV subgroup (2.4 in VA vs. 2.0 in CS [p=0.012]) and the LR-/UR-HPV subgroup (1.1 in VS vs. 0.6 in CS [p<0.001]). The most frequently encountered HR-HPV genotypes were HPV 16, 31, 51, and 52 (Table 1).
 | Fig. 3Number of HPV genotypes identified in paired VA and CS samples collected from 52 FSWs.
CS, ThinPrep cervical smear; FSW, female sex worker; HPV, human papillomavirus; VA, vaginal Abbott swab.
|
The 14 HR-HPV genotypes included in the Abbott HR-HPV assay are also covered by the INNO-LiPa assay, enabling comparison of the results of both assays for those genotypes. As we included paired samples (VA and CS) from 52 FSW, the Abbott and INNO-LiPa results of 104 samples could be compared. Overall, 11/104 analyses (11%) from 8 different FSWs showed discordant results for at least one of these 14 genotypes, in favor of INNO-LiPa: 7 VA samples and 4 CS samples showed the presence of at least one genotype with INNO-LiPa that was not detected with Abbott. The Abbott amplification curves of each discordant sample were examined, in order to detect any weak amplification signal below the assay cutoff. In summary, HPV 66 was missed 4 times (twice weak amplification signal and twice not detected); HPV 68 was missed 3 times (each time not detected); HPV 52 was missed twice (1 weak amplification signal and once not detected); HPV 58 was missed twice (each time not detected) and HPV 31, 51, and 18 were missed once (weak amplification signal). It should be noticed, however, that only 2/8 FSWs with discordant results had HSIL cervical cytology. Moreover, both FSW were positive for HPV 16 both with Abbott as with INNO-LiPa, reflecting the dubious relevance of the discordant results for the other HR-HPV genotypes.
Besides the 14 mutual HR-HPV genotypes, the INNO-LiPa assay detects 4 additional (p)HR-HPV genotypes: HPV 26, 53, 73, and 82. One should be aware that these additional genotypes are usually not included in assays currently approved for primary HPV testing [8]. Therefore, theoretically, HSIL cases with isolated positivity for one of these (p)HR-HPV genotypes could be missed. We explored the occurrence of such events in our dataset and found 23 FSWs to be positive for at least one of these genotypes. However, all but one of these FSW showed positivity for one of the 14 HR-HPV genotypes that are included in the Abbott assay as well. Only 1 FSW was positive for HPV 73 and negative for each of the 14 mutual HR-HPV genotypes. In case of primary HPV testing with the Abbott HR-HPV assay, this FSW would have been missed.
DISCUSSION
Within the studied population, we found a prevalence rate for HR-HPV of 51%, taking both positivity on vaginal swabs and cervical smears into account. When only considering the results on cervical smear, the gold standard, the prevalence falls back to 42%. This is lower than the number reported in a study conducted in the same Pasop vzw population between 1992 and 2001 (56%), and similar to other studies conducted worldwide in FSW (mean=41%; range=2%–100%) [910111213141516]. The prevalence rate in the general population is markedly lower, as reported in literature and estimated by the Centers for Disease Control and Prevention (CDC) (mean=24%; range=22%–27%) [91718].
The majority of FSWs (82%) showed NILM or ASC-US on cervical cytology, often (66%) with a negative result for HR-HPV. In contrast, the subgroup of FSW with LSIL or HSIL abnormity on cervical cytology (18% of FSW) was predominantly positive for HR-HPV (80%). Given the choice of the studied population, one could presume that a positive HPV result following recent sexual activity could be derived from the male partner, even when condoms are used [19]. Although a small study found no effect on HPV detection when vaginal intercourse occurred within 48 hours of self-sampling, further study is needed to evaluate the effect of vaginal intercourse on HPV screening and cervical cytology [20].
Cervical screening programs have not achieved adequate coverage of the populations at risk. In Belgium, for instance, the current screening coverage is only 59% in women 25 to 64 years old [21]. Even when screening is readily available, ignorance and fear of pelvic examination may create barriers. As multiple screening strategies include (primary) HPV testing, self-collection of vaginal samples instead of physician-collected cervical smears could increase the accessibility of screening. Indeed, multiple studies have suggested that vaginal self-sampling is an effective way to collect exfoliated cell specimens from the vaginal tract and cervix and is better accepted [322]. However, little is known on the clinical validity of (self-collected) vaginal samples, as vulvovaginal contamination could lead to the detection of more and other genotypes compared to the physician-collected cervical smears. Besides, the performance of HPV testing on self-collected samples is debatable. Arbyn et al. [23] conducted a meta-analysis to investigate the clinical accuracy of HPV testing on a self-sample in comparison with samples taken by a clinician in women attending cervical cancer screening. As both the pooled sensitivity and specificity were lower in self-samples vs. clinician-taken samples, they recommend sampling by a clinician to be retained in screening programs using signal-based assays. However, they suggest the use of HPV testing on a self-sample as an additional strategy to reach women not participating in the regular screening program. In studies comparing self-collected vaginal swabs with physician-collected cervical smears, vaginal swabs were more often positive and contained a greater number of genotypes compared to physician-collected samples [2425]. Our study confirms these findings. Complete agreement between paired vaginal samples and cervical smears was far from achieved and (mainly non-HR) HPV positivity was often detected exclusively in vaginal samples. Despite these divergences, most importantly, the sensitivity of vaginal swabs for the detection of HR-HPV and pHR-HPV was 100%, enabling vaginal swabs to serve as an acceptable sample for primary HPV testing. The suboptimal specificity (70% for HR-HPV and 91% for pHR-HPV), however, suggests the need of additional testing in case of HPV positivity, e.g., cervical cytology. Internal preliminary research (data not published) revealed that FSW with HR-HPV detected in the vaginal region only are likely to have normal cervical cytology results. As epidemiological data show that HPV infection is common and transient in 90% of cases within two years, with only a few individuals developing persistent infections, isolated HPV positivity in the vaginal region in the absence of abnormal cervical cytology should be interpreted carefully [2627]. Indeed, HPV detected in vaginal swabs could represent freshly infected vaginal cells, whether or not as a prelude of later cervical infection, rather than exfoliation from infected cervical cells. Besides, one should take into account that the cancer-causing effects of HPV are not limited to the cervix, but also vulvar and vaginal cancers are attributable to HPV [1].
We evaluated the concordance between Abbott HR-HPV RealTime PCR and INNO-LiPA HPV Genotyping Extra II, for the 14 HPV genotypes common to both assays in both vaginal swabs and cervical smears. Detection of most analyses was similar in 89% (83/104) of cases. In case of discordance, INNO-LiPa detected more genotypes than Abbott, suggesting an increased sensitivity of HPV DNA detection. However, the clinical relevance of these findings is debatable, as only 2 out of 8 FSWs with discordant results had HSIL cervical cytology and both of them were positive for HPV 16 with both assays as well. In addition, it should be noticed that the Abbott software uses clinical cutoffs which apply only to cervical smears, we examined the amplification curves of each discordant sample, in order to detect any weak amplification signal below this assay cutoff. In contrast to our findings, the previous version of the INNO-LiPA genotyping assay (INNO-LiPA HPV Genotyping Extra) showed a lower sensitivity compared to type-specific multiplex HPV PCR assays [28].
Besides the 14 HR-HPV genotypes included in both assays, INNO-LiPA detects 5 additional (p)HR-HPV genotypes. As these genotypes are not included in the assays currently approved for primary HPV testing, cases with isolated positivity for one of these genotypes could be missed. In our study, however, the only FSW who met these criteria had LSIL cervical cytology, reflecting the limited relevance of additional testing for these (p)HR-HPV genotypes.
The main purpose of our study was to explore the use of vaginal swabs instead of cervical smears for (primary) HPV testing. Though close consideration was given to the order in which samples were taken, the order was not altered during the study, whereby potential influences on the results cannot be fully excluded. However, it has been proven that the sampling order, the frequency of sampling and the interval between sampling do not influence HPV detection [24]. A second issue might be that vaginal swabs are not validated by Abbott for HPV testing, as clinical cutoffs derived from studies using cervical smears are applied when interpreting the results. We responded to this concern by manually inspecting the amplification curves in case of discordant results. Next, as FSW were included chronologically, follow up samples were only available by coincidence at varying time intervals. The lack of consistent follow up samples hampers unambiguous interpretation of the predominance of HPV positivity in vaginal swabs. At the moment, we cannot confirm that this positivity represents local infection or exfoliation of cervical cells. In analogy with current cervical cancer screening programs, we used the data of cervical cytology to give direction to cervical pathology instead of sampling for histology. However, this approach provides less accurate information on the true cervical pathology. Finally, as we studied a population of FSW, which are at higher risk for STI than the overall population, caution is to be made when generalizing our results to lower prevalence populations.
In conclusion, our study shows that vaginal swabs are equivalent to cervical smears for the detection of (p)HR-HPV in a population of FSW. As the vast majority of women might favor self-sampling over physician-sampling, vaginal sampling offers an opportunity to boost screening coverage. However, the clinical accuracy of HPV on self-collected samples needs to be further documented in larger clinical trials, following females over a long period. In the meantime, cytological data are unbearable to interpret the clinical value of (probable) HR-HPV positivity.
 XML Download
XML Download